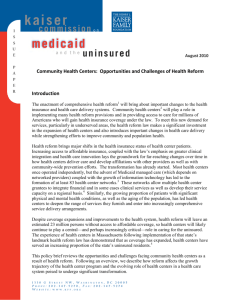
Ethics and Health
System Reform:
Caring for Vulnerable Patients
and Populations
University of California at Davis
February 2012
Matthew Wynia, MD, MPH
Institute for Ethics at the American Medical Association
Disclosure and Disclaimer
Matthew Wynia, MD, MPH, FACP
Has no financial relationships with any for-profit
entities producing health care goods or services
consumed by or used on patients.
Views and opinions expressed are mine alone and
should not be construed as policy statement of the
American Medical Association
“Of all the forms of inequality,
injustice in health care is the
most shocking and inhumane.”
March 25, 1966
Goals for Today
Reasons for reform: coverage and cost
The health reform puzzle
How reforms might affect especially
vulnerable patient populations
Expanding access
Public health and wellness
Health disparities
Home and community based care programs
Vulnerable populations and payment reform
“I want my coverage to stay the same.”
Pre-ACA it was clear that significant change
was inevitable
2010 Towers-Watson Employer Survey
“In 2010, 83% of companies have already
revamped or expect to revamp their health care
strategy.”
“57% - are very confident that employers will
continue to offer health care benefits 10 years
from now.”
• Released March 9, 2010
“It's critical that we keep the
momentum going to achieve
meaningful health care reform
this year … The status quo is
unacceptable.”
J. James Rohack, MD,
AMA President
St Louis Post-Dispatch, Oct. 8, 2009
“This is a second opinion. At first, I thought you
had something else.”
“It's critical that we keep the
momentum going to achieve
meaningful health care reform
this year … The status quo is
unacceptable.”
J. James Rohack, MD,
AMA President
St Louis Post-Dispatch, Oct. 8, 2009
% GDP
The Future without Reform
According to the CBO
Without reform, premiums hit 25K
within 10 years
August, 2009
Cumulative Changes in Health Insurance Premiums,
Overall Inflation, and Workers’ Earnings 2000 - 2008
Health Insurance Premiums
Overall Inflation
Workers' Earnings
98%
100%
87%
80%
73%
60%
60%
43%
40%
25%
24%
25%
20%
21%
2007
2008
20%
20%
11%
7%
0%
0%
0%
2000
10%
12%
15%
18%
14%
4%
3%
5%
7%
2001
2002
2003
10%
2004
2005
2006
From Jon Gabel
Source: KFF/HRET Survey of Employer-Sponsored Health Benefits, 2001-2008; Bureau of Labor Statistics,
Consumer Price Index, U.S. City Average of Annual Inflation (April to April), 2001-2008; Bureau of Labor
Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey (April to April), 2001-2008.
Value = The Nexus
of Quality and Cost
Health Affairs, 10.1377/hlthaff.w4.184, 2004
“…the value to U.S. employers and workers of the U.S. health system
was 23 percent below that of the G-5 countries’ health systems. The bulk
of the U.S. value shortfall was attributable to much higher spending in the
United States to attain a level of workforce health and care quality that
trails the G-5 by roughly 10 percent across 17 measures.”
The Business Roundtable
Health Care Value Comparability Study
February 28, 2009
The Newspaper Summary…
“If the global economy were a 100-yard dash,
the U.S. would start 23 yards behind its
closest competitors because of health care
that costs too much and delivers too little.”
AP Report, March 12, 2009
"Employers are angry, fed up and desperately
seeking relief from a system that ranks
37th worldwide in quality of care but
costs more per capita than other
industrialized nations.”
Bonnie Blackley
Benefits Director, Blue Ridge Paper Products
In testimony to the US Senate, 2008
Employees Pay for Rising Health Care Costs
Chart borrowed from
Emanuel and Fuchs,
2008, JAMA
Wages, not corporate profits, are
sacrificed to pay for health care.
Productivity and indexed wages
1972-2004
Adjusted corporate profits
1985-2006
Injustices in US Health Care
Sacrifice other social investments to pay
for an insatiable health care system
Poor and uninsured often pay more for the
same service than insured and wealthy
Uninsured often receive late (and
expensive) care in emergency departments
American business bears unequal burden
in international competition
American entrepreneurialism restricted by
fears of uninsurance
Who are the uninsured?
