Dosha Cummins, PharmD - Arkansas Academy of Family Physicians
advertisement

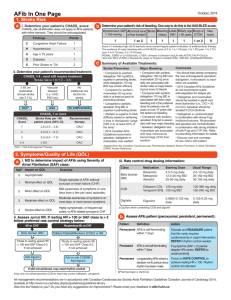
Advancements In Anticoagulation June 14, 2013 Dosha Cummins, PharmD, BCPS UAMS Northeast Associate Professor Dept. of Pharmacy Practice Dept. of Family and Preventive Medicine Direct Thrombin Inhibitors IV • Bivalirudin (Angiomax®) • PCTA • Desirudin (Iprivask®) • DVT/hip • Argatroban (Argatroban™) • HIT Oral • Dabigatran (Pradaxa®) • Prevention of stroke in a fib- 10/10 Dabigatran (Pradaxa®) • Prodrug • Dabigatran etexilate → hydrolyzed by esterase to dabigatran • Tartaric acid in product improves absorption • 80% renally eliminated • 68% dialyzed at 4 hours • P-glycoprotein (P-gp) pumps • (rifampin, ketoconazole; adjustment not required for verapamil, amiodarone, quinidine, clarithromycin) • Discard 4 months after bottle opened Dabigatran (Pradaxa®) • To prevent stroke in non-valvular atrial fibrillation • RE-LY Trial • N=18,113 • Mean CHAD2 score 2.1 • Mean age 72 years • Excluded: stroke within 14 days prior or severe stroke within 6 months • Dabigatran 110mg bid vs dabigatran 150mg bid vs dose-adjusted warfarin Dabigatran (Pradaxa®) • Results • Primary endpoint stroke/systemic embolism • 1.11% dabigatran 150mg bid vs 1.71% warfarin • NNT for 1 year to prevent 1 stroke/systemic embolism = 167 • About 6 events prevented per 1000 patients treated for 1 year • Adverse Effects • Intracranial bleed: NNT=227 • GI bleed: NNT= 204 Dabigatran (Pradaxa®) • Results • Primary endpoint stroke/systemic embolism • 1.11% dabigatran 150mg bid vs 1.71% warfarin • NNT for 1 year to prevent 1 stroke/systemic embolism = 167 • About 6 events prevented per 1000 patients treated for 1 year • Adverse Effects • Intracranial bleed: NNT=227 • GI bleed: NNT= 204 • “Suggested” over warfarin (Grade 2B) – CHEST 2012 Dabigatran (Pradaxa®) • Dosing for prevention of stroke in atrial fibrillation • CrCl > 30mL/min - 150mg bid (with or without food) • CrCl 30-50mL/min on ketoconazole or dronedarone, consider adjusting to 75mg bid • CrCl 15-30mL/min – 75mg bid; avoid P-gp inhibitors • CrCl <15mL/min or dialysis – avoid • Avoid with P-gp inducers (rifampin) Direct Xa Inhibitors IV Oral • Fondaparinux (Arixtra®) • Rivaroxaban (Xarelto®) • VTE • Ortho VTE prophylaxis-7/11 • Prevention of stroke in a fib-11/11 • PE/DVT treatment-11/12 • Apixaban (Eliquis®) • Prevention of stroke in a fib-12/12 Rivaroxaban (Xarelto®) • Absorption – dose dependent • 10mg (80-100%) • 20mg (66%) – increased by 76% with food • Drug released in stomach (AUC decreases by 29% via feeding tube into proximal small intestine) • Metabolized in liver by CYP3A4/5 and CYP2J2; P-gp substrate • Avoid meds that can inhibit/induce both systems (erythromycin, clarithromycin, ketoconazole, fluconazole; rifampin, phenytoin, CBZ, St. John’s Wort) • Not dialyzable Rivaroxaban (Xarelto®) • To prophylaxis for DVT/PE in knee and hip replacement Population Comparer Results NNT RECORD 1 Hip arthroplasty 40mg enoxaparin 1.1% vs 3.7% 38 (at 35 days) RECORD 3 Knee arthroplasty 40mg enoxaparin 9.6% vs 18.9% 11 (at 2 weeks) RECORD 4 Knee arthroplasty 30mg bid enoxaparin 6.9% vs 10.1% 32 (at 17 days) Rivaroxaban (Xarelto®) • To reduce the risk of stroke and embolism