Travel Clinic - Antimalarial drugs and side effects
advertisement

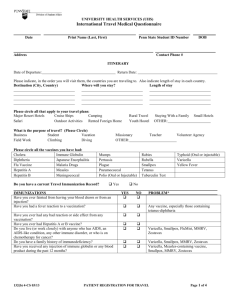
Antimalarial Drugs & Common Side Effects It is important to note that no oral antimalarial agent is 100% effective and therefore it is important to practice bite avoidance as well (impregnated nets, insect repellents, clothes etc). Any high body temperature lasting longer than 12 hours should be reported. Chloroquine Minor side effects such as stomach upset and blurred vision occur frequently. These can be lessened by taking tablets with food, or taking half the dose on 2 occasions each week. They are safe in pregnant women and children in correct doses. Pruritus (itch) in dark skin individuals is common. If you have had generalised psoriasis, chloroquine and other chloroquine-like drugs, including primaquine, quinidine and proguanil should be avoided. Retinal changes including eye damage and blindness may occur after prolonged use but on the usual 300mg per week dose it would take 6-7 years. Malarone A combination of atovaquone and proguanil in a single tablet, it is a new addition for malaria prevention. It’s use has been approved for treatment and prevention of malaria since November 2001. It is particular useful where malaria is resistant to chloroquine and mefloquine (Larium). On evidence to date, it appears to be very safe and effective, but is expensive. For the prevention of malaria, Malarone is taken once a day, starting 2 days before entering malarial risk areas and continuing for 1 week after leaving the malarious area. It should be taken with food and milk. This regime is simple and suited to business and frequent travellers. NB – when malarone is used for malaria prevention, side effects are uncommon. However nausea, vomiting, abdominal pain and diarrhoea occur when higher doses of the drug are used for treatment. Convulsions and rash have rarely been reported. Doxycycline It is an alternative to mefloquine for short-term travellers. Doxycycline at 100 mg/day is approved for a period of up to 8 weeks only but is probably safe for longer use. Side effects include thrush, stomach and bowel upsets (particularly if medication is taken on an empty stomach) and sunlight sensitivity. The exaggerated sunburn reaction may be minimised by avoidance of sunlight, using sunscreen and taking the drug in the evening. Drinking copious amounts of water after swallowing the drug is recommended to reduce heartburn. Using Doxycycline may make the contraceptive pill unreliable. The Therapeutic guidelines 2002 states that: “A second form of contraception is not necessary but may be offered” & “women who develop breakthrough bleeding might consider using barrier methods for the duration of antibiotic therapy”. Discuss this matter with your doctor. Mefloquine Side effects (‘Larium’) Minor side effects such as nausea, vomiting, heartburn and loose stools occur in about 20% of users, but this is no more frequent than with other antimalarials and usually subside with continued use. Taking ½ tab twice a week with food, and drinking copious water with medical will help reduce these. Unfortunately, mefloquine frequently produces annoying adverse neurological effects such as insomnia, vivid dreams, dizziness, mental clouding, anxiety and coordination problems. These are sufficient to interfere with daily activities in up to 10% of users and are probably aggravated by use of alcohol and cannabis. Disabling side effects sufficient to recommend the cessation of mefloquine occur in 0.5% of users. However despite this, some 5-10% of users will stop the Dr Mittal & Partners – Travel Vaccination Clinic Antimalarial Drugs & Common Side Effects drug. Consequently, any person requiring a clear mind and good co-ordination should not use mefloquine. This may involve travellers to high altitude and definitely those contemplating aqualung (scuba) diving. Other contra indications include persons with a history of seizures, neuro-psychiatric disorder, the first three months of pregnancy and those with cardiac conduction problems. Women are advised to use contraceptives during and for 3 months after administration of mefloquine. Mefloquine is probably best commenced 2 ½ weeks before entering a malarious area as it takes this long to build up to satisfactory blood levels (half-life of 21 days). Also this provides time to detect those travellers that develop unacceptable side-effects and thus enable a change in medication. Commencing 1 or 2 weeks before departure is not adequate. A recent report involving soldiers taking mefloquine 250mg daily for 3 days to enable a quick build up in blood levels was surprisingly well tolerated. US authorities are prepared to use mefloquine for up to 2 years continuously in Peace Corps Volunteers overseas. Serious neuropsychological side effects can occur when mefloquine is used in high doses. Proguanil One of the safest antimalarial drugs. Mouth ulcers is an annoying complication in up to 37% of travellers (when taking with Chloroquine). Proguanil is taken 2 tablets daily, starting 1 day before entering malarial area and continuing for 4 weeks after leaving the area. Chloroquine is taking 2 tablets weekly – confusing your tablets could be deadly. Contrary to WHO recommendations, Australian travel physicians mostly limit the use of Chloraquine + Proguanil, to travellers unable to take mefloquine or doxycycline. Dr Mittal & Partners – Travel Vaccination Clinic