Parkinson’s Disease: a geriatrics
syndrome
Primary Care
Gerald Jogerst, M.D.
May 16, 2014
Objectives
• Describe a new approach to Parkinson’s
disease.
• Discuss the diagnostic criteria for Parkinson’s
disease.
• Compare conditions misdiagnosed as
Parkinson’s disease.
• List drug and non-drug therapies.
• Provide recommendations for practice.
Parkinson’s Disease
• Described by James Parkinson in 1817
• Kampavata (tremor and akinesia) described in
literature in India 4500-1000 B.C.
• Prevalence of 1 to 2 million people in North
America
• Mortality is 2 to 5 times higher versus agematched controls
• Age is the single most consistent risk factor
Epidemiology
• Occurs throughout the world, in all ethnic groups
• Slight male predominance
• Incidence
– Lowest among Asians and African blacks
– Highest among whites
– African blacks much lower than Afro-Americans
– Exponential increase between ages 65 and 90
– Only 5-10% of patients have symptoms before
age 40 (risk reduction with smoking)
Genetics
• Early studies of twins excluded genetic
contribution
• 1997 study found high concordance among
monozygotic twins (one twin had youngonset disease)
• Linkage to chromosome 2p13 in six families
Pathological Findings
• Progressive death of selected but heterogeneous
populations of neurons
• Sites
– Pars compacta of substantia nigra (dopaminergic)
– Selected aminergic brain stem nuclei
(Catecholaminergic and serotoninergic)
– Nucleus basalis of Meynert (cholinergic)
– Hypothalamus
– Small cortical neurons
– Olfactory bulb, sympathetic ganglia, and
parasympathetic neurons in the gut
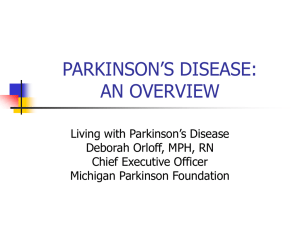
Parkinson’s Disease:
A New Multidisciplinary Approach for this Old Actor
Premotor Phase
Clinically Evident (PD)
Aspecific non-motor
symptoms:
• Hyposmia
• Constipation
• Depression
• Articular pain
• Fatigue
• Orthostatic
Hypotension
Frail “in situ”: mean 10 years
With Complications (PD-D)
Specific motor
symptoms:
Diagnosis
2 yr
Aspecific non-motor
symptoms, specific in
the geriatric setting
• Bradykinesia
(plus at least)
• Rigidity
• Tremor
• Postural
Instability
Frail: mean 10 years
F. Lauretani et al. / Archives of Gerontology and Geriatrics 54 (2012) 242-246
> 1 yr
• Memory Impairment
• Sleep Disorder
• Acute Delirium
• Nocturia
• Dysphagia with
pneumonia
ADL-Disability: mean 7 years
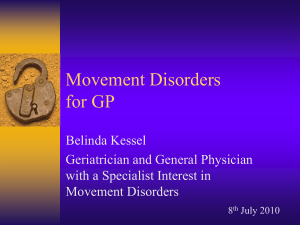
Parkinson’s Disease:
A New Multidisciplinary Approach for this Old Actor
Braak’s Stage 1-2
locus coeruleus
dorsal IX/X nucleus
Clinical Symptoms
Premotor Phase:
• Hyposmia
• Constipation
• Depression
• Articular pain
• Fatigue
• Orthostatic hypotension
Braak’s Stage 3-4
Braak’s Stage 5-6
mesocortex
substantia nigra
locus coeruleus
dorsal IX/X nucleus
Clinical Symptoms
Clinically Evident (PD):
• Bradykinesia
(plus at least)
• Rigidity
• Tremor
• Postural Instability
F. Lauretani et al. / Archives of Gerontology and Geriatrics 54 (2012) 242-246
neocortex (sec. & prim.)
neocortex association
mesocortex
substantia nigra
locus coeruleus
dorsal IX/X nucleus
Clinical Symptoms
With Complications (PD-D):
• Memory Impairment
• Sleep Disorder
• Acute Delirium
• Nocturia
• Dysphagia with pneumonia
Diagnosis
• No biologic marker to confirm the diagnosis
• Underdiagnosis and incorrect diagnosis are
common
• Classic signs and symptoms - tremor, rigidity,
bradykinesia and postural instability
• Best differentiate from other parkinsonisms by:
– Asymmetry
– Resting tremor
– Good response to levodopa
UK Parkinson’s Disease Society clinical
criteria
• Step 1
Bradykinesia
At least one of the following:
Rigidity
4-6 Hz rest tremor
Postural instability not caused by
primary visual, vestibular, cerebellar
or proprioceptive dysfunction
UK criteria
• Step 2
Exclude other causes of parkinsonism
• Step 3: at least 3 of the following criteria:
Unilateral onset, rest tremor, progressive
disorder, asymmetry primarily affecting side of
onset, 70-100% response to levodopa, severe
levodopa induced dyskinesia, levodopa
response for 5 years or more, clinical course of
10 years or more.