in atrial fibrillation • ROCKET-AF Trial • N= 14,264 • Mean CHAD2 score 3.5 • Mean age 73 years • Excluded: stroke within 14 days or TIA within 3 days, GI bleed within 6 months • Rivaroxaban 20mg* daily vs dose-adjusted warfarin * 15mg daily if CrCl 30-49mL/min Rivaroxaban (Xarelto®) • Results • Primary endpoint stroke/systemic embolism • 2.1% rivaroxaban vs 2.4% warfarin • NNT for 1 year to prevent 1 stroke/systemic embolism = 330 • About 3 events prevented per 1000 patients treated for 1 year • Adverse Effects • Intracranial bleed: NNT= 500 • GI bleed: NNT= 100 Rivaroxaban (Xarelto®) • To treat DVT, PE and reduce the risk of recurrence • EINSTEIN-PE Trial • N=4832 with confirmed, symptomatic PE • 15mg rivoroxaban bid x 3 weeks, then 30mg daily vs enoxaparin + vitamin K antagonist • Randomized to 3, 6 or 12 months • Primary endpoint: symptomatic, recurrent VTE • 2.1% rivaroxaban vs 1.1% standard therapy • NNT= 333 (mean study duration ∼ 263 days) • NNT for major bleeding = 91 Rivaroxaban (Xarelto®) • Acute coronary syndrome – ATLAS ACS • June 2012 • FDA rejected 6:4 • Reduced risk of stroke by 15% • 2.5 or 5 mg bid vs placebo • N=15,526 • FDA cited incomplete outcome data for 12% of study participants Rivaroxaban (Xarelto®) • Ortho VTE prevention: • Hip: 10mg/d x 35 days (with/without food) • Knee: 10mg/d x 12 days (with/without food) • CrCl < 30mL/min - avoid • Stroke prevention in atrial fibrillation: • 20mg/d daily with evening meal • CrCl 15-50mL/min - 15mg/d with evening meal • CrCl <15mL/min – avoid • PE/DVT treatment: • 15mg bid x 3 weeks, then 20mg daily • CrCl15-49mL/min – 15mg bid x 3 weeks, then 20mg daily • CrCl <15mL/min – avoid Apixaban (Eliquis®) • Absorbed in small intestine and colon • Metabolized by CYP3A4 and a P-gp substrate • Reduce dose to 2.5mg bid if on ketoconazole, itraconazole, clarithromycin (avoid if already on apixaban) • Avoid dual inducers: rifampin, CBZ, phenytoin, St. John’s Wort • Not dialyzable Apixaban (Eliquis®) • To reduce the risk of stroke and embolism in atrial fibrillation • ARISTOTLE Trial • N= 18,201 • Mean CHAD2 score 2.1 • Mean age 70 years • Included: • More than 1: ≥ 75 years, prior stroke/TIA/systemic embolus; symptomatic CHF, DM, HTN, female • Excluded: CVA within 7 days, ASA dose ≥ 165mg/day • Apixaban 5 mg bid* vs dose-adjusted warfarin *2.5mg bid if ≥ 2 of the following: ≥80 years, ≤60 kg, or Scr ≥ 1.5mg/dL Apixaban (Eliquis®) • Results • Primary endpoint stroke/systemic embolism • 1.27% apixaban vs 1.6% warfarin • NNT for 1 year to prevent 1 stroke/systemic embolism = 303 • About 3 events prevented per 1000 patients treated for 1 year • Adverse Effects • Intracranial bleed: NNT= 212 • GI bleed: NNT= NS Apixaban (Eliquis®) • Stroke prevention in atrial fibrillation: • 5mg bid • 2.5mg bid ≥ 2 of the following: • ≤60kg, ≥80yrs, Scr ≥1.5mg/dL Prosthetic Heart Valve Patients • Pradaxa® • Contraindicated for patients with mechanical heart valve - December 2012 • RE-ALIGN Trial • Dabigatran patients more likely to experience stroke or major thromboembolic event vs warfarin • Dabigatran patients had more bleeding after valve surgery • Xarelto® & Eliquis®- not recommended Atrial fibrillation Per year NNT to prevent an event Additional events prevented