Commitment to Change and CME
advertisement

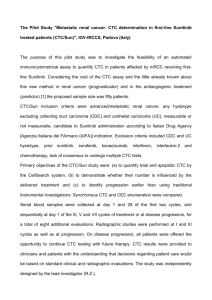
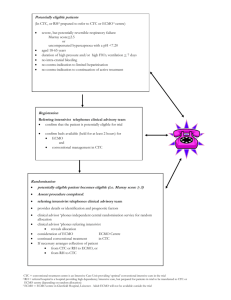
Mesiha Final Essay Commitment to Change and CME As healthcare providers we are all aware of the importance of lifelong learning, evidence based medicine and best practices, for patient care and outcomes. Among the most common learning activities post residency, are the CME conferences. According to the medical literature, traditional medical education is effective in the transfer of knowledge and skills, yet is inadequate in changing behavior. Physicians report spending about 50 hours per year in continuing medical education activities. These activities are geared toward improving and optimizing patient outcomes. There is an underlying belief associated with CME activities that health care professionals will improve how they practice, which will in turn improve patient outcomes. Despite this belief, many studies have demonstrated a lack of effect from formal CME (Davis, 1999). From these and other reports in the literature, it is becoming clear that formal CME programs with little interaction improve knowledge and skills but do not change behavior. Yet, the majority of CME-accredited programs continue to be didactic lectures whether live or via the Internet. Research into the adult learning and medical literature identified effective techniques that lead to behavior change. A combination of interactive tactics such as problem-based learning and simulation, along with reinforcement strategies such as “commitment to change” instruments and follow-up reminders, must be incorporated into the design of educational programs in order to successfully change the behavior of the learner. Studies have shown Physicians who make a commitment to change their practice behavior are more likely to make changes than those who do not. In order to achieve behavior change, which leads to change in outcome, effective learning methodologies and Reinforcement strategies should be used. I think commitment to change (CTC) is one of the valuable intervention that can be implemented as a reinforcement strategy. There are several venues where the concept of CTC can be applied and used as a valuable tool, in my Institution. In regards to our fellows in Training: 1- During their biannual review, currently the fellows have a chance to reflect on their training, weaknesses, strength and the feedback they received (from faculty, 360 evaluations..). Fellows will be writing a CTC in one or two points, able to review it in 6 months and self-report change. Subsequent evaluations can also be used as a way to document a change if applicable. 2- CTC can be implemented after Morbidity and Mortality Conference, that can involve both fellows and faculty. Reminders will be sent every 6 months, with questionnaire/self-reporting the change. In regards to Faculty Development o Our program has been implementing a Faculty Development Program for almost a year. Plan to implement CTC in these sessions. In this case, I might choose a predefined lecturederived commitments versus CTC statements made spontaneously or a combination of both. I think the key in all cases would be the reminder, self-reporting of change to enhance the process and impact behavior and outcome change.