House Health and Aging Committee Proponent Testimony on
advertisement

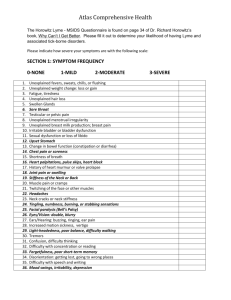
House Health and Aging Committee Proponent Testimony on House Concurrent Resolution 5 Chairwoman Gonzales and members of the House Health and Aging Committee, I am here today to testify in support of House Concurrent Resolution 5, cosponsored by Representatives Patterson and Ruhl, which urges the Centers for Disease Control and Prevention to take action to improve prevention, diagnosis, and treatment of Lyme disease. As a matter of introduction and background, my name is Kerry Metzger. I was a practicing dentist for some 26 years. I also had the privilege to serve in the Ohio House of Representatives as a member of this body from 1995 through 2002. I currently serve as a Tuscarawas County Commissioner and had the honor of serving as President of the County Commissioners Association of Ohio in 2009. I’m here today to strongly urge your support of HCR 5. Lyme disease is a deeply personal issue for my family. Both my wife, Karen, and my son, Ryan have contracted the disease and have had to deal with the chronic affects of it on a daily basis. I’ve seen firsthand the physical and the emotional toll this disease can have on your loved ones and witnessed the frustration that occurs when you can’t get any answers as to why you constantly feel so bad. I’ve seen firsthand the chronic fatigue, the joint and muscle pain, the numbness in the limbs, the inability to focus, the memory loss, and the anxiety and depression that affect not only your loved one’s body and mind but also affects their ability to carry on with the tasks of everyday life. Yes, this issue is personal to me but there are hundreds of thousands of people annually affected by this terrible disease and their voice needs to be heard! HCR 5 gives them that voice to be heard by the policy makers and the health care professionals who are in positions to improve the lives of those in the Lyme disease community. As you may be aware, Lyme disease is the most common tick-borne illness in the world today. And until recently, the Centers for Disease Control and Prevention reported an average of only 30,000 cases of Lyme disease annually in the U.S. However, two recent CDC studies (Hinckley and Hook et al.) have indicated that the true incidence may be greater than 300,000 cases and could be as high as 1 million cases per year! In comparison, HIV/AIDS is diagnosed at a rate of 55,000 new cases annually. Using the 300,000 case figure, Lyme disease appears to be around six times more common in the United States than HIV/AIDS! This appears to be of epidemic proportions! The actions, found in HCR 5, that the General Assembly is asking the CDC to take are essential, reasonable and practical. Action # 1 is to update definitions of Lyme disease symptoms by clinical diagnosis. The diagnosis of Lyme disease must be approached by considering all the symptoms along with the patient’s past history and not based just on one or two symptoms which could lead to misdiagnosis. We need to view these symptoms when diagnosing Lyme disease from the “30,000 foot view” and not by looking at just the individual trees. Action #2 asks the CDC to reconsider standards and best practices for diagnosis and treating Lyme disease. Many in the Lyme disease community feel that the diagnostic standards are too restrictive. They exclude many patients suffering with Lyme disease from being diagnosed properly and getting the treatment they so sorely need. Patients feel that the treatment standards in use are too restrictive, such as the use of short-term antibiotic therapy and the rejection of the long-term use of antibiotics to treat the disease. This approach to treatment contrasts with other serious infectious diseases such as tuberculosis and HIV/AIDS, where long-term antimicrobial therapy is the norm. Education is also a huge component of the prevention, diagnosis, and treatment of the disease. The general public needs to be made more aware of the disease, how you contract it and how it can be prevented through enhanced media campaigns. Even more important is the need to educate our physicians and medical community on current diagnostic and treatment options. Action item #3 addresses this need. The fourth action item concerns the need for improving the reporting techniques that the state and local public health agencies use to report diagnosed cases of Lyme Disease. The current CDC diagnostic criteria are too stringent with only objective signs of the disease, such as a “bulls-eye” rash, arthritis, or carditis to name a few, considered relevant. As a result many cases are never reported or treated. Better reporting techniques will allow the CDC to obtain better data on the incidence of Lyme disease nation-wide. An accurate surveillance picture will help hundreds of thousands of people affected by the disease to obtain more effective diagnoses and treatment for the disease. Finally, the Resolution asks the CDC to provide for improved funding and better laboratory testing to enhance early detection. This is essential if we are to be able to detect the presence of Lyme disease when it is in its early stages and is more easily treated than when it is detected too late and has already moved into the chronic form of the disease. Commercial laboratory testing continues to yield poor results and has been shown to be unreliable. One study was done that showed that testing has a sensitivity of only 46% in patients who have been infected for more than 4-6 weeks. This means that these tests will miss almost 50% of Lyme disease cases. In conclusion, HCR 5 is an important piece of legislation that informs the CDC about the concerns of many Ohio citizens regarding the prevention, diagnosis, and treatment of Lyme disease. Ultimately, attention to the issues it outlines will help all Ohio families affected with this terrible disease to receive accurate diagnoses and treatment and lead them towards living a normal life. Thank you and I will be happy to answer any questions that I can.