per 1000 patients NNT for Major Bleed TTR (Warfarin Patients) Dabigatran (CHAD2- 2.1) 167 ∼6 400 64% Rivaroxaban (CHAD2 - 3.5) 330 ∼3 500 55% Apixaban (CHAD2 -2.1) 303 ∼3 104 62% TTR – Time in Therapeutic Range Risk of Bleeding with Antithrombotic Treatment 4.5 4.03 4 3.57 RR (relative risk) 3.5 3 2.5 1.75 2 1.45 1.5 1 1.91 0.96 1.0 0.5 0 ASA warfarin Plavix® warfarin Plavix® warfarin warfarin + + + + ASA ASA Plavix® Plavix® + Arch Intern Med 2010;170(16):1433-1441 ASA Dabigatran Rivaroxaban Apixaban Absorption and crushing Do not break/chew Can crush and suspend in 50ml of water to administer via NG or gastric tube; follow with feeds N/A Affect of food on bioavailability None 20mg dose – food increases None Product Monitoring New Agents • INR – specifically calibrated to monitor vitamin K antagonists • New agents affect, but no correlation with efficacy or safety • May affect first 2 days when transitioning to warfarin • Direct thrombin inhibitors (dabigatran) • Diluted thrombin time (TT) evolving • Factor Xa inhibitors (rivaroxaban & apixaban) • PT affected more than PTT • Linear response, but reagent specific Reversing New Agents • Dabigatran (Pradaxa®) • 60% dialyzed • Distributes to tissue early, then serum rebound • Rivaroxaban (Xarelto®) & Apixaban (Eliquis®) • Not dialyzed • Prothrombin Complex Concentrate (PCC) • Factor VII General Reminder for New Agents • Avoid “indication creep” • Avoid in patients with a prosthetic heart valve • Be vigilant in dosing adjustments • Changes in renal function • Changes in indications (post-ortho patient diagnosed with atrial fibrillation) • Compliance is extremely important because of short duration of effects SPECIFIC POPULATIONS Atrial fibrillation and Stents • Chest. 2012; 141(suppl 2): e531S-e575S • CHAD2 score ≥ 2 (Grade 2C) • Triple therapy duration (warfarin + DAPT) • Bare-metal stent – 1 month • Drug-eluting stent – 3 months • After triple therapy, continue warfarin and a single anti-platelet agent until 12 months after stent placement • After 12 months, warfarin alone • CHAD2 score 0-1 (Grade 2C) • DAPT for 12 months Atrial fibrillation and ACS • CHADS2 score ≥ 1 with ACS not receiving stents • Warfarin plus single anti-platelet therapy for the first 12 months rather than DAPT or triple therapy x12 months (Grade 2C) • CHADS2 score of 0 or 1 • DAPT recommended over warfarin plus single antiplatelet therapy or triple therapy x 12 months (Grade 2C). • After the first 12 months, antithrombotic therapy is suggested as for patients with AF and stable coronary artery disease (eg, warfarin only) (Grade 2C) Atrial fibrillation and Stable CAD • If on warfarin and no ACS within past year, warfarin only recommended over warfarin plus aspirin. (Grade 2C) PRIMARY PREVENTION WITH ASA USPSTF¶ Men Women MI <49 years: ASA not recommended Age 45-79 years: ASA benefit outweighs GI bleed risk ASA not recommended ASA not recommended <55 years: ASA not recommended 55-79 years: ASA if benefit outweighs GI bleed risk Stroke ADA# Diabetics >50 years* Diabetics >60 years* *Consider ASA (81-162 mg/day) if ≥ 1 risk factor (family history or CVD, HTN, smoking, dyslipidemia or albuminuria) ¶AHRQ Publication No. 09-05129-EF-2, March 2009; # Diabetes Care. 2013; (36):S Outpatient