Pain Management in Mass Casualty Events (MCEs)
advertisement
")
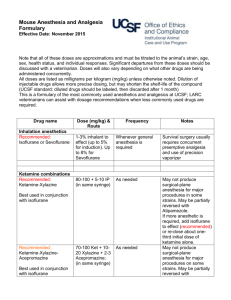
Pain Management in Mass Casualty Events (MCEs) (Civilian) Thom Bloomquist, MSN, CRNA, CH, FAAPM Advanced Anesthesia & Pain Management Bow, NH Pain – MCEs Welcome back Happen not anywhere – but everywhere As Boston knows well Presentation is about out-of-box solutions Hope is that our meeting includes ideas from the experienced and generates other ideas and approaches. Objectives Consider characteristics of disaster Explore pain management in unusual situations Explore adapting analgesia with usual and unusual supplies Explore the effects of crisis on personal/team performance Important! This presentation is explores hypothetical approaches to truly dire situations. This presentation considers off-label use of medications and non-standard practices usually considered beyond bounds of accepted, customary and safe. The author advocates AANA standards and other safe standards of practice whenever possible. Disaster strikes somewhere every day • Cyclone, Indian province of Gujarat: killed >10 000 people • Hurricane Mitch, Nicaragua and Honduras: > 9 000 deaths • Severe floods, Kenya, Myanmar, Somalia, United States, Pacific coast of Latin America (hospitals wiped away) • 9/11/01 • Asian tsunami, spring 2005 • Hurricane Katrina, “Health Care ceased to exist . . .” 2005 • Earthquake, Pakistan, 23,000 deaths, Will you be involved? First – Won’t happen here/to me magical thinking!- (smell the coffee) Next – preplanning limits inevitable chaos Know the factors which inhibit YOU during crisis management, e.g., personal injury, shock, denial, worries about family, team incapacitation Stages of Disaster 1. 2. 3. 4. 5. 6. Warning or threat (maybe) Impact (type and extent) Heroic (heroic actions common) Community solidarity (honeymoon 1 wk6 months) Disillusionment (2 months – 1-2 yrs) Reconstruction or recovery Psychological causalities Can out number physical causalities Ratio – 5-10 to 1 1250 injured - 5,500 sought treatment E.g., Tokyo Sarin attack How long before the Calvary arrives? During 9/11 – re-supply began within 4hr During New York City blackout – 24-48 hrs Indian Ocean tsunami – days to weeks In a “dirty bomb” scenario, decontamination units need arrive/assess/decontam supplies – how long? You may be called upon . . . To provide pain management for large numbers injured and dying. How? Supplies: pluses and minuses (-) Most hospitals went from well-stocked supply rooms to relying on minimal supplies and daily ordering (+) Emergency agencies like F.E.M.A. have pre-positioned “Push Packs” to re-supply in event of local or regional MCEs When you have consumed ~80% of your supplies . . . Organize a scavenging party Pull from discharged patient supplies Closets, drawers, near out-dates Supplies from offices and clinics DPMs, DDSs, Veterinarians Only in dire circumstances . . . Consider crushing Oxycontin or MS Contin for potent immediate release cmpd. Crushing doesn’t change slow-release agents, like Avinza or Kadian. You may need sustained release agents for serious injuries when re-supply is unpredictable. Fentanyl patch FDA cautions against use for acute pain in normal circumstances, but in an MCE . . . Rub skin vigorously with alcohol – more rapid onset Consider methadone Long half-life, but short duration of action Mu & NMDA receptor activity Requires q 4-6 hr dosing Titration trickier than classic opiates (accumulation) Equi-potent dosing Generic Dose Route Duration Morphine Oxycodone Hydromorphone Methadone 10 mg 30mg 1-1.5mg 10-20mg IM/SC PO IM/SC PO 3-6hr 4-6hr 4-5hr 4-6hr See Handout – keep it handy Multi-modal PM NSAID – opiate therapy Combining an NSAID with an opiate can yield effective pain relief with a lower dose of opiate E.g., morphine/toradol or oxycodone/celebrex and…….. Acetaminophin - different Combine acetaminophen with other NSAIDs for improved analgesia Clonidine (Catapres) Will decrease opiate requirement (~50%) IV, transdermal, sublingual