Erythema Migrans (EM) Decision Support Tool
advertisement
 Decision Support Tool")
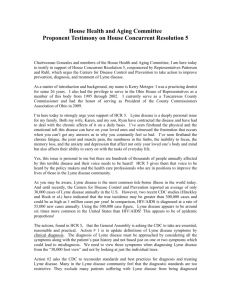
Erythema Migrans (EM) Decision Support Tool For use in assisting in the identification and diagnosis of Erythema Migrans Erythema migrans is the earliest clinical manifestation of Lyme borreliosis (LB), which has the potential to develop into disseminated borreliosis, if untreated. This decision support tool (DST) is intended as an aid to diagnosis of erythema migrans (EM). Other manifestations of LB are not dealt with here. Background EM is the initial, and most prominent feature of early dermatological of Lyme borreliosis and represents the body’s early response to exposure to Borrelia. EM is essentially a clinical diagnosis and this Decision Support Tool (DST) is intended as an aid in the diagnosis of EM. Under S.I. No. 452 of 2011 (The Infectious Diseases [Amendment] Regulations 2011), Lyme disease has been included in the Schedule of Diseases that require to be notified to the local Director of Public Health by the attending Physician who diagnoses the infection, or by the Laboratory Director in whose laboratory the diagnosis is confirmed. Under the current case definition for Lyme disease, only cases of neuroborreliosis are required to be notified; there is no requirement to report individual cases of EM, or other forms of borreliosis. In a number of countries (notably Scotland) all cases of LB are statutorily notifiable. In 2010 there were 308 cases of LB in Scotland (giving an incidence rate of 5.9/100,000 population while in England and Wales, 973 cases of LB (including 173 people or 18% travel related cases) were identified, giving an incidence rate of 1.79/100,000 population. The true burden of LB is unknown in Ireland, but were the incident rate to be halfway between that of England & Wales, and Scotland at 3 cases/100,000 population, then we could expect 120-150 cases per annum (this compares with an estimated burden in Austria of 14,000 cases per annum, giving an annual incidence rate of 130/100,000 population and the Netherlands, which has an annual incidence of EM of approximately 133 cases/100,000 population). It is estimated in the US that only about 70% of cases of Lyme disease present with EM (this is about the same for adults and children). This figure is somewhat higher in Europe; in a series of European studies, EM was shown to occur as the presenting sign in about 90% of patients with Lyme borreliosis and can be accompanied by “viral-like” (“flu-like”) symptoms including myalgias and arthralgias without significant respiratory involvement. Between five and eight percent present as neuroborreliosis (The epidemiology, prevention, investigation and treatment of Lyme borreliosis in United Kingdom patients: A position statement by the British Infection Association: British Infection Association). If untreated, borrelial spirochetes can disseminate and cause early neuroborreliosis (in between 316% of cases).1,2 One Irish series with small numbers identified a neuroborreliosis rate of 50%.3 (The Clinical Spectrum of Lyme Neuroborreliosis M Elamin, T Monaghan, G Mulllins, E Ali, G Corbett-Feeney, S O†™Connell, TJ Counihan); this would be considerably higher than more extensive series in Europe and the US. HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Although more common in Europe, facial nerve palsy is found in 3% to 5% of all children with Lyme disease in the United States.4 Meningitis occurs in 2% to 12% of children with LD.5 Data from the Netherlands provides an interesting population-level view of LB. In a Dutch study with 167 tick bite cases in a GP population, only one case (0.7%) developed Lyme borreliosis upon followup serology. Notably, this tick was attached longer than 24 hours. In general, ticks attached for less than 24 hours do not transmit Borrelia.6 In general, erythematous skin lesions smaller than 5 cm starting within two days after detachment of the tick are most likely a tick bite hypersensitivity reaction and these reactions should resolve within one to two days (Coumou et al 2011). In the US, in highly endemic areas, one case of LB is estimated to be