PE Treatment • CHEST 2012;141;e419S-e494S • 5.5 In patients with low-risk PE whose home circumstances are adequate, we suggest early discharge over standard discharge (eg, after 5 days of treatment) Grade 2B Potential Outpatient Candidates Based on acute symptomatic PE, PESI – PE Severity Index 1. Clinically stable with good cardiopulmonary reserve • PESI score <85 or simplified PESI of 0 if none of: • SBP < 100 • Recent bleeding • Severe chest pain • Platelets <70,000/mm3 (on anticoagulant therapy) • Severe hepatic or renal disease 2. Good social support with ready access to medical care 3. Expected to be compliant with follow-up LMWH Dosing • 5.4.2. In patients with acute PE treated with LMWH, we suggest once- over twice-daily administration (Grade 2C) . • Remarks: This recommendation only applies when the approved once-daily regimen uses the same daily dose as the twice-daily regimen (ie, the once-daily injection contains double the dose of each twice-daily injection). It also places value on avoiding an extra injection per day. Avoid ‘Bridging a Bridge” … using newer anticoagulants instead of heparin while waiting for a therapeutic INR Clopidogrel: Treatment Failure vs Resistance • Treatment failure (clinical observation) • Non-compliance • Individual variation in ADP-mediated platelet response • Resistance • In-complete blockade of P2Y12 receptor • Proton pump inhibitors • Clopidogrel label • Includes omeprazole & esomeprazole as DI’s • Pantoprozole will be moved to preferred status by AR Medicaid July 9th, esomeprazole moved to nonpreferred Genotype Variability • P2Y12 receptor variability • Drug transport (MDR1) • CYP2C19 has >25 known variant alleles • Most common dysfunction • ∼15% of Caucasians and Africans • 29-35% Asians Clin Pharmcol Ther 2011;90(2): 329-332 • Testing not universally recommended by ACC • ACCF/ACG/AHA 2010 Expert Consensus Document on the Concomitant Use of PPI’s and Thienopyridones. JACC 2010; 56(24): 2051-2066 VerifyNow® Results % Inhibition Threshold PRU Threshold 10 259 20 237 30 214 40 187 50 159 60 131 ADP 2Y12 assay • Light transmission platelet aggregometry endorsed by platelet specialists as standard of care • Available assays correlate poorly with each other and only modestly predict clinical outcome (sensitivity 5563%, specificity 59-64%) • Other medications can interfere with assays • Lack of universally accepted cut-off value for resistance • “Bedside monitoring” and dose adjustment hasn’t been shown to be beneficial (NEJM 2012;367:2100-2109) References RE-LY Connolly, SJ, Ezekowitz MD, Yusuf S, et al. NEJM 2009;361:1139-1151. RECORD 1 Eriksson BI, Borris LC, Friedman RJ, et al. NEJM 2008;358:2765-75. RECORD 3 Lassen MR, Angeo W, Borris LC, et al. NEJM 2008;358: 2776-86. RECORD 4 Turpie AG, Lassen MR, Davidson BL, et al. Lancet 2009;373:1673-80. ROCKET AF Patel MR, Mahaffey KW, Garg J, et al. NEJM 2011; 365:883-891. EINSTEIN-PE Einstein investigators. NEJM 2012;366:1287-97. ARISTOTLE Granger CB, Alexander H, McMurray JJV, et al. NEJM 2011. 365:981- 992 Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141(suppl 2): http://www.mdcalc.com/simplified-pesi-pulmonary-embolism-severity-index/ Collet JP, Cuisset T, Range G, et al. NEJM 2012;367:2100-2109