Features suggestive of alternative
diagnoses
• Dementia preceding motor symptoms
• In first 3 years: postural instability, freezing,
hallucinations ( not related to medication)
• Supranuclear gaze palsy (downward gaze)
• Severe symptomatic dysautonomia
• Documentation of plausible cause of
parkinsonism ( focal brain lesion, neuroleptic)
Conditions Misdiagnosed as
Parkinson’s Disease
•
•
•
•
•
Essential tremor
Vascular parkinsonism
Drug-induced parkinsonism
Dementia with Lewy bodies
Atypical parkinsonism ( progressive
supranuclear palsy, multisystem atrophy)
Tremor
•
•
•
•
Resting tremor
4-6 Hz
Prominent in hands
Absent in 25%
Tremor
Parkinson’s disease
• Age at onset 55-75 yrs
• Family Hx +/• Frequency (Hz) 4-6
• Characteristics: Suppronation- asymmetric
• Rest -> increase
• Writing dec. (micrographia)
• Face, jaw, lips, chin
Essential tremor
• 10-80 years
• Family Hx ++
• Hz 5-10
• Flexion-extensionsymmetric
• Rest -> decrease
• Increases (tremulous)
• Head, voice
Rigidity
• Increased tone
throughout range
of motion
• Increases when limbs
are moving
• By itself, not disabling
• Spasticity versus rigidity
Bradykinesia
•
•
•
•
One of the more disabling symptoms
Delay in starting all movements
Slowness and poverty of movement
Arrest of ongoing movements
Postural Instability
• Inability to maintain
equilibrium
• Inability to react to
abrupt changes
in position
Modified Hoehn & Yahr Staging
•
•
•
•
•
•
•
•
Stage 0 = No signs of disease
Stage 1= Unilateral disease
Stage 1.5= Unilateral plus axial involvement
Stage 2= Bilateral disease ,no imbalance
Stage 2.5= Mild bilateral, recovery on pull test
Stage 3= postural instability but independent
Stage 4= Severe disability; still able to walk
Stage 5= Wheelchair or bed bound.
Decision to Start Medical Therapy
(consider)
•
•
•
•
Effect of disease on dominant hand
Significant bradykinesia or gait disturbance
Personal philosophy regarding drug use
DEGREE TO WHICH DISEASE EFFECTS
FUNCTION
Protective Therapy
• No proven treatment to slow progression
• Selegiline-ameliorated symptoms/question
of increased mortality
• High dose Vitamin E ineffective
Symptomatic Therapy
• Levodopa remains the most
effective treatment (Sinemet
25/100 TID)
– Most patients benefit
over the entire
course of the illness
– No evidence that it
accelerates the
neuro-degenerative
process
– Increases life expectancy
– Survival reduced if drug
is delayed until
greater disability
Symptomatic Therapy
• Anticholinergics (Artane 0.5-1 mg BID)
• Amantadine (100 mg BID)
• Selegiline (5 mg BID - last dose mid-day)
– All have mild to moderate benefit, but
levodopa or dopamine agonists are
required as disability progresses
• Tolcapone (COMT inhibitor) 100 mg TID
monitor LFT’s
Symptomatic
Therapy
Dopamine agonists
May provide
inadequate benefit
(1/3 of patients
have good
responses)
Always require
supplementary
levodopa but may
be adequate alone
for two to five
years
Infrequent
fluctuations and
dyskinesias
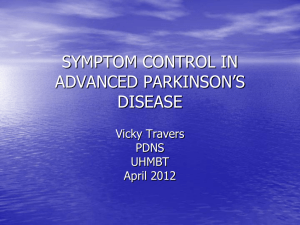
Pramipexole versus levodopa complications
Figure Legend:
Cumulative probability of reaching the first dopaminergic complication (A) and the individual complications wearing off (B),
dyskinesias (C), and freezing (D) by treatment assignment. First dopaminergic complication is defined as the first occurrence of
wearing off, dyskinesias, or on-off fluctuations.
