ICD-10 SC Physician Letter
advertisement

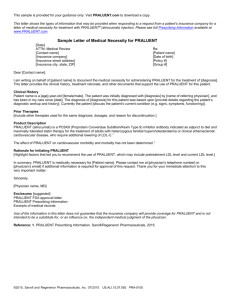
Dear Dr. Your patient is a participant of Home and Community-Based Services (HCBS) offered through the Department of Human Services (DHS). The goal of these services is to allow individuals with physical disabilities, developmental disabilities and/or traumatic brain injury to remain in their homes. These programs provide services including, but not limited to, assistance with personal care, health maintenance activities, transfers, meal preparation, grocery shopping, laundry, errands and light housekeeping in order to maintain a person’s health, safety and independence in the community. All Service Coordination Entities and service providers who provide HCBS services to participants through OLTL waiver/programs will require an ICD-10 diagnosis code to bill for services rendered effective October 1, 2015. In order to assist with obtaining the required ICD-10 diagnosis code for HCBS, the attached Physician Certification form needs to be completed to ensure that your patient’s HCBS records and DHS system data contain the appropriate ICD-10 diagnosis code information. Please complete ALL of the following sections: PRIMARY PHYSICAL DIAGNOSIS (please include diagnosis of Traumatic Brain Injury and/or Developmental Disability if present) DX Code (ICD 10 code is REQUIRED) Level of Care (select all that apply) Long term or Short term Physician signature (Attending physician not CRNP, MT,INTERN, RESIDENT OR RN Print Physician Name Physician License # or MAID # Physician phone and fax Date Please complete, sign, and fax the form to ________________________________________________________________within 5 days of receipt. Once this form is completed and returned, your patient’s information will be entered into the appropriate DHS systems. Sincerely, (SC PROVIDER NAME) (SC PROVIDER ADDRESS) (SC PROVIDER CITY, STATE, ZIP) (SC PROVIDER TELEPHONE) (SC PROVIDER FAX #) (SC PROVIDER EMAIL ADDRESS)