What are the complications of infection in association with
advertisement

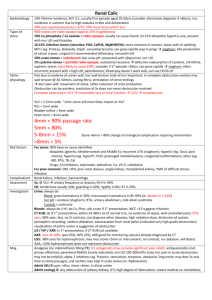
What are the complications of infection in association with obstruction of the upper urinary tract? How is it managed? Obstruction – block of urine flow through the ureter → distension of renal pelvis and calyces. Intrinsic / extrinsic Most common cause of obstruction and infection is stone disease. Unwell, fever, flank pain and tenderness This is a urological emergency Consequences of Infection + Obstruction Pyonephrosis Infected hydronephrosis. Pus accumulates in renal pelvis + calyces. Can present with sepsis or septic shock. Perinephric abscess Consequence of extravasation o infected urine outside the parenchyma of the kidney. Abscess develops in Gerota’s fascia Emphysematous pyelonephritis Caused by gas forming organisms (usually E.coli, also klebsiella, proteus). Presents as severe acute pyelonephritis which fails to respond to antibiotics. Radiographic evidence of gas within and around kidney. 70 – 90% are diabetic. Presents with a flank mass, rarely surgical emphysema, hyperglycaemia. Carries a high mortality Management - IV antibiotics, fluid resuscitation, percutaneous drainage, diabetic control. If sepsis not controlled – nephrectomy Xanthalomatous pyelonephritis Severe infection resulting in destruction of renal tissue and a non-functioning kidney. Can present acutely with acute flank pain, fever, tender flank mass. Commonly e.coli and proteus Fat laden macrophages deposited around abscesses in parenchyma of kidney. Kidney becomes grossly enlarged, containing yellowish nodules, pus and areas of haemorrhagic necrosis. On CT difficult to distinguish from RCC (great imitator, calcification often seen within renal mass). How is it managed? Early recognition Treat sepsis – hydration, appropriate broad spectrum antibiotics, HDU/ITU if septic shock. Relieve obstruction – Retrograde stent Percutaneous nephrostomy Two randomised trials have compared retrograde stent insertion with percutaneous nephrostomy with one trial reporting specifically on patients with acute sepsis and obstruction. Neither trial showed one superior modality of decompression in effecting decompression and resolution of sepsis. An overall major complication rate from percutaneous nephrostomy insertion was found to be 4%, although the complication rates from stent insertion are less consistently reported. (Ramsey) Radiologists would prefer more retrograde stent insertions Potentially higher failure rate, higher cost and anaesthetic risk with retrograde stent S Ramsey, A Robertson, MJ Ablett, RN Meddings, GW Hollins, B Little. Evidence-Based Drainage of Infected Hydronephrosis Secondary to Ureteric Calculi: Journal of Endourology: 2010