Holloway RG, Shoulson I, Fahn S, et al. Pramipexole vs Levodopa as Initial Treatment for Parkinson Disease: A 4-Year Randomized Controlled Trial Arch Neurol. 2004;61(7):1044-1053.
doi:10.1001/archneur.61.7.1044
Copyright © 2014 American Medical Association. All rights reserved. Date of download: 1/10/2014
Dopamine Agonists
Ergot-derived (lung and cardiac valve fibrosis)
Bromocriptine 20-40 mg/day
Non-Ergot-derived (as first-line and adjunctive
therapy)
Ropinirole
Pramipexole
Rotigotine
up to 24 mg/day,
divided TID or SR
up to 4.5 mg/day,
divided TID or SR
up to 6 mg/24 hr patch
Late Stage Problems
(Disease)
• Motor-dysarthria, freezing of gait, postural
instability with falls
• Nonmotor-dysautonomia, weight loss,
pain, changes in mood or behavior,
sleep disturbance, cognitive dysfunction,
dementia
Late Stage Problems
(Treatment and Disease)
Motor fluctuations: (in 70% treated for 15 years)
• Wearing off of drug effect
• On-off phenomenon
Dyskinesia: (may respond to amantadine)
• Peak-dose dyskinesia
• Diphasic dyskinesia
• Off-period dystonia
Psychiatric disturbances - vivid dreams, visual
hallucinations, mania, hypersexuality, paranoid
psychosis
Surgical Therapy
• Reserved for disabling, medically refractory
symptoms
• Ventrointermediate thalamic nucleus lesions
reduce contralateral arm tremor by 80%
• Pallidotomy - 80% improvement in contralateral
drug-induced dyskinesia (akinesia, rigidity and
tremor reduced)
• Stimulation of subthalamic nuclei-benefits all
aspects of parkinsonism
Deep Brain Stimulation
• For intolerable dyskinesias or motor
fluctuation while on levodopa
• Appropriate candidates have cognition
relatively intact and are less than 70 yrs old.
• Benefit: reduction in levodopa dose,
improvement in off-medication function and
reduced dyskinesias when taking medication.
• Risks: depression, decreased verbal fluency,
increased falls and impulsivity.
Fetal Cell transplantation
• 2 patients
• Intrastriatal grafts of human fetal ventral
mesencephalic tissue (dopaminergic
neuroblasts)
• Assessed 15 & 18 years post graft.
*motor gains over first yr. sustained 18yrs.
*patient remained off dopaminergic drugs.
Kefalopoulou Z et al, JAMA Neurol. 2013.4749
Support Services
• Usual Elder Services
• Specific Disease Oriented Organization
http://www.ninds.nih.gov/disorders/parkinso
ns_disease/org_parkinsons_disease.htm
• Physical therapy – disability improves
• Occupational therapy- in home interventions
• Speech therapy- intensive therapy for 2 week can
improve voice problems and gain may last up to 3
months.
Assisted Devices
Recommendations for Practice
• Carbidopa/levodopa, nonergot dopamine
agonists, or MAOB-I for initial treatment.
• Nonergot dopamine agonists, COMT-I or
MAOB-I added to levodopa to treat motor
complications.
• Consistent, good-quality patient-oriented
evidence.
Recommendations for Practice
• Amantadine for dyskinesias in advanced
disease.
• Deep brain stimulation for functional
impairment despite optimal medical tx.
• PT to improve gait and speech therapy to
improve speech volume.
• Inconsistent patient-oriented evidence.
Recommendations for Practice
• Physicians with limited experience should
refer patients to confirm diagnosis.
• OT may help patients maintain family, social
and work roles, continue ADLs and improve
safety.
• Consensus, usual practice, expert opinion,
case series.
Dementia and Depression
Caregiver burden
Isolation and Loneliness
Parkinson’s Disease:
A New Multidisciplinary Approach for this Old Actor
Premotor Phase
Clinically Evident (PD)
Aspecific non-motor
symptoms:
• Hyposmia
• Constipation
• Depression
• Articular pain
• Fatigue
• Orthostatic
Hypotension
Frail “in situ”: mean 10 years
With Complications (PD-D)
Specific motor
symptoms:
Diagnosis
2 yr
Aspecific non-motor
symptoms, specific in
the geriatric setting
• Bradykinesia
(plus at least)
• Rigidity
• Tremor
• Postural
Instability
Frail: mean 10 years
F. Lauretani et al. / Archives of Gerontology and Geriatrics 54 (2012) 242-246
> 1 yr
• Memory Impairment
• Sleep Disorder
• Acute Delirium
• Nocturia
• Dysphagia with
pneumonia
ADL-Disability: mean 7 years
References
Bega D, Krainc D. Long-term clinical outcomes after fetal cell transplantation in parkinson disease: implications for the
future of cell therapy. JAMA. 2014 Feb 12;311(6):617-8. doi: 10.1001/jama.2013.285516. PMID: 24519302
Follett KA, Weaver FM, Stern M, Hur K, Harris CL, Luo P, Marks WJ Jr, Rothlind J, Sagher O, Moy C, Pahwa R, Burchiel K,
Hogarth P, Lai EC, Duda JE, Holloway K, Samii A, Horn S, Bronstein JM, Stoner G, Starr PA, Simpson R, Baltuch G, De Salles
A, Huang GD, Reda DJ; CSP 468 Study Group. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease. N
Engl J Med. 2010 Jun 3;362(22):2077-2091. doi: 10.1056/NEJMoa0907083. PMID:20519680.
