FQ 4 dizziness - Ipswich-Year2-Med-PBL-Gp-2

DIZZINESS
‘Dizziness’ can be used to describe many different phenomena
Other terms may be used to describe the same sensation:
‘giddiness’
‘swimming in the head’
‘my brain spinning’
‘whirling’
‘swinging’
Vertigo is defined medically as ‘a sudden sense of movement’, and used to describe a hallucination of rotation of self or the surroundings in a horizontal or vertical direction.
Classification of dizziness vertigo dizziness giddiness or lightheadedness fainting or syncopial episodes pseudovertigo disequilibrium
Vertigo
An episodic sudden sensation of circular motion of the body or of its surroundings. Some terms used by the patient to describe this symptom include:
‘everything spins’
‘my head spins’
‘the room spins’
‘whirling’
‘reeling’
‘swaying’
‘pitching’
‘rocking’
Vertigo is characteristically precipitated by standing or turning the head or by movement. Patients have to walk carefully and may become nervous about descending stairs or crossing the road and usually seek support. Thus the vertigo patient is usually very frightened and tends to remain immobile during and attack.
True vertigo is a symptom of disturbed function involving the vestibular system or its central connections. It invariably has an organic cause.
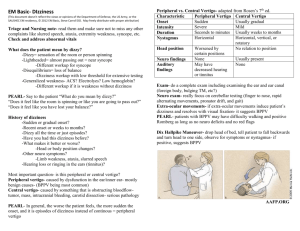
INSERT FIGURE 46.2 FROM MURTAGH
Causes of vertigo
Peripheral disorders
Central disorders
Labyrinth
Labyrinthitis: viral or suppurative
Meniere’s syndrome
Benign paroxysmal positional vertigo (BPPV)
Drugs
Trauma
Chronic suppurative otitis media
8 th nerve (vestibulocochlear)
Vestibular neuronitis
Acoustic neuroma
Drugs
Cervical vertigo
Brain stem
Vertebrobasilar insufficiency
Infarction
Cerebellum
Degeneration
Tumours
Migraine
Multiple sclerosis
Giddiness
sensation of uncertainty or ill-defined light-headedness
other terms used: o ‘swimming sensation’ o ‘walking on air’ o ‘ground going beneath me’
usually contains no elements of rotation, impulsion, tinnitus, deafness, nausea or vomiting
patient with giddiness can walk without difficulty if forced to do so
(although they may be fearful of falling)
giddiness usually a psychoneurotic symptom
Syncopal episodes
may present as a variety of dizziness or light-headedness where there is a sensation of impending fainting or loss of consciousness.
Common causes are o cardiogenic disorders o postural hypotension (usually drug induced)
Disequilibrium
Implies a condition with a loss of balance or instability while walking, without any associated sensations of spinning o Terms used to describe this include:
‘unsteadyness on feet’
‘staggers’ or ‘swaying feeling’
Disequilibrium is usually of neurogenic origin
DDx of dizziness/vertigo
Probability diagnosis Anxiety – Hyperventilation (G)
Postural hypotension (G/S)
Simple faint – vasovagal (S)
Ear infection – acute labyrinthitis (V)
Vestibular neuronitis (V)
Benign paroxysmal positional vertigo
(V)
Motion sickness (V)
Post head injury (V/G)
Cervical dysfunction/spondylosis
Serious disorders not to be missed Neoplasia
acoustic neuroma
posterior fossa tumour
other brain tumours (primary or secondary)
Intracerebral infection (eg. abcess)
Cardiovascular
arrhythmias
myocardial infarction
Often missed (pitfalls)
aortic stenosis
Cerebrovascular
vertebrobasilar insufficiency
brain stem infarct, eg. PICA thrombosis
Multiple sclerosis
Ear wax – otosclerosis
Arrhythmias
Hyperventilation
Alcohol and other drugs
Cough or micturition syncope
Vertiginous migraine
Parkinson’s disease
Meniere’s syndrome
Possible Masquerades
Depression
Drugs o Alcohol o Antibiotics: streptomycin, gentamicin, kanamycin, tetracyclines o Antidepressants o Antiepileptics: phenytoin o Antihistamines o Antihypertensives o Aspirin and salicylates o Cocaine o Diuretics in large doses: intravenous frusemide, ethacrynic acid o Glyceryl trinitrate o Quinine-quinidine o Tranquillisers: phenothiazines, phenobarbitone, benzodiazepines
Anaemia
Spinal dysfunction
Less likely o Diabetes o Thyroid disorder o UTI
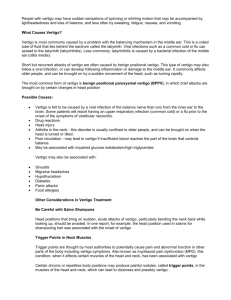
Meniere syndrome
Caused by a build-up of endolymph
Commonest in 30-50 yrs age group
Characterised by paroxysmal attacks of vertigo, tinnitus, nausea and vomiting, sweating and pallor, deafness (progressive)
Onset is abrupt
Attacks last 30 minutes to several hours
There is a variable interval between attacks (eg. Twice a month to twice a year)
Nystagmus is observed only during an attack
Dizziness in emergency medicine
ECG can help to determine a cardiac cause
AMI, acute ischaemia, unstable angina or acute coronary syndrome can cause syncope
FATIGUE
Ddx
Probability diagnosis
Serious disorders not to be missed
Often missed (pitfalls)
Stress and anxiety
Depression
Viral/postviral infection
Sleep-related disorders (eg. Sleep apnoea)
Malignant disease
Cardiac arrhythmia (eg. Sick sinus syndrome)
Cardiomyopathy
Anaemia
Hidden abcess
Haemochromatosis
HIV infection
Hepatitis C
‘Masked’ depression
Food intolerance
Coeliac disease
Chronic infection (eg. Lyme disease)
Incipient CCF
Fibromyalgia
Lack of fitness
Drugs: alcohol, prescribed, withdrawal
Menopause syndrome
Pregnancy
Neurological disorders:
Post-head-injury
CVA
Parkinson disease
Kidney failure
Metabolid (eg. Hypokalaemia, hypomagnesaemia)
Chemical exposure (eg. Occupational)
Rarities:
Hyperparathyroidism
Addison disease
Cushing syndrome
Narcolepsy
Masquerades
Depression
Diabetes
Drugs
Anaemia
Thyroid disease
Spinal dysfunction
UTI
Multiple sclerosis
Autoimmune disorders