Chair of Medical Biology, Microbiology, Virology,
and Immunology
Picornaviruse Family
Lecturer Prof. S.I. Klymnyuk
Picornaviruses are small (20-30 nm) and nonenveloped and contain
a single-stranded RNA genome (MW 2-3 x 106). The nucleocapsid
has cubic symmetry and contains 32 spherical subunits
(capsomeres). Virus maturation takes place in the cytoplasm.
Enteroviruses and rhinoviruses commonly infect humans.
Enterovirus. Enteroviruses exist in many animals, including humans,
cattle, pigs, and mice. Enteroviruses of human origin include the
following:
(1) Polioviruses, types 1-3.
(2) Coxsackie viruses of group A, types 1-24.
(3) Coxsackie viruses of group B, types 1-6.
(4) Echoviruses, types 1-34.
(5) Enteroviruses, types 68-71. Since 1969, new enterovirus types
have been assigned enterovirus type numbers rather than being
subclassified as coxsackie-viruses or echoviruses. The vernacular
names of the previously identified enteroviruses have been retained.
Genera of Picornaviruses
Enterovirus
•Polio
•Coxsackie A and B
•Echo
•Other enteroviruses
Diseases of the human (and other) alimentary tract
(e.g. polio virus)
Rhinovirus
Disease of the nasopharyngeal region (e.g. common
cold virus)
Cardiovirus
Murine encephalomyocarditis, Theiler's murine
encephalomyelitis virus
Aphthovirus
Foot and mouth disease in cloven footed animals
Hepatovirus
Human hepatitis virus A
Others
Drosophila C virus, equine rhinoviruses, cricket
paralysis virus
Clinical Picornavirus Syndromes
Virus
Diseases (Virus Type)
Polioviruses (types 1- Undifferentiated febrile illnesses (types 1-3)
3)
Aseptic memingitis (types 1-3)
Paralisis and encephalitic diseases (types
1-3)
Coxsackievirus group Acute hemorrhagic conjunctivitis (type 24
A (A1-A, A-24)*
variant)
Herpangina (types 2-6, 8, 10, 22)
Exanthem (types 4, 5, 6, 9, 16)
Hand-foot-mouth disease (types 5, 10, 16)
Aseptic memingitis (types 1, 2, 4-7, 9, 10,
14, 16, 22)
Paralysis and encephalitic diseases
(occasional types 4, 7, 9, 10)
Hepatitis (types 4, 9)
Virus
Diseases (Virus Type)
Coxsackievirus group Upper and lower respiratory
illnesses
A (A1-A, A-24)*
(types 9, 10, 16, 21, 24 variant)
Lymphonodular pharyngitis (10)
Infantile diarrhea (types 18, 20, 21, 22, 24
variant)
Undifferentiated febrile illnesses (types 1-6)
Pleurodinia (types 1-5)
Pericarditis, myocarditis (types 1-5)
Aseptic meningitis types (106)
Paralysis and encephalitic diseases
(occasional types 1-5)
Severe systemic infection in infants,
meningoencephalitis
and
myocarditis
(types 1-5)
Upper and lower respiratory
illnesses
(types 4, 5)
Exanthem, hepatitis, diarrhea (types 5)
Virus
Echoviruses (1-7, 9,
11, 29-33)*
Diseases (Virus Type)
Aseptic meningitis (many seroypes )
Paralysis and encephalitic diseases
(occasional types 1, 2, 4, 6, 7, 9, 11, 14-16,
18, 22, 30)
Exanthem (types 1-9, 11, 14, 16, 18, 19,
25, 30, 32)
Hand-foot-mouth disease (19)
Pericarditis, myocarditis (types 1, 6, 9, 19,
22)
Upper and lower respiratory
illnesses
(types 4, 9, 11, 20, 22, 25)
Neanatal diarrhea (types 11, 14, 18, 20, 32)
Epidemic mialgia (types 1, 6, 9)
Hepatitis (types 4, 9)
Virus
Diseases (Virus Type)
New enteroviruses
Pneumonia and bronchiolitis (types 68, 69)
Acute hemorrhagic conjunctivitis (type 70)
Aseptic meningitis, meningoencephalitis
Hand-foot-mouth disease (71)
Hepatitis (type 72)
Rhinoviruses (1-115)
Upper and lower respiratory illnesses
(types 1-115)
Hepatovirus
(Hepatitis A)
Gastroenteritis and hepatitis A
* Reclassification of coxsackievirus A23 as echovirus 9,
echovirus 8 as 1, echovirus 10 as reovirus, echovirus 28 as
rhinovirus type 1A, and echovirus 34 as coxsackievirus A24.
