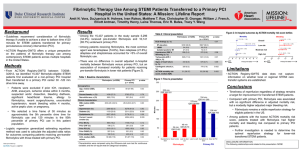
Table 1 - European Heart Journal
advertisement

Incidence and Multivariable Correlates of Long-Term (up to 4-Year) Mortality in Patients Treated with Surgical or Percutaneous Revascularisation in the Synergy Between PCI with TAXUS Express and Cardiac Surgery Trial Supplementary Appendix Contents 1. Supplementary Methods 2. Supplementary Tables a. Table 1: Comparison of anatomical and clinical variables between patients with and without discharge antiplatelet therapy in the CABG arm (n=897). b. Table 2: Comparison of anatomical and clinical variables between patients with and without post-procedural antiplatelet therapy in the PCI arm (n=903). 3. Patient Narratives a. Table 3: Known patient related events (as detailed in the patient narratives) preceding death in the 10 of the 11 patients not taking any postprocedural anti-platelet therapy at the time of death. 1 1. Supplementary Methods Continuous data are presented as medians and interquartile range (IQR) and were compared with the Mann-Whitney rank sum test. Categorical variables were compared with the chi-square test. 2. Supplementary Tables Table 1 Comparison of anatomical and clinical variables between patients with and without discharge antiplatelet therapy in the CABG arm (n=897). CABG No Antiplatelet Therapy on Discharge (n=100) Categorical Variables Peripheral vascular disease 13/100 (13%) Pre-procedural poor LVEF 6/100 (6.0%) COPD 15/100 (15.0%) History of GI bleeding peptic ulcer disease 7/99 (7.1%) Amiodarone therapy on discharge 9/99 (9.1%) Hypertension 83/99 (83.8%) Lack of pre-procedural aspirin 83/99 (83.8%) Metabolic syndrome 43/73 (58.9%) Left main coronary artery disease 30/100 (30.0%) Diabetes 33/100 (33.0%) On pump CABG 89/99 (89.0%) Anterograde administration of cardioplegia 84/99 (84.8%) Crystalloid cardioplegia 33/99 (33.0%) Incomplete revascularisation 39/99 (39.4%) Male 73/100 (73.0%) Current Smoker 22/97 (22.7%) High SYNTAX Score tertile 33/99 (33.3%) Blood cardioplegia 45/99 (45.0%) Retrograde administration of cardioplegia 14/99 (14.1%) Continuous Variables*** Age per increase in 10 years 69 (IQR 60-75) Creatinine (mg/dL) 1.00 (IQR 0.90-1.20) SYNTAX Score per increase in 10 points 27 (IQR 20-36) Cross-clamp time (minutes) 52 (IQR 37-64) BMI 28 (IQR 26-31) Post CABG peak CK-MB ratio 7.6 (IQR 4.4-11.9) Antiplatelet Therapy on Discharge (n=770) p-value 78/770 (10.1%) 14/770 (1.8%) 66/770 (8.6%) 31/764 (4.1%) 102/770 (13.2%) 581/765 (75.9%) 482/770 (62.6%) 270/616 (43.8%) 313/769 (40.7%) 208/770 (27.0%) 635/753 (82.5%) 618/754 (82.0%) 244/753 (31.7%) 280/770 (36.4%) 618/770 (80.3%) 168/768 (21.9%) 275/766 (35.9%) 382/753 (49.6%) 109/754 (14.5%) 0.38 0.009 0.037 0.17 0.24 0.080 <0.001 0.014 0.039 0.21 0.25 0.48 0.72 0.56 0.091 0.86 0.62 0.45 0.93 66 (IQR 58-72) 1.00 (IQR 0.85-1.10) 28 (IQR 21-37) 51 (IQR 38-67) 27 (IQR 25-30) 6.0 (IQR 3.5-10.3) 0.26 0.93 0.95 0.077 0.91 0.001 2 ***Continuous variables are presented as mean±SD in patients who died within 4-years (age and SYNTAX Score are presented as actual values). Abbreviations: GI gastrointestinal; COPD chronic obstructive pulmonary disease; IQR interquartile range; LVEF left ventricular ejection fraction; CABG coronary artery bypass graft surgery; CK-MB creatine kinase myoglobin, BMI body mass index. Table 2 Comparison of anatomical and clinical variables between patients with and without