• 46 million
`
63% are full time workers
85% are in families headed by a worker
Minorities and health insurance
~1/3 of the US population but …
~50% of the uninsured
~50% of patients at FQHC
~50% of Medicaid beneficiaries
More likely to work low-paying jobs without
employer sponsored coverage
Higher rates of many chronic diseases
$$ Cost of health disparities
>30% of all care costs for minorities are due to
inequities
Direct and indirect costs of disparities over a 3
year period estimated to be $1.24 trillion
direct costs = additional illness care provided to
disadvantaged populations ($230 billion)
indirect costs = lost productivity, lost wages,
absenteeism, family leave, and premature death
LaVeist TA, Gaskin DJ, and Richard P. (2009). The Economic Burden of Health
Inequalities in the United States. Washington, DC: Joint Center for Political and
Economic Studies.
Unique features in CA
57% of population and >2/3 of uninsured are
‘minorities’
Nearly 500,000 minority-owned small
businesses
>1,000 FQHC delivery sites, serving about 2.5
million patients (75% are racial/ethnic
‘minorities’)
The evolving face of the uninsured
Between 2004 and 2008 the proportion
of those 18-64 without insurance rose …
Almost 20% ↑ among non-poor (> 3x FPL)
↑ 6.6% among whites
↑ 13.5% among those with at least a HS
education
MMWR, Jan 14, 2011
In sum … systemic transformation
was recognized as inevitable
Declining coverage
Employer-sponsored coverage decline >10% since 2000
Rising cost
5% rise in premiums seems low, but not compared to -1%
inflation
Demographic changes
Elderly population will double in next 20 years
Uneven quality
Deliver ~50% of appropriate care
Recent ‘solutions’ weren’t working, or favored
Problems with solutions that mainly allow stripped down
coverage and increased cost-sharing…
Health Reform: What Counts?
S-CHIP re-authorization
~20 billion to promote HIT
$$ for Clinical Effectiveness Research
All this was accomplished with
ARRA/HITECH, but it wasn’t enough
Because our health care system is a big
puzzle, with lots of pieces…
(And it’s not done yet)
So, let’s focus on one set of issues …
improving care for uninsured, vulnerable
patient populations
What’s NOT in the law?
56% think it includes a government-run
insurance option
35% think it includes a government panel to
make end of life care decisions
48% of Republicans
50% think it allows cost sharing for
preventive services
56% of Americans want to keep or expand
the health reform law
KFF tracking poll, November 2011
Access to private insurance
By 2014, 32 million people will have insurance
who would have been uninsured otherwise
The ACA:
Bans pre-existing condition exclusions
Bans lifetime limits on coverage
Bans rescissions of coverage upon becoming ill
Bans higher premiums for sick people
Everyone might benefit from these provisions
(esp. including minorities and the disabled)
Medicaid expansions
In 2014, Medicaid programs nationwide will
cover individuals and families with incomes up to
133% FPL
In California, ~66% of those newly covered by
Medicaid will be minorities
Cook Co Hosp expects new enrollees to cost
~$2,000/each, suggesting mostly well single people
New enrollee costs covered entirely by federal funds
Improved payments to Medicaid PCPs
Public health and wellness
(selected provisions)
$11b new funding for CHCs
CA has 113 FQHCs, serving ~2.5 million
75% of CA FQHC patients are minorities
Community health workers
Grants for organizations that hire community health
workers
Funding to train, supervise and support community
health workers for 2010-2014
Requires coverage of preventive care and
wellness (without co-pays or deductibles)
Disabilities provisions (selected)
Community First Choice Option for Medicaid
6% increase in federal payments for home services
“Money Follows the Person” demonstration project
Extended through 2016 (promotes transitions to home and
community based care)
State Balancing Incentive Program
2% increase in federal payments through 2015 for “conflictfree case management” and transitions to HCBS
1915 (i) amendment
Allows statewide HCBS option in Medicaid without enrollment
ceiling for patients not requiring NH level care (not likely in IL)
CLASS Act (suspended)
Disparities provisions (selected)
Workforce diversity
Scholarships/grants/loan repayment programs (e.g., §5402)
CE support for health professionals (e.g., §5307)
Grants to improve health care services, increase retention, and
increase the representation of minority faculty members
Data collection
All data to be collected and reported by race, ethnicity, sex,
primary language, and disability status for participants at the
smallest geographic level possible for all federally conducted or
supported health care or public health programs. (§4302)
Many other possibly relevant
provisions
Extended Federal Tort Claims Act coverage to officers, governing
board members, employees, and contractors of free clinics
Medicare bonus payments for primary care physicians and general
surgeons.
Increasing geographic adjustments for Medicare physician
payments.
Benefits must be described in “plain language”
NHSC increase to $2.7 billion through 2015 (§5207)
Primary care training, including CC training (§5301)
Makes OMH an NIH Institute
$500 million for care transitions programs (§3026)
Payment reform provisions to promote more coordinated and
efficient care…
Many challenges
Will the individual mandate be overturned?