Properties of enteroviruses
Property
Enteroviruses
Size (nm)
Capsid
form
Polypeptide
RNA type
RNA molecular weight
Acid
22-30
Optimal temperature for
growth(oC)
Density in caesium chloride
(g/m)
37
Icosahedral
VP1, VP2, VP3, VP4
SS-PS
2000,000-2600,000
Stable*
1.34*
Epidemic Poliomyelitis Virus
Poliomyelitis is an acute infectious disease that in its serious
form affects the central nervous system. The destruction of
motor neurons in the spinal cord results in flaccid paralysis.
However, most poliovirus infections are subclinical.
In spite of the fact that poliomyelitis is one of the most ancient
contagious diseases, its infectious nature was ascertained only
in 1905 by O. Wickman who investigated a poliomyelitis
epidemic in Sweden.
In 1908-09, K. Landsteiner and E. Popper proved poliomyelitis
to be of viral etiology. They produced a febrile disease in
monkeys by injecting an emulsion prepared from the spinal
cord of a fatal case of poliomyelitis. The animals displayed
typical manifestations of poliomyelitis accompanied with flaccid
paralysis. The virus was isolated in tissue culture in 1949 by
J. Enders.
Poliomielitis virus
POLIOMYELITIS
• “Picornavirus”
• 3 types: Poliovirus
1,2,3
• Ingested, spread by
faeco-oral route:
Commoner in areas of
poor sanitation
• Infants protected by
maternal antibodies
Virus Replication. After attaching to virus receptors
(which seem to be controlled in humans by genes on
chromosome 19). Poliovirus RNA serves both as its
own messenger RNA and as the source of the
genetic information. Viral protein is synthesized on
polysomes held together by viral RNA.
Guanidine in concentrations greater than 1 mM and
2-(alpha-hydroxybenzyl)-benzimidazole
inhibit
poliovirus multiplication in tissue culture. Guanidine
acts by inhibiting the release of newly made viral
RNA from the replicative complex.
Important Characteristics
• D or N antigen:
Type specific
(CFA)
• C or H antigen:
Common
antigen (CFA)
• Type 1-3
Resistance. The virus is extremely resistant to
photodynamic inactivation. It survives in sterile water
at room temperature for a period of more than 100
days, in milk for 90 days, in faeces in the cold for
more than 6 months, and in sewage for several
months. It withstands exposure to 0.5-1 per cent
phenol solutions and remains viable for several
weeks at pH 3.8-8.5.
The poliomyelitis virus is sensitive to calcium chlorate
lime, chloramine, formalin, potassium permanganate,
and hydrogen peroxide solutions. It is rapidly killed on
boiling.
Pathogenesis
1. Source of infection: Apparent and subclinical
patients
2. Incubation: 7-14 days
3. Pathogenesis: Only much less than 0.1% subjects
exposed to polio virus form the flaccid paralysis
Transmission
• Fecal – oral route: poor hygiene, dirty
diapers (especially in day-care settings)
• Ingestion via contaminated food and water
• Contact with infected hands
• Inhalation of infectious aerosols
Clinical Syndromes
• Asymptomatic illness: 90%
• Abortive poliomyelitis, the minor illness: 5%
infected people
• Nonparalytic poliomyelitis or aseptic meningitis:
1%-2% of patients with poliovirus infections.
