Parkinson`s disease
advertisement

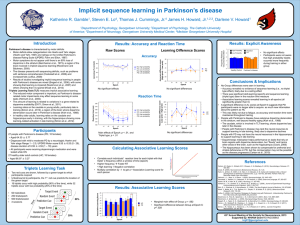
Parkinson's Disease Dr. Kleyn Department of Geriatric Medicine SVCMC History James Parkinson 1817, England Shaking palsy Paralysis agitans “Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with a propensity to bend the trunk forward, and to pass from a walking to a running pace, the senses and intellects being uninjured.” Introduction Parkinson’s disease is a chronic neurodegenerative movement disorder affecting voluntary and emotional movements and most commonly seen in the elderly, but is also found in the young and inexorably progresses leading to significant disability. Epidemiology Primarily a disease of the elderly Mean age 55, Range 20 - 80 years Juvenile parkinsonism- Less than 20 years M/F = 3:2 Prevalence increases with age Aging and Parkinson’s disease Exponential fall Linear fall Anatomy-Basal Ganglia Internal capsule Putamen Globus pallidus Caudate Nucleus PATHOPHYSIOLOGY PATHOPHYSIOLOGY DA SUBSTANTIA NIGRA GLOBUS, PARS RETICULATA A C H GABA STRIATUM CAUDATE, PUTAMEN Chemical Balance in Corpus Striatum Excitatory Cholinergic pathway BALANCE Inhibitory Dopaminergic pathway Chemical Balance in Corpus Striatum Excitatory Cholinergic pathway Imbalance Inhibitory Dopaminergic pathway Parkinson’s disease - Pathophysiology Pathology - Lewy Bodies Eosinophilic hyaline inclusion bodies Spherical dense hyaline core with a clear halo Mechanism of formation unknown Pathology Lewy body dementia Parkinson’s disease Pathology-Parkinson’s disease MIDBRAIN Classification and Etiology Idiopathic Parkinson’s disease Parkinson-like syndromes Drug induced parkinsonism Hypoxia Tumor Trauma Vascular:Multiinfarct Toxin:Mn, CO, MPTP and cyanide Post-encephalitic parkinsonism (von Economo’s encephalitis) Normal pressure hydrocephalus Wilson’s disease, Hutington’s disease Classification and Etiology Medications that can cause parkinsonian symptoms, but not PD itself, include the following: o o o o Metoclopramide Domperidone Reserpine-containing antihypertensives Neuroleptics Some evidence also indicates that certain environmental factors (including smoking and coffee drinking) may actually have protective associations. Clinical features of Idiopatic Parkinson’s disease. Major features Minor features Resting tremor in hands, arms, legs, jaw, and face Bradykinesia Rigidity- cogwheel or lead-pipe Bradyphrenia Speech abnormalities Depression Dysautonomia Dystonia Constipation Hallucinations Dysphagia Parkinson’s disease Symptomatology Parkinson’s disease -Symptomatology Tremor dominant Tremor: Rest Fixed frequency 3-6 Hz Not a feature of old age Pill-rolling Usually starts in one limb, and then to other limbs Rarely starts in lower limbs Intermittent for many years They usually disappear briefly during movement and do not occur during sleep. Tremors can also eventually occur in the head, lips, tongue, and feet. In younger patients tremor is usually predominant and often suggests a less aggressive form of the disease. Parkinson’s disease-Symptomatology Rigidity Striatal hand: Ulnar deviation, MCP flexion, IP extension Striatal Sitting toe: Big toe dorsiflexion en bloc: Collapses into a chair on attempting to sit down Parkinson’s disease-Symptomatology Posture Kyphosis Flexed elbows, knees and hips Hands held in front of body Trunk bent forward Head bowed Parkinson’s disease-Symptomatology Bradykinesia Slowness of motion (bradykinesia) is one of the classic symptoms of Parkinson's disease. Hypomimia- “masked facies”,expressionless face, blinking Speech abnormalities Hypophonia: soft voice Aprosody of speech: monotonous and lack of inflection Tachyphemia: do not separate syllables together, running words together Patients may eventually develop a stooped posture and a slow, shuffling walk. The gait can be erratic and unsteady. Parkinson’s disease-Symptomatology Motor fluctuations Freezing phenomenon- Sudden, transient inability to perform active movements, lasting no more than a few seconds Start hesitation Turn hesitation Target hesitation Palilalia (speaking) Apraxia of eyelid opening Writing Kinesia paradoxica-Despite severe rigidity and bradykinesia, they may rise suddenly and move normally Parkinson’s disease-Symptomatology “Today is a sunny day in Toronto" Loop drawing: Amplitude Interloop distance “Micrographia” Parkinson’s disease-Symptomatology Festinating gait Drooling of saliva Dysphagia Constipation Dementia Depression Orthostatic hypotension Low resting blood pressure HTN Normotensive Sweating