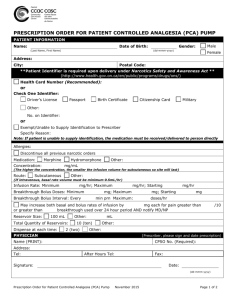
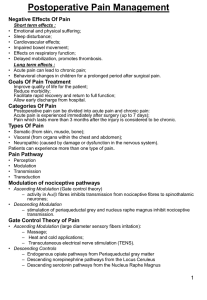
Pain Medications
advertisement

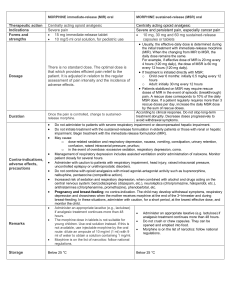
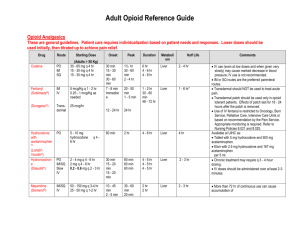
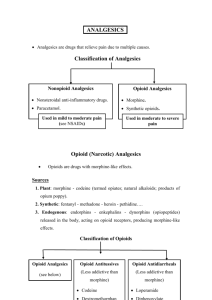
Pain Medications Over the counter pain meds-non opioid Both acetaminophen and nonsteroidal antiinflammatory drugs (NSAIDs) (ibuprofen and others) reduce fever and relieve pain caused by muscle aches and stiffness, Acetaminophen works on the parts of the brain that receive the "pain messages." Reduce fever and relieve pain caused by muscle aches and stiffness Dose excess is easy because in many products Causes hepatic damage—DO NOT exceed 3-4 g/day NSAIDS reduce inflammation (swelling and irritation); reduce fever and relieve pain caused by muscle aches and stiffness work by reduction of prostaglandisn (hormone-like substances that cause pain) available in a prescription strength Analgesic ceiling—more medication will not give more pain relief Gastric upset Platelet dysfunction and bleeeding All NSAIDS inhibit the enzyme cyloxygenase (COX) COX-2 is produced mainly at the site of tissue injury; therefore COX-2 inhibitors like Celebrex (celecoxib) may produce better pain relief for inflammatory pain like arthritis. Some COX-2 inhibitors have been removed from the market because of a high association with cardiovascular events. Opioids—can be agonist, antagonist, or mixed; most of the commonly used one are agonists. Opioids are narcotic pain medications that contain natural, synthetic or semi-synthetic opiates. Opioids are often used for acute pain, such as short-term pain after surgery. Better for nociceptive pain than neuropathic pain; No analgesic ceiling Adding acetominophen or NSAID limits the daily dose that can be given Some examples of opioids include: Morphine; Dilaudid (hydromorphone) usually given IV; IV narcotics have an onset of action of about 2-5 minutes, peak in 20 minutes. Rapid pain relief but don’t last as long as IM or PO. Need to know the onset and peak so you know when it is safe to give the next dose. Respiratory depression is an important observation. Respiratory rate below 10 may require Narcan (naloxone—an opioid antagonist). Dilaudid is much more potent than morphine, therefore the dose is much lower. While both of these are used for severe pain; hydromorphone is generally reserved for the most severe pain. Naloxone given IV will provide instant relief of respiratory depression, but you will have a patient in pain; therefor use lowest possible dose; will wear off before the narcotic; anticipate return of respiratory depression Morphine: Oral forms exist but require higher doses because or the first pass effect . Fentanyl—potent, rapid acting; patch for round the clock pain relief; generally used for cancer pain; if have breakthrough pain may treat with additional pain medication. Also use as anesthetic. Oxycontin—long acting form of oxycodone; po; do not crush— MS contin—long acting form of morphine; do not crush, patient will get all medication at once (possibly lethal) Oxycodone/acetominophen (Vicodin 5 mg/500 mg, Norco 10/500); other forms of acetominophen should not be taken because of the danger of liver toxicity Codeine—not commonly used; may be in prescription cough medicine Opioids are effective for severe pain and do not cause bleeding in the stomach or other parts of the body as can other types of pain relievers Side effects of opioids may include: Drowsiness, dizziness, especially in opioid naïve, goes away with long term use Nausea, vomiting, stomach pain, especially in opioid naïve, goes away with long term use Constipation—doesn’t go away with long term use Itching—may or may not be a sign of allergic reaction; observe carefully; Benadryl may help Difficulty urinating-less