• Paralytic polio, the major illness: 0.1% to 2%of
persons with poliovirus
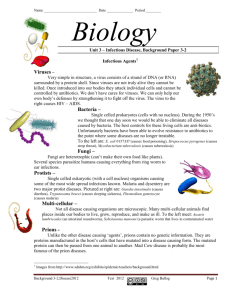
Child with polio sequelae
Polio in the United States, 1952
Lab Diagnosis
• Definitive diagnosis is made by osolation of the
virus from stool, CFS, oropharyngeal secretions
• Cell culture involves fibroblastic MRC-5 cells
• CPE is usually evident within 36 hours
• Serotyping is based on neutralization of CPE by
standardized antisera using intersecting pool
followed by specific sera.
• ELISA
• IFA
• neutralizing Test
• CFT
Immunity
•
sIgA and neutralizing antibody (IgG,
IgA, IgM) persist for life span
Progress Toward Polio Eradication: 1988
~350,000 cases
1000 cases/day worldwide
125 endemic countries
Progress Toward Polio Eradication: 1998
6349 cases
~40 endemic countries
Progress Toward Polio Eradication: 2004
1267 cases
<10 endemic countries
~10 re-infected countries
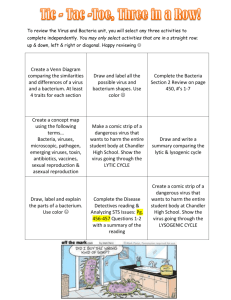
Wild Poliovirus*, 04 May 2004 to 03 May 2005
Wild virus type 1
Wild virus type 3
Wild virus type 1 & 3
Endemic countries
Re-established transmission countries
Case or outbreak following importation
*Excludes viruses detected from environmental
surveillance and vaccine derived polio viruses.
Data in WHO HQ as of 03 May 2005
The boundaries and names shown and the designations used on this map do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning
the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
WHO 2005. All rights reserved
Prevention
• Both oral polio vaccine (OPV live,
attenuated, Sabin, 1957) and inactivated
poliovirus vaccine (IPV, Salk, 1954) are
avilable
• ****IPV is used for adult immunization
and Immunocopromised patients
Advantages and disadvantages of opv
• Advantages
• Effectiveness
• Lifelong immunity
• Induction of secretory antibody response similar to that
of natural infection
• Possibility of attenuated virus circulating in community
by spread to contacts (indirect immunization)(herd
immunity)
• Ease of administration
• Lack of need for repeated boosters
• Disadvantages
• Risk of vaccine-associated poliomyelites in vaccine
recipients or contacts
• Spread of vaccine to contacts without their consent
• Unsafe administration for immunodeficient patients
Advantages and disadvantages of IPV
• Advantages
•
•
•
•
Effectiveness
Good stability during transport and in storage
Safe administration in immunodeficient patients
No risk of vaccine-related disease
• Disadvantages
• Lack of induction of local (gut) immunity
• Need for booster vaccine for lifelong immunity
• Fact that injection is more painful than oral
administration
• Fact that higher community immunization levels
are needed than with live vaccine
IPV (Salk Vaccine) Field Trials, 1954
Albert Sabin
USA, 1961
Uttar Pradesh, India, 2000
COXSACKIEVIRUSES
The coxsackieviruses comprise a large subgroup of the
enteroviruses. They produce a variety of illnesses in
human beings, including aseptic meningitis, herpangina,
pleurodynia, hand, foot, and mouth disease, myo- and
pericarditis, common colds, and possibly diabetes.
Coxsackieviruses have been divided into 2 groups, A and
B, having different pathogenic potentials for mice.
Coxsackie B viruses are the most commonly identified
causative agents of viral heart disease in humans.
Properties of the Viruses
General Properties: Coxsackieviruses are typical
enteroviruses, with a diameter of 28 nm.
Features of coxsackievirus infection in
the labortory
Types Growth in MK Effect in
cell culture sucking mice
Coxsackie A virus 1-24 a
Coxsackie B virus 1-6
+
+
Paralysis
Spasticity
MK , monkey kidney
a Coxsackievirus A23 now classified as echovirus 9
Group A viruses produce widespread myositis in the
skeletal muscles of newborn mice, resulting in flaccid
paralysis without other observable lesions.
