Meredith Fonesca of SpeechVive - Chapel Hill Parkinson`s Support
advertisement

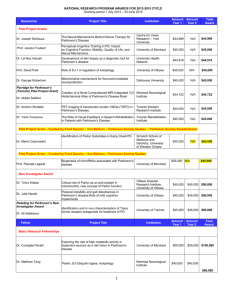
Little Bubbles of Noise Meredith Fonseca, MA CCC-SLP How SpeechVive came to be Dr. Huber at Purdue University began her research in 2005 She studied changes in the voice and asked herself, “How would I respond if my voice changed?” Can’t we do better than this? Traditional Speech Therapy The speech therapist asks the patient to change something such as loudness or clarity The speech therapist cues the patient to make these changes Usually works very well during therapy, but being clearer and louder at home is MUCH harder Dr. Huber first studies how to best cue people with PD A visual cue was used: patients watched a decibel meter and were told to target a number An internal cue was used: thinking about being louder A unique cue was used: the Lombard effect. The Lombard Effect is: When people are in noisy environments they automatically speak louder When people speak clearer because they are in noise When people change their rate when speaking in noise Why did the Lombard effect work best? Because Because it was an external cue the patient was simply responding to a reflex and not relying on training or memory. Dr Huber asks; What if I could create a bubble of noise? It’s It It there when you talk stops when you stop talking is with you outside of therapy when you need it most Engineers are smart Purdue University engineers made Dr. Huber her very first portable bubble of noise. Then they made her 40 more which she used in a 3 year NIH clinical trial SpeechVive Study: Subject Characteristics Age: 67.67 years Time Since Diagnosis: 8.67 years 4 of these subjects had a deep-brain stimulator 1 of these subjects had undergone a pallidotomy and thalamotomy Pre-treatment speech severity: Moderate 14 participants had previous speech therapy Of those 14, 8 had LSVT previously SpeechVive • Patients were fitted with a SpeechVive device • Intensity output of the SpeechVive set to elicit an increase of 3-5 dB from patients during conversation • Wore the device in communicative contexts 2-8 hours/day, 7 days/week • Included reading for 30 minutes per day, 5 days/week • SpeechViveTM intensity output was reset every 2 weeks SpeechVive: Results Summary Patients and caregivers reported improvements in communication 90% patients improved loudness by the end of treatment 75% of patients improved in some way (vocal intensity, rate, and speech clarity) by the end of treatment SpeechVive Treatment You must be assessed by a trained speech therapist You must commit to working with a speech therapist for 6-8 sessions to get the full benefit You must be willing to wear the device Sample Comments about the SpeechVive People no longer spoke over me like I was not there I got more respect from people because I could talk better It was a reminder to speak louder My wife said I pronounced words better, more clearly My kids thought I had a good voice after using the device Who can use SpeechVive? People with softer voices People with changes in rate People with changes in clarity Who can’t use SpeechVive People who can only whisper People with 2 hearing aids How much is it? SpeechVive costs $2495 Payment plans of about $75/ month are available Insurance does not cover the cost of the device Insurance will likely cover the cost of therapy The VA will pay for it. How do I get one? You must be evaluated by a speech therapist to determine if SpeechVive is the right therapy for you Duke University Medical Center Chapel Hill OP Rehab Order it directly from our website SpeechVive will send it to your speech therapist for proper programming Your therapist will fit you with the device during your next appointment. Questions? References 1. Braak, H., Ghebremedhin, E., Rub, U., Bratzke, H., and Del Tredici, K. (2004). Stages in the development of Parkinson's disease-related pathology. Cell and Tissue Research, 318(1), 121-134. 2. Burn, D. (2000). Parkinson's disease: An overview. The Pharmaceutical Journal, 246, 333-337. 