Goetz CG, Poewe W, Rascol O, Sampaio C, Stebbins GT, Counsell C, Giladi N,Holloway RG, Moore CG, Wenning GK, Yahr
MD, Seidl L; Movement Disorder SocietyTask Force on Rating Scales for Parkinson's Disease. Movement Disorder
SocietyTask Force report on the Hoehn and Yahr staging scale: Status and recommendations. Mov Disord. 2004
Sep;19(9):1020-8. PubMed PMID: 15372591.
Jankovic J. Parkinson's disease: Clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008 Apr;79(4):368-376. doi:
10.1136/jnnp.2007.131045. PMID: 18344392.
Lauretani F, Maggio M, Silvestrini C, Nardelli A, Saccavini M, Ceda GP. Parkinson's disease (PD) in the elderly: An example of
geriatric syndrome (GS)? Arch Gerontol Geriatr. 2012 Jan-Feb;54(1):242-246. doi: 10.1016/j.archger.2011.03.002. PMID:
21459464.
Miyasaki JM, Martin W, Suchowersky O, Weiner WJ, Lang AE. Practice parameter: Initiation of treatment for Parkinson’s
disease: An evidence-based review: Report of the Quality Standards Subcommittee of the American Academy of
Neurology. Neurology. 2002 Jan 8;58(1):11-17. PMID: 11781398.
Pahwa R, Factor SA, Lyons KE, Ondo WG, Gronseth G, Bronte-Stewart H, Hallett M, Miyasaki J, Stevens J, Weiner WJ;
Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter: Treatment of Parkinson
disease with motor fluctuations and dyskinesia (an evidence-based review): Report of the Quality Standards
Subcommittee of the American Academy of Neurology. Neurology. 2006 Apr 11;66(7):983-995. PMID: 16606909.
References
Schuepbach WM, Rau J, Knudsen K, Volkmann J, Krack P, Timmermann L, Hälbig TD, Hesekamp H, Navarro SM, Meier N,
Falk D, Mehdorn M, Paschen S, Maarouf M, Barbe MT, Fink GR, Kupsch A, Gruber D, Schneider GH, Seigneuret E, Kistner A,
ChaynesP, Ory-Magne F, Brefel Courbon C, Vesper J, Schnitzler A, Wojtecki L, Houeto JL, Bataille B, Maltête D, Damier P,
Raoul S, Sixel-Doering F, Hellwig D, GharabaghiA, Krüger R, Pinsker MO, Amtage F, Régis JM, Witjas T, Thobois S, Mertens
P,Kloss M, Hartmann A, Oertel WH, Post B, Speelman H, Agid Y, Schade-Brittinger C, Deuschl G; EARLYSTIM Study Group.
Neurostimulation for Parkinson's disease with early motor complications. N Engl J Med. 2013 Feb 14;368(7):610-622. doi:
10.1056/NEJMoa1205158. PMID: 23406026.
Scottish Intercollegiate Guidelines Network. Diagnosis and Pharmacological Management of Parkinson’s disease: A
National Clinical Guideline. Edinburgh: Scottish Intercollegiate Guidelines Network; January 2010.
http://www.sign.ac.uk/pdf/sign113.pdf. Accessed March 8, 2011.
Smeding HM, Speelman JD, Koning-Haanstra M, Schuurman PR, Nijssen P, van Laar T, Schmand B. Neuropsychological
effects of bilateral STN stimulation in Parkinson disease: A controlled study. Neurology. 2006 Jun 27;66(12):1830-1836.
PMID: 16801645.
Stowe R, Ives N, Clarke CE, Deane K; van Hilten, Wheatley K, Gray R, Handley K, Furmston A. Evaluation of the efficacy and
safety of adjuvant treatment to levodopa therapy in Parkinson’s disease patients with motor complications. Cochrane
Database Syst Rev. 2010 Jul 7;(7):CD007166. doi: 10.1002/14651858.CD007166.pub2. PMID: 20614454.
Suchowersky O, Gronseth G, Perlmutter J, Reich S, Zesiewicz T, Weiner WJ; Quality Standards Subcommittee of the
American Academy of Neurology. Practice parameter: Neuroprotective strategies and alternative therapies for Parkinson
disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of
Neurology. Neurology. 2006 Apr 11;66(7):976-982. Erratum in: Neurology. 2006 Jul 25;67(2):299. PMID: 16606908.
The National Collaborating Centre for Chronic Conditions. Parkinson’s Disease: National Clinical Guideline for Diagnosis and
Management in Primary and Secondary Care. London: Royal College of Physicians, 2006.
http://www.nice.org.uk/nicemedia/live/10984/30087/30087.pdf. Accessed March 8, 2011.