post-procedural antiplatelet therapy in the PCI arm (n=903). PCI No Post-Procedural Antiplatelet Therapy* (n=11) Categorical Variables Pre-procedural poor LVEF 0/11 (0%) Amiodarone therapy on discharge 0/11 (0%) Peripheral vascular disease 2/11 (18.2%) History of GI bleeding or peptic ulcer disease 0/10 (0%) Female gender 6/11 (54.5%) Lack of pre-procedural thienopyridine** 2/11 (18.2%) Diabetes 6/11 (54.5%) Hypertension 9/11 (81.8%) Metabolic syndrome 6/9 (66.7%) Incomplete revascularisation 7/11 (63.6%) Current smoking 3/11 (27.3%) Stent length greater than 100 mm 5/8 (62.5%) Any total occlusion 2/11 (18.2%) Left main coronary disease 4/11 (36.4%) Age per increase in 10 years SYNTAX Score per increase in 10 points Serum creatinine (mg/dL) Post PCI peak CK ratio Total number of stents Total stent length (mm) BMI Post PCI peak CK-MB ratio Continuous Variables*** 73 (IQR 70-75) 32 (IQR 17-39) 1.00 (IQR 0.90-1.60) 2.8 (IQR 0.5-4.9) 7 (IQR 4-8) 136 (IQR 64-148) 25 (IQR 24-26) 24.8 (IQR 14.3-32.8) Antiplatelet Therapy p-value on Discharge†* (n=885) 12/885 (1.4%) 13/885 (1.5%) 80/885 (9.0%) 37/881 (4.2%) 204/885 (23.1%) 26/885 (2.9%) 248/885 (28.0%) 649/878 (73.9%) 331/722 (45.8%) 381/885 (43.1%) 163/885 (18.4%) 286/869 (32.9%) 212/879 (24.1%) 348/885 (39.3%) 0.70 0.69 0.30 0.51 0.014 0.004 0.052 0.55 0.21 0.17 0.45 0.077 0.65 0.84 66 (IQR 59-73) 27 (IQR 20-35) 1.00 (IQR 0.80-1.10) 0.54 (IQR 0.35-0.91) 4 (IQR 3-6) 80 (IQR 52-112) 27 (IQR 25-31) 12.5 (IQR 6.2-20.3) 0.012 0.38 0.46 0.014 0.12 0.13 0.10 0.21 *Aspirin or thienopyridine **Clopidogrel or ticlopidine ***Continuous variables are presented as medians±IQR in patients who died within 4-years (age and SYNTAX Score are presented as actual values). Abbreviations: PCI percutaneous coronary intervention; GI gastrointestinal; IQR interquartile range; LVEF left ventricular ejection fraction; CK creatine kinase; CK-MB creatine kinase myoglobin, BMI body mass index. 3 3. Patient Narratives Table 3 Known patient related events, as detailed in the patient narratives, preceding death in the 10 of the 11 patients not taking any anti-platelet therapy at the time of death. Age/ Gender 79/F SYNTAX Score 13 (LM + 2VD) Known Events Preceding Death (Autopsy Details Provided Where Available) 73/F 15 (3VD) 74/M 64 (LM + 3VD) 67/F 17 (3VD) Attempted RCA PCI - coronary dissection with inferior ST elevation (no stents implanted). Emergency CABG: SVG TO RCA and LCx OM branches. Cardiogenic shock post-procedure: patient expired within 6 hours. Autopsy: “acute myocardial infarction of the wall of the left ventricle…haemopericardium developed, this was the direct cause of death.” 81/F 31 (3VD) Peri-procedural small distal perforation conservatively treated: “small area of intramyocardial dye ‘staining’ probably due to a small distal perforation induced by the hydrophilic guidewire.” 6 hours post PCI developed sudden hypotension secondary to cardiac tamponade leading to death. Autopsy: cause of death haemopericardium, “...the examination of the 3 coronary vessels documented the presence of normally positioned and patent stents…” 72/F 39 (3VD) Left main, mid LAD stent implantation. Coronary perforation in LAD. Cardiac tamponade necessitating pericardiocentesis and cardiac surgery – bleeding site identified in right anterior wall next to proximal LAD. SVG to LAD, LCx and PDA. Developed systemic inflammatory response syndrome, “multi-organ failure with disseminated intravascular coagulation…massive liver failure, increasing lactic acidosis…” 13 days post index procedure patient expired. 