prevented for every 50 individuals treated prophylactically with antibiotics. However, as asymptomatic infection is thought to be much more frequent in Europe than in the US, this argument would not appear to be as strong in European LB cases. However, in highly endemic areas of the Netherlands and the tick was known to have been attached for longer than 24 to 48 hours, and the patient presents within three days following the tick bite, Dutch authorities state that use of prophylactic doxycycline (200 mg stat) is be considered.6 The early manifestation of LB is the pathogonomic EM. Typical EM presents as an expanding, circular erythematous skin lesion with central clearing centred at the site of tick bite that begins after three to 30 days (median seven to 14 days) that varies in diameter from five to 75 cm (median 15 cm). The skin rash can be accompanied by systemic symptoms (i.e. fever, myalgia, arthralgia) and local symptoms (itching, burning, mild pain). Very occasionally following European exposure, and most commonly in children, a bluish red tumour-like skin infiltrate, often found on the earlobe or nipple may appear – this is a borrelial lymphocytoma. In typical European series, In Europe, 77 to 89% of all Lyme manifestations are erythema migrans and 2 to 3% are borrelial lymphocytoma.6 Identification of EM in Irish Patients A significant minority (as many as 10-20%) of LB patients will not present with EM and are likely to present at a later stage. The following images are intended to provide an overview of the many different presentation of EM to General Practice. Tick bites are most likely to occur on the thinner skin found in skin folds and around the ears of children, but the following images show that EM following tick bite can occur anywhere on the body. Image HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Description Irregular EM Rash Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie EM Rash on a child’s upper chest Typical bull’s-eye EM rash on a child’s torso Fading EM Rash HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Irregular, faint EM rash EM rash at the nipple Older, fainter EM rash on leg Very faint EM rash, child’s buttock HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Typical bull’s-eye EM rash Extensive EM rash on the shoulder Flexural EM Rash, elbow HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie “Burnt” EM rash, thigh Non-bulls-eye rash, flank of young woman Extensive EM rash, hip and abdominal wall HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Atypical EM rash, foot Atypical EM rash, face HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Atypical EM rash, child EM Rash, child’s shoulder HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie Multiple EM rashes – very unusual EM rash, bulls-eye difficult to make out Images courtesy of EUCALB and Dermis.net HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie References 1. Berglund J, Eitrem R, Ornstein K, Lindberg A, Ringér A, Elmrud H, Carlsson M, Runehagen A, Svanborg C, Norrby R. An epidemiologic study of Lyme disease in southern Sweden. N Engl J Med. 1995 Nov 16;333(20):1319-27. 2. Huppertz HI, Böhme M, Standaert SM, Karch H, Plotkin SA Incidence of Lyme borreliosis in the Würzburg region of Germany. Eur J Clin Microbiol Infect Dis. 1999 Oct;18(10):697-703. 3. Elamin M, Monaghan T, Mulllins G, Ali E, Corbett-Feeney G, O'Connell S, Counihan TJ. The clinical spectrum of Lyme neuroborreliosis. Ir Med J. 2010 Feb;103(2):46-9. 4. Gerber MA, Shapiro ED, Burke GS, Parcells VJ, Bell GL. Lyme disease in children in southeastern Connecticut. Pediatric Lyme Disease Study Group. N Engl J Med. 1996 Oct 24;335(17):1270-4. 5. Garro AC, Rutman M, Simonsen K, Jaeger JL, Chapin K, Lockhart G. Prospective validation of a clinical prediction model for Lyme meningitis in children. Pediatrics. 2009 May;123(5):e829-34. 6. Coumou J, van der Poll T, Speelman P, Hovius JW. Tired of Lyme borreliosis. Lyme borreliosis in the Netherlands. Neth J Med. 2011 Mar;69(3):101-11 HSE-Health Protection Surveillance Centre (HPSC) 25-27 Middle Gardiner Street, Dublin 1, Ireland. Tel: +353 1 8765 300 Fax: +353 1 856 1299 www.hpsc.ie