common Respiratory depression—especially in narcotic naïve patients and people with preexisting respiratory problems, but could happen in any patient Addiction . It is rare for people to become addicted to opioids if the drugs are used to treat pain for a short period of time. Mixed agonist-antagonist—Talwin (pentazocine and Stadol (butorphanol)—produce less respiratory depression; also cause more dysphoria and agitation; have an analgesic ceiling Demerol (meperidine) only for acute pain lasting 2 days of less; long term use or high doses can cause neurotoxicity, e.g. seizures, hyperpyrexia with delirium and death when taken with MAO inhibitors. It is a good drug if used correctly. Darvon—no more effective that 600 mg of aspirin. Adjuvant Analgesic Therapy Anticonvulsants Anticonvulsants are drugs typically used to treat seizure disorders. Some of these medications are shown to be effective in treating neuropathic pain and migrain headaches, as well. The exact way in which these medicines control pain is unclear but it is thought that they minimize the effects of nerves that cause pain. Some examples include carbamazepine (Tegretol), gabapentin (Neuronton) and pregabalin (Lyrica). In general they are well tolerated. The most common side effects include: Drowsiness Dizziness Fatigue Nausea Alpha 2 adrenergic agonists; Corticosteroids; Local anesthetics Scheduling Schedule for prevention or control (before pain becomes severe) Constant chronic pain (like cancer pain) should have 24 hour dosing with addition dose for breakthrough pain Fast acting drugs for breakthrough pain; long acting for constant pain Titration—start with low dose and give frequently until pain is relieved, with minimal side effects. Must know the onset and peak of action to safely titrate a dose. For example, morphine IV has an onset of action in 2-5 and peaks in ~ 20 minutes. Therefore in 20 minutes you are seening the full effect; if no respiratory depression it is safe to give more. This allows us to administer morphine even to respiratory patients For acute pain titration over time is usually downward as the acute process is resolving and pain becomes less severe; for cancer pain titration is often upward as tolerance develops or pain becomes more severe Routes Intravenous—most commonly used for severe, acute pain—morphine or oxymorphone Intramuscular—not commonly used in hospital; gives longer duration of action than IV; very short term use only because of pain at site, unreliable absorption, possible abscess and with long term use-fribrosis. Onset ~15 minutes; peak 60-90 minutes; duration 4-6 hours Oral—mild to moderate pain; must have functioning GI tract; hydromorphone and hydrocodone; Long acting for constant chronic pain such as as cancer pain—oxycontin, MS-contin. Morphine is given to cancer patients po. Need 30 mg to be equivalent to 10 mg of morphine because of the first pass effect MS contin takes 2 hours to be effective with first dose. May need to take breakthrough med at the same time. On the other hand Oxycontin immediately releases 1/3 of its dose; should not take breakthrough med wit oxycontin. Sublingual or buccal—for amount absorbed buccal or sublingual, first pass effect not present Rectal—good route if can’t take oral and IV access not available Transdermal—fentynal patch is absorbed slowly and take 12-17 hours for full effect; change 4872 hours depending on patient response Spinal—needs smaller doses; monitor carefully for overdose and infection; Inplantable pump is sometimes used Patient-controlled analgesia (PCA)—titrates IV MED according to patient need; giveS patient control. Programmed for a maximum dose. May be programmed for constant delivery of set dose with patient controlled intermittent dose. May give push for breakthrough pain.