71/M 38 (LM + 3VD) PCI to trifurcation lesion of left main (crush technique) and mid LAD. PCI to RCA 4 days later as staged procedure. Acute stent thrombosis 1 day post staged procedure – catheterisation revealed thrombotic occlusion of common trunk. “Using PTCA, partial rehabilitation of the anterior descending artery was obtained. Recanalization of the intermediate ramus and circumflex was not obtained.” Underwent emergency CABG: LIMA LAD, SVG D1 and OM (no RCA graft documented). Seven days post CABG, “suddenly…the blood pressure decreased…subsequently experienced refractory hypotension…patient expired.” No autopsy performed. 56/F 32 (3VD) Acute stent thrombosis/LAD abrupt closure 1 hour post 3VD PCI necessitating emergency PCI. Over the following 5 days developed respiratory sepsis, congestive heart failure and cardiogenic shock. New severe mitral regurgitation and worsening left ventricular function necessitating surgical mitral valve repair (no documented grafts) and biventricular assist device. Persistent ventricular failure and profound acidosis. Treatment withdrawn due to poor prognosis. Patient expired 17 days post index procedure. 75/M 65 (LM + 3VD) 76/M 33 (3VD) Anaemia and thrombocytopenia (unknown cause), on warfarin long term (recurrent DVT/PE). Transfused 2 units packed red cells and platelets pre-procedure. 5 days post procedure melaena and anaemia. 9 days post index PCI, sudden cardiac arrest/death. No autopsy performed. 24 hours post index PCI, a significant fall in haemoglobin necessitating 3 unit blood transfusion. Upper GI endoscopy demonstrated ‘duodenitis.’ 9 days post index procedure, developed sudden anterior infarct/cardiac arrest. Autopsy: “Taxus Express stents were deployed in the LM-LAD and LM-LCx bifurcations, so both stents extended to the proximal segment of these vessels (LAD and LCx). The stent thrombosis occurred in each of these stents.” Rapidly progressive hypotension and cardiac arrest during index PCI procedure with bleeding from right femoral puncture site. Patient was anticoagulated with coumadin preadmission and received abciximab. Computed tomography imaging of abdomen confirmed retroperitoneal bleeding as cause of haemorrhagic shock. Developed disseminated intravascular coagulopathy, multiorgan failure and expired 3 days post index procedure. Patient became haemodynamically and electrically unstable during the procedure. Peri-procedural death despite placement of stent in the left main stem. No autopsy performed. Balloon catheter rupture during PCI to LCx (only 1 stent deployed) with retainment of material. Underwent emergency CABG for extraction of ruptured balloon catheter and SVG to PDA, LAD and OM. Patient developed cardiogenic shock a few hours post CABG requiring inotropic support. Patient expired 9 days post index procedure. 4 Abbreviations: 2VD 2 vessel disease; 3VD 3 vessel disease; CABG coronary artery bypass graft; DVT deep vein thrombosis; GI gastrointestinal; LCx left circumflex; LAD left anterior descending; LIMA left internal mammary artery graft; LM left main; OM obtuse marginal; PCI percutaneous coronary intervention; PE pulmonary embolism; PTCA percutaneous transluminal coronary angioplasty; RCA right coronary artery; SVG saphenous vein graft 5