How will the “mandate” to purchase insurance
work for poor and uninsured people – how many
will elect to pay the penalty rather than purchase
insurance?
What happens to safety net facilities when
many of their patients obtain coverage?
How will the variety of pilot programs to
incentivize better care work?
Pilot programs
“Where we crave sweeping transformation, however,
all the current bill offers is those pilot programs,
a battery of small-scale experiments. The strategy
seems hopelessly inadequate to solve a problem
of this magnitude. And yet – here’s the interesting
thing – history suggests otherwise.”
Testing, Testing
Atul Gawande, MD
The New Yorker, Dec 14, 2009
Focus on one set of issues
Ethical Issues in Payment Reform
Bundled Payment
Gain-sharing (and risk-sharing)
Pay for performance
Focus on one set of issues
Ethical Issues in Payment Reform
Bundled Payment
Gain-sharing (and risk-sharing)
Pay for performance
Quality Measurement and Equity:
What do physicians say?
“Dr. Brook correctly states that the use of physician-specific outcome data
would radically change how we practice medicine. Based on his system, I
would assess each patient's risk. If it differed dramatically from the
"sickness" scale that he proposes, I would consider asking the patient to
seek care elsewhere.”
•
Stephen Clement, MD, Annals of Intern Med 1994
“If my pay depended on A1c values, I have 10-15 patients whom I would have
to fire. The poor, unmotivated, obese and noncompliant would all have to
find new physicians.”
•
Physician in a 2005 survey on P4P (Casalino et al 2007)
“39% of physicians in this study were willing to discharge hypothetical
patients who were nonadherent or questioned the physician’s decisionmaking.”
•
Farber et al. JGIM 2007
Inequities of bonuses for hitting
target performance level
Those in this area have
little hope of gaining
the bonus
Those in this area have
a strong incentive to improve
Those in this area will
get the bonus with no
additional work
Quality
Target
Could performance
measurement harm quality?
How: Neglect of the unmeasured
“Incentives based on a handful of measures of
quality may encourage physicians to focus their
efforts on improving quality in the areas targeted by
the programs, neglecting other important aspects of
care” (Epstein et al. 2004)
Few data to date …
NEJM 2009; 361:368-78
Could performance measurement harm
quality in other ways?
Boyd et al: 79 yo woman with DM, COPD, HTN,
osteoporosis and osteoarthritis
Follow relevant guidelines: 12 meds, $406/month,
complex lifestyle modifications, possible
interactions… ?? top quality
Fee and Weber: Of patients not receiving antibiotics
within 4 hours for pneumonia, 58.5% not diagnosed
before leaving the ED
Could prompt overuse of antibiotics
J Gen Intern Med, July 2009
How should we pay doctors so that they will be motivated
to provide high-quality care?
J Gen Intern Med, July 2009
How should we pay doctors so that they will be motivated
to provide high-quality care?
Assumptions
The reason we suffer from poorer than desired quality is that
physicians aren’t motivated enough
Financial incentives will increase physicians’ motivation
Research in education
“people expecting to receive a reward for completing a
task, or doing it successfully, simply do not perform as
well as those who expect nothing.”
Alfie Kohn, 1994
4 meta-analyses have confirmed “tangible rewards [have]
a significant negative effect on intrinsic motivation…”
Deci and Ryan, 1999
This is a “major anomaly” in economics
Monetary rewards and
motivation
Temporary: Results achieved with monetary
incentives don’t “create an enduring commitment
to any value or action.” (Kohn 1993)
Risky: May reduce intrinsic motivation through
“external shifting” or “crowding out.”
Monetary incentives can, and do, backfire if…
Interesting work
Small rewards for work required
Externally controlled reward system
Incentives and Motivation
“Increasing external incentives reduces internal
motivation… [so the worst problem with P4P
would be] “if you ended up with a system
where… doctors only did anything because
they were paid for it and had lost their
professional ethos.”
Martin Rowland, NHS (Health Affairs
interview, Sept 2006)
Still, paying for improved performance is
probably better than the opposite…
Measuring quality (and especially rewarding
for doing “well”) holds risks, BUT
Payers won’t keep paying for unclear quality
Have to pay practitioners and providers
somehow…nothing is perfect
Need to
Be aware of, mitigate and track known risks
Maintain professional control of measures
Thank You
For more information, please visit
www.hsreform.org
www.ama-assn.org/go/ethicsinstitute
Or e-mail me at:
matthew.wynia@ama-assn.org