3. Countryman, S. and Ramig, L.O. (1993). Effects of intensive voice therapy on voice deficits associated with bilateral thalamotomy in Parkinson disease: A case study. Journal of Medical SpeechLanguage Pathology, 1, 233-249. 4. Darley, F.L., Aronson, A.E., and Brown, J.R. (1969). Clusters of deviant speech dimensions in the dysarthria. Journal of Speech and Hearing Research, 12, 462-496. 5. Darley, F.L., Aronson, A.E., and Brown, J.R. (1969). Differential diagnostic patterns of dysarthria. Journal of Speech and Hearing Research, 12, 246-269. References 6. 7. 8. 9. 10. Darling, M., and Huber, J.E. (2011). Changes to articulatory kinematics in response to loudness cues in individuals with Parkinson’s disease. Journal of Speech, Language, and Hearing Research, 54, 1247–1259. doi: 10.1044/1092-4388(2011/10-0024) Holmes, R.J., Oates, J.M., Phyland, D.J., and Hughes, A.J. (2000). Voice characteristics in the progression of Parkinson's disease. International Journal of Language & Communication Disorders, 35(3), 407-418. doi: 10.1080/136828200410654) Kannus, P., Sievanen, H., Palvanen, M., Jarvinen, T., and Parkkari, J. (2005). Prevention of falls and consequent injuries in elderly people. The Lancet, 366, 1885-1893. Logemann, J.A., Fisher, H.B., Boshes, B., and Blonsky, E.R. (1978). Frequency and cooccurrence of vocal tract dysfunctions in the speech of a large sample of Parkinson patients. Journal of Speech and Hearing Disorders, 43, p. 47-57. MacPherson, M. K., Huber, J.E., & Snow, D.P. (2011). The intonation-syntax interface in the speech of individuals with Parkinson's disease. Journal and of Speech, Language and Hearing Research, 54, 19-32. References 11. 12. 13. 14. 15. Obeso, J.A., Rodriguez-Oroz, M.C., Goetz, C.G., Marin, C., Kordower, J.H., Rodrigues, M., Hirsch, E.C., Farrer, M., Schapira, A.H.V., and Halliday, G. (2010). Missing pieces in the Parkinson’s disease puzzle. Nature Medicine, 16(6), 653-661. Pitts, T., Bolser, D., Rosenbek, J., Troche, M., Okun, M.S., and Sapienza, C. (2009). Impact of expiratory muscle strength training on voluntary cough and swallow function in Parkinson disease. Chest, 135 (5), 1301-1308. Pitts, T., Bolser, D., Rosenbek, J., Troche, M., and Sapienza, C. (2008). Voluntary cough production and swallow dysfunction in Parkinson’s disease. Dysphagia, 23, 297–301. Ramig, Lorraine O., Countryman, S., O'Brien, C., Hoehn, M., & Thompson, L. (1996). Intensive speech treatment for patients with Parkinson's disease: Short- and long-term comparison of two techniques. Neurology, 47, 1496-1504. Ramig, Lorraine O., Countryman, Stefanie, Thompson, Laetitia L., & Horii, Yoshiyuki. (1995). Comparison of two forms of intensive speech treatment for Parkinson disease. Journal of Speech and Hearing Research, 38, 1232-1251. References 16. 17. 18. 19. 20. 21. Sadagopan, N., and Huber, J.E. (2007). Effects of loudness cues on respiration in individuals with Parkinson's disease. Movement Disorders 22, 651-659. Sapienza, C. M. (2008). Respiratory muscle strength training applications. Current Opinion in Otolaryngology Head and Neck Surgery, 16, 216-220. Wood, B.H., Bilclough, J.A., Bowron, A., and Walker, R.W. (2002). Incidence and prediction of falls in Parkinson's disease: a prospective multidisciplinary study. Journal of Neurology, Neurosurgery, and Psychiatry, 72(6), 721-725. Yorkston, K.M., Beukelman, D.R., Strand, E.A., and Bell, K.R. (1999). Management of motor speech disorders in children and adults (Second ed.). Austin: Pro-Ed. Zgaljardic, D.J., Borod, J.C., Foldi, N.S., Mattis, P.J., Gordon, M.F., Geigin, A., and Eidelberg, D. (2006). An examination of executive dysfunction associated with frontostriatal circuitry in Parkinson's disease. Journal of Clinical and Experimental Neuropsychology, 28, 1127-1144. Zgaljardic, D.J., Borod, J.C., Foldi, N.S., and Mattis, P. (2003). A review of the cognitive and behavioral sequelae of Parkinson's disease: Relationship to frontostriatal circuitry. Cognitive and Behavioral Neurology, 16, 193-210.