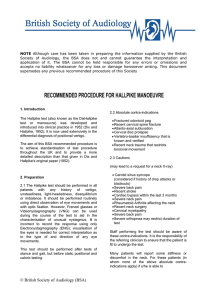
View
advertisement

DIZZINESS IN AN OLDER ADULT 10/12/05 MARY JO WILLIS MS, APRN, BC CLINICAL PROFESSOR NURSE PRACTITIONER I have no financial interest to report OBJECTIVES Review common causes of dizziness/vertigo Describe clinical pearls of vertigo testing/treatment Discuss the issues of vertigo testing THE CASE 79 year old with Hx postural hypotension Sudden onset of dizziness 2 weeks ago Two more episodes since that time THE PATIENT PMH: Macular degeneration, BPH, anemia, polymyalgia rheumatica SH: Retired, non-smoker, no ETOH FH: No Meniere’s disease ROS: No changes in hearing, vision, speech; no fall, head injury, weakness/ paralysis of extremities, LOC, or recent URI THE PATIENT Medications: – Prednisone – Terazosin – Ferrous sulfate – TMP-Sulfa DS – Ocuvite DIZZINESS IN THE ELDERLY Cannot place dizziness into one category – Disequilibrium can accompany other types of dizziness when intact compensatory systems are absent – Need to distinguish between primary symptom and secondary causes – Need to distinguish acute from chronic dizziness-no consensus Sloane et. Al., (2001) CATEGORIZING DIZZINESS Pre-syncope Syncope Disequilibrium Psychogenic Vertigo PRESYNCOPE Sense of impending fainting or LOC Episodic diffuse temporary cerebral ischemia Sweating, pallor, telescoping of peripheral vision SYNCOPE Syncope: sudden transient loss of consciousness with concurrent loss of postural tone Multi-system causation Most common causes are vasovagal episodes or orthostatic hypotension DISEQUILIBRIUM Disequilibrium: Perceived postural instability involving legs and trunk without head sensation Overlap between imbalance and disequilibrium Vertigo not present PSYCHOGENIC Dizziness that cannot be readily classified into previous categories No focal or PE findings Chronic Common Mechanisms – Hyperventilation – GAD, Major depressive disorder – Somatization disorders – Substance abuse VERTIGO Illusion of motion interpreted as self movement or environmental movement Rotating with spinning sense of falling or swaying back and forth: Merry-Go Round Effect 1/2 of patients with dizziness have vertigo ETIOLOGY OF VERTIGO Asymmetry of the vestibular system due to pathology involving: – Labyrinth and vestibular nerve(40%) – Central vestibular structures in brainstem (10%) – Remaining 50% are conditions noted earlier VERTIGO Time course Provoking factors Associated symptoms Prior risk factors PERIPHERAL VESTIBULAR DYSFUNCTION Labyrinthitis (vestibular neuronitis) Meniere’s Disease Trauma Tumors (Acoustic Neuroma) Benign Paroxysmal Positional Vertigo PERIPHERAL VERTIGO Acute Viral Labyrinthitis /Vestibular Neuronitis – Usually preceded by a viral respiratory or GI infection – Sudden onset of nausea, vomiting, severe vertigo worsened by change in position – Can last for days to weeks – Nystagmus may last for months PERIPHERAL VERTIGO Meniere’s (Endolymphatic Hydrops) – Spontaneous onset/recurrent attacks – Duration of symptoms: min- hrs – Often preceded by tinnitus, ear fullness – Sensori-neuro hearing loss which varies day to day – Chronic recurrent PERIPHERAL VERTIGO Drugs (www.annuls.org) Appendix (41-44) Trauma Acoustic Neuroma: Vestibular Schwannoma – Account for < 1% of patients – Disequilibrium is more likely – Gradual rather than acute onset The Patient Episodes occurred when he was lying down and turned over to his left side Slightly nauseated-no vomiting Reports that the room is spinning Last about “10 minutes” Getting into an upright position helps DIZZY HISTORY Key questions: Describe the first episode – Objects spinning/turning around you – Occur in attacks – Position change makes you dizzy – Can you tell when it may start – Can you stand unsupported – What will stop the dizziness, make it better or