abnormalitiesexcessive perspiration Blepharospasm/ keratitis Movement Disorders Parkinson’s disease Hutington’s disease Multiple system atrophy Motor neuron disease Cortical basal ganglionic degeneration Patients with PD may develop a stooped posture and a slow, shuffling walk. The gait can be erratic and unsteady. Movement Disorders “Off”phase Movement Disorders “On” phase Diagnosis There are currently no blood or laboratory tests that have been proven to help in diagnosing PD. Therefore the diagnosis is based on medical history and a neurological examination. The disease can be difficult to diagnose accurately. Doctors may sometimes request imaging studies (i.e. MRI’s or brain scans) or laboratory tests in order to rule out other diseases. Differential diagnosis of Parkinson’s diseases. N e u ro lo g ic d is o rd e r M u ltip le s y s te m a tro p h y E s s e n tia l tre m o r H u n tin g to n ’s d is e a s e s T o x in -in d u c e d p a rk in s o n is m D ru g -in d u c e d p a rk in s o n is m C o rtic a l b a s a l g a n g lio n ic d e g e n e ra tio n F e a tu re s P ro m in e n t d y s a u to n o m ia C e re b e lla r d y s p h a n c tio n o r p e rip h . n e u ro p a th y . K in e tic tre m o r p lu s in s ta b ility . F a m ily h is to ry . Y o u n g e r p a tie n t,fa m ily H x , n o tre m o r. E x p o s u re to C O , c y a n id e , M n , M P T P , m e th a n o l o r la c q u e r th in e r. A n tid o p a m in e rg ic e x p o s u re B ila te ra l o n s e t. R e v e rs ib ility . A lie n lim b ,d y s to n ia ,m y o c lo n u s , p a rie ta l s e n s o ry lo s s . Parkinson’s disease - Management Nonpharmacologic Management S u pp o rt P at ient A ssess em oti o n al n eeds P e e r su p p o rt G ro u p su p p o rt(dise a se sta g e a pp ro p ria te P ro fe ssio n al co u n se lling L e g a l/fin a n cia l co u n se lling O ccu p a tio n al co u n se lling (e a rly d ise a se ) Fam ily Nonpharmacologic Management E x e rc is e E d u c a tio n A s s e s s e x e rc is e c a p ac ity a n d lim ita tio ns T ra in in g A e ro b i c S tre n g h th e n in g S tre tc h in g N o n w e ig h t b e a rin g R e g u la r,fo c u s s e d e x e rc ise Nonpharmacologic Management N u t r it io n O b t a in d ie t a r y h is t o ry E d u c a te a b o u t b a la n c e d d ie t N u t r it io n a l c o u n s e llin g Drugs for Parkinson’s disease A m a n ta d in e W e ll to le ra te d , p o s s ib le a n k le e d e m a o r liv e d o re tic u la ris A n tic h o lin e rg ic s G o o d fo r tre m o r A v o id in p a tie n ts a g e 6 5 a n d o ld e r S id e e ffe c ts in c lu d e d ys k in e s ia , c h o re a , d y s to n ia C o n tro v e rs ia l n e u ro p ro te c tiv e a g e n t. M in im a l s ym p to m . b e n e fit H e lp fu l w ith s u p e rim p o s e d re s tle s s le g s sy n d ro m e C a rb id o p a /L e v a d o p a S e le g ilin e B ro m o c rip tin e S e le c tiv e C O M T in h ib ito r A d ju n c tiv e th e ra p y ; in c re a s e s b io a v a ila b ility o f le v a d o p a ; s id e e ffe c ts in c lu d e d ia rrh e a , d y s k in e s ia The Management of Parkinson’s disease P a rk in so n's d ise a se N o n P h a rm a c o lo g ic P h a rm ac o lo g ic E d u c a tion N e uro p ro te ction ? S e le g ilin e S u pp o rt F u n c tion a l im pa irm e nt Yes E x e rc ise NO ? A n tic h olin e rg ics N u trition ? A m a nta d ine D o p a m in e A g o n ists L e vod o pa Dose Dose C o m b in e d the ra py D o p a m ine a g o n ist + L e vod o pa + /C O M T in h ib itor S u rg ic al th e rap y if un a c c e pta b le c o n trol w ith m e d ic a l th e ra py Surgical Therapy- Deep brain stimulation When symptoms are uncontrollable with medical therapy None ablative method is used Transpalntation of fetal nigral cells Thalamotomy Parkinson’s disease - Imaging Predicted developments Research into the causes of Parkinson’s diseases are likely to show that multiple genetic and environmental factors are involved Disease of early onset is more likely to be genetic New drugs acting on both dopaminergic and nondopaminergic transmitter systems will become available over the next 10 years Clinical trials of new drugs with neuroprotective and neurorescue properties are in progress Research At no time in the past have the basic and clinical sciences applied to Parkinson’s disease been so active. Future progress in understanding the causation and pathogenesis of the disorder will permit the development of new treatments that will slow, halt, or even reverse the currently progressive course of Parkinson’s disease.