Lower GI bleed - WordPress.com
advertisement

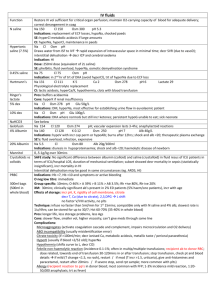
Lower GI bleed Epidemiology Incr morbidity rate if: haemodynamic instability, rpted haematochezia, gross blood on PR, initial Hct <35%, syncope, non-tender abdo, aspirin use, >2 co-morbid conditions Distal to ligament of Trietz Pathophysiology Causes 60% diverticular disease (R=L; acute, painless; can be heavy; 90% resolve spontaneously) Assessment Investigations Mng In paeds Mortality 5-10%; 20% of all GI bleeds; significant haemorrhage with haemodynamic compromise uncommon; stops spontaenously in 80% 10-20% no cause found 12% angiodysplasia (more in elderly; often recurrent; usually R; rarely severe; assoc with AS) 2% Ca / polyp Others: ischaemic colitis, infection, IBD, aorto-enteric fistula If <20yrs: Peutz Jegher syndrome, HSP, Meckel’s diverticulus Sx: blood mixed with stool = likely higher; pink frothy blood in pan or on paper = haemorrhoids; tarry black stool = upper GI; bright red and not severely shocked = lower GI; haematemesis = upper GI; bright red on surface of stool or toilet paper = fissure OE: look for signs of chronic liver disease Bloods: incr Ur:Cr and incr K suggests upper GI; decr Hb and normal MCV = acute; decr Hb and MCV = chronic; incr plt = acute; macrocytosis = hepatic disease; G+S if mod, XM if severe Erect CXR: if AP or findings in chest CT: 79-100% sens IVF As OP if: bleeding not haemodynamically signficant and ceased Colonoscopy if: bleeding haemodynamically significant but ceased if rectal bleeding >50yrs, need colonscopy as OP Angiography if: bleeding haemodynamically signficiant and ongoing requires >0.5ml/min; 10% serious complication rate OT if: torrential bleeding or failed scope ?ischaemic colitis; laparotomy has incr mortality and morbidity Technetium-labelled RBC: good at detecting intermittent bleeding; requires >0.1ml/min <2/12: swallowed maternal blood, infectious colitis, intussusception, volvuls, AVM, haemorrhagic disease of newborn, Hirschsprung disease milk allergy (onset 12-24hrs after introduction of new formula or chronic diarrhoea, poor weight gain and AP; IgE mediated) meckel diverticulum (remnant of omphalomesenteric duct in distal ileum, 2% incidence, lined with ectopic gastric mucosa, painless PR bleeding; may result in signficant bleeding) 2/12 – 2yr: milk allergy, intussusception, volvulus, meckel diverticulum anal fissure, gastro, HUS, HSP (may be severe), polyps, IBD >2yr: intussusception, volvulus, meckel diverticulum, anal fissure, gastro, HUS, HSP, polyps, IBD haemorrhoids, colitis, angiodysplasia, celiac disease, PUD Notes from: Dunn, Cameron, TinTin