worse THE PATIENT Afebrile, No postural hypotension In NAD, cognition appropriate HEENT: WNL Neck: no carotid bruits CV: bradycardia, irregular rhythm Lungs: WNL NEURO EXAM Neuro: CN 2, 5,7,8-12 intact No nystagmus with EOMs Romberg/cerebellar tests intact DTRs. Sensation intact BENIGN PAROXYSMAL POSITIONAL VERTIGO Vertigo with head movements Brief episodes lasting < 1 minute; nausea Usually no tinnitus or hearing impairment Spontaneous nystagmus is not present Usually self-limited; can persist for weeks BPPV Most common form of positional vertigo No predilection based on gender, race or age but usually after 4th decade Provoked by specific head movements Typically have no other neurological complaint May have history of head trauma CANALITHIASIS Loose otoconia consisting of calcium carbonate crystals from the utriculus Usually involve the posterior semicircular canal Causes inappropriate movement of endolymph Giving an erroneous spinning sensation with head movement BPPV ETIOLOGY CANALITHIASIS CANALITHIASIS DIAGNOSTIC CRITERIA Vertigo w mixed torsional/vertical nystagmus on Dix Hallpike Latency of 1-2 seconds from completion of test and onset or vertigo/nystagmus Paroxysmal provoked vertigo and nystagmus (increase then decline over 10-20 seconds) Fatigability if test repeated Furman (1999).NEJM: November 18, pp1590-1596 Clinic Testing Dix Hallpike maneuver Sensitivity from 50-88%* Purpose is to: – replicate the symptoms – elicit positional nystagmus – to determine whether nystagmus is fatigable *Hoffman, RM., et.al.(1999) DIX HALLPIKE MANEUVER The patient is positioned in front of the examiner with their head turned to the side at 45 degree angle The examiner supports the head and shoulder, then quickly brings patient to a reclining position with head rotated to one side and hanging over the table The position is maintained for 30 sec DIX HALLPIKE MANEUVER Tell patient not to fixate vision Look for nystagmus, noting time of onset, direction – Nystagmus upward and torsionally with upper poles of eyes beating toward the ground-last ~20-30 seconds – Once sitting, nystagmus will recur but in the opposite direction – Repeat to same side, repetition diminishes the intensity and duration DIX HALLPIKE MANEUVER DIX HALLPIKE FRENZEL LENSES THE PATIENT Nystagmus elicited Vertigo elicited-lasted for few seconds Symptoms absent after sitting upright ISSUES Self limiting disorder Diagnosed by history-do we need to do Dix Hall pike Dix Hallpike may interfere with treatment using the Epley test When does patient need Canalith repositioning? TREATMENT Epley maneuver: – Relocate the debris from the posterior semicircular canal to the vestibule – 80% success rate after one treatment and 100% after >1 (Epley) – 89% success rate after one treatment compared to 23% in untreated group (Lynn) – Recurrence rate of 30% in 30 month F/u period; 15% over 4 years (Epley) Lynn(1995) CANALITH REPOSITIONING Home treatments with modified pocedures Modified Semont – Less effective than modified Epley (95 vs 58% Brandt-Daroff – Less effective than modified Epley (64% vs 23% THE PATIENT No further episodes Avoids turning to left side while supine References Froehling, D.A., et.al.,(2000). The canalith repositioning procedure for the treatment of benign paroxysmal positional vertigo: a randomized controlled trial. Mayo Clin Proc 75:695 Furman, J.M. et.al(1999). Benign paroxysmal positional vertigo. NEJM, 341(21), pp.1590-96. Kroenke, K. et.al., (200). How common are various causes of dizziness? A critical review. South Med. J.,93: 160-7. Lynn, S. et.al.,(1995). Randomized trial of canalith repositioning procedure. Otolaryngol Head Neck Surg. 113:712 Sloane, P.D., et.al.(2001). Dizziness: State of the Science. Annuls of Internal Medicine 134(9) part 2, pp. 823-31