Group B viruses may produce focal myositis, encephalitis,
and, most typically, necrotizing steatitis involving mainly fetal
fat lobules. The genetic makeup of inbred strains determines
their susceptibility to coxsackie B viruses. Some B strains
also produce pancreatitis, myocarditis, endocarditis, and
hepatitis in both suckling and adult mice. Corticosteroids
may enhance the susceptibility of older mice to infection of
the pancreas. Normal adult mice tolerate infections with
group B coxsackieviruses. However, severely malnourished
or immunodeficient mice have greatly enhanced
susceptibility.
Features of coxsackievirus
infection in man
• Coxsackievirus A 1-24
• Asptic meningitis
• Febrile illness
• Herpangina
• Hand-foot-and-mouth disease
• Coxsackievirus B 1-6
• Neonatal disease
• Myocarditis, hepatitis
• Meningitis
Pathogenesis of enterovirus infection
Replication in
oropharynx
Rhino,echo,
coxsackie,polio
Primary viremia
Secondary viremia
Target Tissue
Skin
Muscle
Brain
Meninges
Liver
Echo
Echo
Polio
Echo
Echo
Coxsackie
Coxsackie
Coxsackie
Polio
Coxsackie
A
A, B
Coxsackie
Clinical
Findings.
The
incubation
period
of
coxsackievirus infection ranges from 2 to 9 days. The
clinical manifestations of infection with various coxsackie
viruses are diverse and may present as distinct disease
entities.
A. Herpangina: This disease is caused by certain group A
viruses (2, 4, 5, 6, 8, 10), There is an abrupt onset of fever,
sore throat, anorexia, dysphagia, vomiting, or abdominal
pain. The pharynx is usually hyperaemic, and
characteristic discrete vesicles occur on the anterior pillars
of the fauces, the palate, uvula, tonsils, or tongue. The
illness is self-limited and most frequent in small children.
B. Summer Minor Illnesses: Coxsackieviruses are often
isolated from patients with acute febrile illnesses of short
duration that occur during the summer or fall and are
without distinctive features.
Exanthems – Rubelliform rashes
C. Pleurodynia (Epidemic Myalgia, Bornholm
Disease): This disease is caused by group B viruses.
Fever and chest pain are usually abrupt in onset but are
sometimes preceded by malaise, headache, and
anorexia. The chest pain may be located on either side or
substernally, is intensified by movement, and may last
from 2 days to 2 weeks. Abdominal pain occurs in
approximately half of cases, and in children this may be
the chief complaint. The illness is self-limited, and
recovery is complete, although relapses are common.
D. Aseptic Meningitis and Mild Paresis: This syndrome
is caused by all types of group B coxsackieviruses and by
coxsackie viruses A7, A9, and A24. Fever, malaise,
headache, nausea, and abdominal pain are common early
symptoms. Signs of meningeal irritation, stiff neck or back,
and vomiting may appear 1-2 days later. The disease
sometimes progresses to mild muscle weakness
suggestive of paralytic poliomyelitis. Patients almost
always recover completely from nonpoliovirus paresis.
Early in aseptic meningitis, the cerebrospinal fluid shows
pleocytosis (up to 500 cells/mcL) with up to 50%
polymorphonuclear neutrophils.
E. Neonatal Disease: Neonatal disease may be caused
by group B coxsackieviruses. with lethargy, feeding
difficulty, and vomiting, with or without fever. In severe
cases, myocarditis or pericarditis can occur within the
first 8 days of life; it may be preceded by a brief episode
of diarrhea and anorexia. Cardiac and respiratory
embarrassment are indicated by tachycardia, dyspnea,
cyanosis, and changes in the electrocardiogram. The
clinical course may be rapidly fatal, or the patient may
recover completely. The disease may sometimes he
acquired transplacentally. Myocarditis has also been
caused by some group A coxsackieviruses.
F. Colds: A number of the enteroviruses have been
associated with common colds; among these are
coxsackieviruses A10, A21, A24, and B3.
