Dr Michelle Gerstman
advertisement

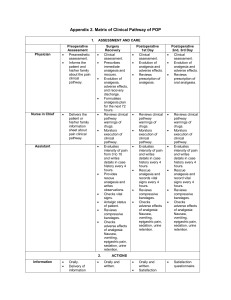
Analgesia Post Emergency Caesarean Section and Educational Intervention in The Developing World Dr Michelle Gerstman Anaesthesia Registrar Alfred Hospital Melbourne Hospital Nacional Guido Valdares (HNGV) Introduction • Caesarean sections amongst the most common surgical procedures performed in the world • Pain relief is a basic human right • Acute pain often poorly managed in developing world • High morbidity associated with pain • Small improvements can potentially have a large positive impact • Simple easy to follow education regarding obstetric postoperative analgesia has wide application WHO: Mother Baby Package: implementing safe motherhood in countries (practical guide). Bosenber, A, Paediatric anaesthesia in developing countries, Current opinion in Anaesthesiology, 2007, 20:204-120 Current Evidence • Minimal in the developing world • Extensive evidence regarding multimodal analgesia in the developed world Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine. Acute Pain Management: Scientific Evidence. 3rd Edition 2010 Hypothesis • Simple education regarding postoperative multimodal analgesia can result in significantly improved pain scores after Emergency Surgery for Caesarean Section in a Developing World setting with limited resources. Study • Prospective audit • Analgesia prescribing patterns and pain intensity after Emergency Cesarean Section for a 48 hour period in two groups. • BEFORE and AFTER simple education regarding multimodal analgesia for prescribers. Analgesic Prescribing • Obstetricians prescribe post op analgesia in Timor • Midwives transcribe and administer • Analgesics available • Any combination • Opioid analgesia is not prescribed Methods • Emergency CS – Pre education - 16 October - 1 December 2009 – Education – Post education - 10 May 2010 - 21 June 2010 • Anaesthesia Registrar/Consultant • Nurse anaesthetists acted as an interpreters Methods: Education • Obstetricians and midwives • Presentation and discussion of pre-education audit data • Agreement that analgesia provision was inadequate • A multimodal analgesia protocol of regular tramadol, paracetamol and ibuprofen was agreed upon Audit data: Primary Measures • • • Analgesia prescribed by the surgical team in surgical notes Actual analgesia transcribed by midwives to drug chart and given on day 1 and day 2 post operatively Pain scores at rest and with movement on day 1 and day 2 post surgery • verbal description of pain (5 categories) from no pain to severe pain then converted to numerical value 1-5 Results • 54 patients were included in the preeducation audit – 54/54 on day 1 – 52/54 on day 2 • 63 in the posteducation audit – 63/63 on day 1 – 55/63 on day 2 Post op analgesia 100% 90% 80% 70% Nil 60% 3 agents 2 agents 50% Single agent 40% 30% 20% 10% 0% Day 1 Pre Day 2 Pre Day 1 Post Day 2 Post Analgesia Pre Education Post Education Day 1 Day 2 Day 1 Day 2 Tramadol alone 62% 12% 32% 11% Paracetamol alone 9% 35% 0% 0% Ibuprofen alone 2% 31% 5% 0% Tramadol/Paracetamol 19% 6% 0% 0% Tramadol/ Ibuprofen 4% 0% 0% 0% Ibuprofen /Paracetamol 0% 4% 3% 74% Tramadol/ Ibuprofen / Paracetamol 0% 0% 57% 11% Nil 4% 12% 0% 2% Mean Pain scores Pre Education Post Education P value Day 1 Rest 2.7 ± 0.9 2.0 ± 0.8 0.0003 Day 1 Movement 3.7 ± 0.8 3.3 ± 0.8 0.0036 Day 2 Rest 2.1 ± 0.8 1.8 ± 0.9 0.0908 Day 2 Movement 3.0 ± 0.8 3.0 ± 0.7 0.8858 Conclusion • Large increase in the use of multimodal analgesia after educational intervention • Significant improvement of early postoperative pain relief • Successful education and implementation of knowledge after one education session Discussion • Less marked improvement with late pain relief – Impact of tramadol? – Rapid mobilization of patients with less use of pre-emptive analgesia? – Loss to follow up? • Language/cultural issues • Challenges with staff changeover • Stoic patients vs. developed world Discussion • Different Anaesthesia Registrar • Audit, not RCT • Small number of patients had midline incision rather than Pfannenstiel incision Future • Further education sessions • Retention of information repeat audit 1 year after post education audit • Written pain protocol displayed in Obstetric ward and OR • Potential application to other surgical specialties • Potential for opioid? Acknowledgements • Dr Eric Vreede – Head Department of Anaesthesia HNGV, Team Leader RACS • Dr Alex Konstantatos – Analysis • Dr Jane Chia – Audit 1 • HNGV Nurse Anaesthetists - Translation services








![medicine16_2[^]](http://s3.studylib.net/store/data/005824937_1-d1fb9b19cd06bd3bedabbcb316965247-300x300.png)