IV 0.1-0.3 mg Caution – may cause sedation +/or bradycardia & suppress thermoregulation Combination of clonidine patch and fentanyl patch yields even more potency NMDA blockers, e.g., Ketamine May decrease opiate requirement by 50% Wide range of safety Can be given IV, IM or PO, nasal, rectal To augment narcotic analgesia, consider 10- 20mg added to IM/IV opiate dose NMDA blockers …but if ketamine is running low consider Dextromethorphan (aka – Robitussin cough syrup) 60mg p.o. – q 12 hrs. Anticonvulsants May be helpful in neuropathic pain problems or as part of multi-modal PM, e.g., amputation or brachial plexus avulsion Usually require ramp-up to effective dosage to minimize side effects E.g., start gabapentin - slowly increasing dosage over days Anticonvulsants gabapentin Dose: usually titrate up slowly 100-300 mg at HS Increase by 100-300 mg per day up to 900 mg/day – then . . . Increase by 300 mg/d once per week up to 2400 – 3800 mg Fast ramp up – start at 900/day . . . Other agents for neuropathic pain Carbamzipeine (Tegretol) Lamotrigine (Lamictil) Phenytoin (Dilantin) Pregabalin (Lyrica) New class – Ca+ channel modulators Clinically effective – 50-75mg p.o. Lidocaine drip? (effective but low therapeutic ratio) Neuroaxial opiates 0.2 mg PF morphine – 12-16 hrs – potential to stretch resources 1 – 10ml vial – analgesia- 20 patients! Side effect mgt. Naloxone 0.2 mg/liter of primary IV fluid nalbuphine & butorphanol Out of spinal meds? Meperidine (Demerol) has weak local anesthetic and neural-axial opiate effect sufficient for some procedures. Has been used for C/Ss, minor ortho. Do not use opiates with preservatives – CNS unable to break them down – possible long term toxicity Out of epidural/spinal needles? Caudal Epidural access with any number of needles. Local & regional blocks Regional anesthesia/analgesia, e.g., CPNBs, epidurals, thoracic epidurals CPNBs now used more extensively during combat “nerve blocks in the dirt” After a disaster in India, epidurals were used extensively for pain mgt. Sterile conditions, disinfectants, disposable trays may be in short supply Recording administered dose? During the chaos of an MCE – documentation is important to prevent over/under dosing. You may not have charts Record on triage tag Record with marker on arm/abd/ forehead. Draw picture of fractures Out of block needles? Non-pharmacologic Pain Mgt. Splint/stabilize fractures to prevent pain spikes Ice/cold application Protect wounds from jostling/additional injury during evac When possible, arrange for comfortable positioning (try a backboard for 30 min and tell me how you feel) Hypnosis WW II –south pacific Arab spring Pain – MCEs Welcome back Happen not anywhere – but everywhere As Boston knows well Presentation is about out-of-box solutions Psychological impacts Huge factor Psych casualties – 3-4 x physical! Shock, disbelief, disorientation, grief – the full range. Personal/team/patient mgt.? Non-clinical issues Consumption or theft of limited resources Security? Well-meaning volunteers? Credentials of volunteers? (even experienced professionals) Giving orders/delegating in an MCE Your staff may be on the verge of sensory overload (perceptual narrowing) Give precise instructions in simple unambiguous terms & have them repeated back Consider F.E.M.A. Incident Command System (online & free) Use the K.I.S.S. system Other specialties: how can they help? Veterinarians Supplies – Isoflorane, benzo’s, barbiturates, propofol Skills – frequently experienced surgeons – IVs, suturing, casting Other specialties: how can they help? Dentists Supplies Skills – local anesthetics – suturing Others supplies and skills? Podiatrists -same Pharmacists – extra supplies? Caregiver Impact Triage-Triage-triage (study again and once per year) Do what you can –while you can Thank you - Questions? Your turn . . . How else could we record dosages if not charts? Other sources of pain management supplies? Other professional groups that could be recruited?