Autonomic assessment
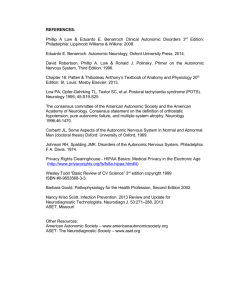
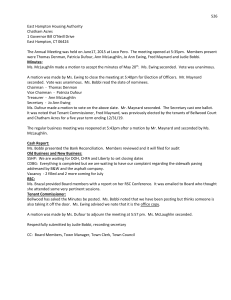
advertisement

Supplementary material Formal vestibular assessment Vestibular failure was defined as a gain ratio of (angular velocity of eye movement)/(angular velocity of head movement) 80ms after onset of head impulse of less than 0.79 (2 standard deviations less than mean in our 60 historical controls aged 20-80 years) (Mossman et al., 2012) or by peak slow phase velocity of the nystagmus on bithermal caloric testing of less than 20°/s summated over the four irrigations (Kim et al., 2011). Autonomic assessment Autonomic testing The protocol used for autonomic function assessment was adapted from Ewing et al for the diagnosis of diabetic autonomic neuropathy (Ewing and Clarke 1982; Ewing et al., 1985). The tests assessed both parasympathetic and sympathetic functions and a detailed description of the procedures is provided below. Parasympathetic function Each patient had continuous ECG monitoring for heart rate variation during Valsalva manoeuvre, deep breathing and on standing. Valsalva ratio For the Valsalva manoeuvre each patient was asked to blow forcefully to maintain a pressure equivalent to 40 mmHg on a sphygmomanometer for 15 seconds. The patient was allowed to rest for 1 minute before repeating the Valsalva manoeuvre. This was performed three times and the R-R intervals during the Valsalva manoeuvre and in the rest period were measured. The Valsalva ratio was calculated by dividing the maximum R-R interval following Valsalva manoeuvre with the minimum R-R interval during Valsalva. The mean ratio of the three attempts was calculated. (Ewing and Clarke 1982; Ewing et al., 1985) Heart rate variation during deep breathing During this manoeuvre the patient was asked to breathe deeply over 10 second cycles for one minute with continuous ECG rhythm recording. The maximum and minimum R-R intervals during each cycle were recorded to enable calculation of the maximum and minimum heart rates. The heart rate in beats per minute was calculated by dividing 60 by the R-R interval. The difference between maximum and minimum heart rates during each cycle was calculated and the mean difference of the six cycles was obtained. Heart rate variation on standing The patient was asked to stand up from a resting supine position without aid. The shortest R-R interval around the 15th heart beat (R-R 15) and the longest R-R interval around the 30th heart beat (R-R 30), after assuming the standing position, were measured. The 30:15 ratio was calculated as R-R 30 / R-R 15. Sympathetic function: Postural blood pressure and blood pressure response to handgrip were measured. Postural blood pressure was measured after the patient had lain supine for 2 minutes and after at least 1 minute of standing up. The systolic blood pressure difference between lying and standing was measured. If two or more readings were obtained the average difference was recorded. To assess blood pressure response to handgrip, the patient was asked to grip at 30% of maximum on a sphygmomanometer bulb and to maintain this for 5 minutes. Three resting blood pressure measurements were obtained prior to handgrip. During handgrip blood pressure was measured at one-minute intervals. Blood pressure response to handgrip was measured as the difference between the mean pre-handgrip diastolic blood pressure and the maximum diastolic blood pressure obtained during handgrip. Interpretation of autonomic tests Each autonomic test (other than the Valsalva ratio which does not have a borderline range) has a defined normal, borderline and abnormal range as described in Ewing and Clarke’s classification of autonomic test results (Ewing and Clarke 1982; Ewing et al., 1985). We ascribed a score of zero for normal, one for borderline and two for abnormal. With minor modification to the Ewing classification, we defined definite parasympathetic dysfunction as a score of ≥ four (equivalent to at least two abnormal, or one abnormal and two borderline results) and definite sympathetic dysfunction as a score of ≥ two (at least one abnormal or two borderline) results. In a series of 71 normal controls studied by Ewing et al (age range 16 - 69) only one control subject had an abnormal result using this battery of tests (one subject had a 30:15 ratio of 1.0). (Ewing et al., 1985) Imaging analysis for focal cerebellar atrophy and association with downbeat nystagmus Methods: The neuroradiologists assessed four cerebellar areas for atrophy: the ventral vermis, the dorsal vermis and the cerebellar hemisphere crus I – which have been identified as showing atrophy in CANVAS (Szmulewicz et al., 2011) - and the floccular complex which has been associated with DBN (Pierrot-Deseilligny and Milea 2005). The vermis and flocculus were assessed using freehand outlining of the areas and standard MRI software to calculate the enclosed area, following the method of Webb et al. (Webb et al., 2009) For crus I we used the ratio on sagittal T1 at the level of the flocculus of maximum craniocaudal thickness of crus I: maximum thickness of horizontal fissure (supplementary fig. 1). Inter-rater reliability of MRI measurements was assessed using the ICC (intraclass correlation coefficient). Results: Twenty-three scans were available for assessment of focal atrophy. There was reasonable inter-rater agreement for measurements of the anterior, dorsal and inferior vermis and for the ratio of crus I to the horizontal fissure (ICC coefficients 0.78, 0.70, 0.68, 0.65, respectively), but the measurement of the area of the flocculus was not reliable (ICC coefficient 0.34), likely due to its small size and highly irregular outline. Sixteen of these patients had DBN and seven did not. Average measured size of all four regions was slightly smaller in the DBN subgroup, but no clear association with atrophy of any particular area of the vermis or crus I was seen (p values for anterior vermis, 0.11; dorsal vermis, 0.47; inferior vermis, 0.36; and crus I, 0.15). Generally there was increased atrophy with increased disease duration, but this was only statistically significant for crus I atrophy (p < 0.001). There was no correlation between the degree of atrophy and age. References: Ewing, D. J. and Clarke, B. F. (1982), 'Diagnosis and management of diabetic autonomic neuropathy', Br Med J (Clin Res Ed), 285 (6346), 916-8. Ewing, D. J. et al., (1985), 'The value of cardiovascular autonomic function tests: 10 years experience in diabetes', Diabetes Care, 8 (5), 491-8. Kim, S. et al., (2011), 'Bilateral vestibulopathy: clinical characteristics and diagnostic criteria', Otol Neurotol, 32 (5), 812-7. Mossman, B. et al., (2012), 'Normal horizontal VOR gain with video-oculography (EyeSeeCam VOG). ', Poster presented at: the 27th Barany Society Meeting, Uppsala, Sweden June 10-13. Pierrot-Deseilligny, C. and Milea, D. (2005), 'Vertical nystagmus: clinical facts and hypotheses', Brain, 128 (Pt 6), 1237-46. Szmulewicz, D. J. et al., (2011), 'Sensory neuropathy as part of the cerebellar ataxia neuropathy vestibular areflexia syndrome', Neurology, 76 (22), 1903-10. Webb, S. J. et al., (2009), 'Cerebellar vermal volumes and behavioral correlates in children with autism spectrum disorder', Psychiatry Res, 172 (1), 61-7. Figure Legend Figure 1: 1a - Representative mid-sagittal measurement of vermal subregions: lobules regions I – V (superior enclosed region), VI-VII (mid-posterior region), VIII-X (inferior region). 1b – Measurement of the flocculus and relative atrophy of Crus I as measured by ratio calculated by maximum Crus I craniocaudal thickness / maximum thickness of horizontal fissure.