G. Hand, Foot, and Mouth Disease: This disease has
been associated particularly with coxsackievirus A16, but
A4, A5, A7, A9, and A10 have also been implicated.
Virus may be recovered riot only from the stool and
pharyngeal secretions but also from vesicular fluidThe syndrome is characterized by oral and pharyngeal
ulcerations and a vesicular rash of the palms and soles
that may spread to the arms and legs. Vesicles heal
without crusting, which clinically differentiates them from
the vesicles of herpes- and pox-viruses. The rare deaths
are caused by pneumonia.
Hand-foot-and-mouth disease
• Hand-foot-and-mouth
disease: mostly coxackie A
– fever, malaise, sore throat,
vesicles on bucсal mucosa,
tongue, hands, feet,
buttocks
•
highly infectious
•
resolution – 1w
H. Myocardiopathy: Coxsackie virus B infections are
increasingly recognized as a cause of primary myocardial disease
in adults as well as children. Coxsackieviruses of group A and
echoviruses have been implicated to a lesser degree.
In experimental animals, the severity of acute viral
myocardiopathy is greatly increased by vigorous exercise,
hydrocortisone,
alcohol
consumption,
pregnancy,
and
undernutrition and is greater in males than in females. In human
illnesses, these factors may similarly increase the severity of the
disease.
I. Acute Hemorrhagic Conjunctivitis: Coxsackievirus A24 is
one of the agents that can cause this disease (see below).
J. Diabetes Mellitus: Serologic studies suggest an
association of diabetes of abrupt onset with past infection by
Coxsackievirus B4 and perhaps other members of the B
group. Experimental studies support the findings in humans.
Another picornavirus, encephalomyocarditis virus, induces
lesions in mice in the pancreatic islets of Langerhans as well
as an accompanying diabetes.
K. Swine Vesicular Disease: The agent of this disease is an
enterovirus that antigenically is related to Coxsackievirus B5.
Furthermore, the swine virus can also infect humans.
Immunity. In humans, Nt and CF antibodies are
transferred passively from mother to fetus. Adults have
antibodies against more types of coxsackieviruses than
do children, which indicates that multiple experience with
these viruses is common and increases with age.
ECHOVIRUSES
The echoviruses (enteric cytopathogenic human orphan
viruses) are grouped together because they infect the
human enteric tract and because they can be recovered
from humans only by inoculation of certain tissue cultures.
Over 30 serotypes are known, but not all cause human
illness. Aseptic meningitis, febrile illnesses with or without
rash, common colds, and acute hemorrhagic conjunctivitis
are among the diseases caused by echoviruses.
Properties of the Viruses
General
Properties.
Echoviruses
enteroviruses measuring 24-30 nm.
are
typical
Important Characteristics
• Not produce diseases in sucking mice,
rabbits, or monkeys;
• Cause aseptic meningitis, infantile
diarrhea,
• Monkey kidney and human
embryonated kidney cell culture
RHINOVIRUS GROUP
Rhinoviruses are isolated commonly from the nose and
throat but very rarely from feces. These viruses, as well as
coronaviruses and some reo-,
adeno-, entero-,
parainfluenza, and influenza viruses, cause upper
respiratory tract infections, including the "common cold."
General Properties: Rhinoviruses are picornaviruses
similar to enteroviruses but differing from them in having a
CsCI buoyant density of 1.40 g/mL and in being acid-labile.
Animal Susceptibility and Growth of Virus. These viruses
are infectious only for humans and chimpanzees. They have
been grown in cultures of human embryonic lung fibroblasts
(WI-38) and in organ cultures of ferret and human trachea!
epithelium. They are grown best at 33 °C in rolled cultures.
Illness associated with recently identified
enteroviruses
• Enterovirus 68 Pneumonia and bronchiolitis
• Enterovirus 69
Isolated from an ill person in Mexico
• Enterovirus 70
Acute hameorrhagic conjunctivitis
• Enterovirus 70, 71
Paralysis, meningo-encephalitis
• Enterovirus 71 hand-foot-and-mouth disease
• Enterovirus 72
Hepatovirus( Hepatitis A)