class 1-2
advertisement

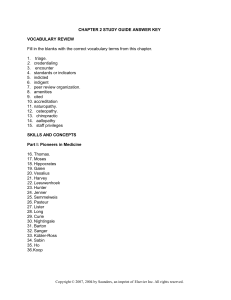
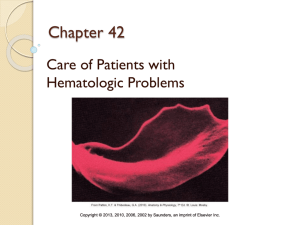
Chapter 1 Child Health Evolution Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. Key Terms • Anticipatory guidance • Critical thinking • Emancipated minor Evidence-based practice • Healthy People 2000: National Health Promotion and Disease Prevention Objectives • HIPAA Holistic • Infant mortality rate Informed consent • Mature minor doctrine Morbidity • Pediatric Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-2 Learning Objectives • Define or identify vocabulary terms listed • List government programs that have affected the care of children • Contrast present-day causes of morbidity and mortality with those of the past • Discuss current health care trends in pediatrics and the effect they have on nursing care Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-3 Pediatrics • The branch of medicine that deals specifically with children, their development, childhood diseases, and the treatment of such diseases • The study of pediatrics began under Abraham Jacobi (1830-1919), a Prussian-born physician – Known today as the father of pediatrics – Paved the way for the promotion of children’s health through the establishment of “milk stations” • Mothers could bring sick children for treatment and learn the importance of pure milk and its proper preparation Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-4 Pediatrics Recent Evolution of Nursing Care • Over the past 100 years, the nursing care of children has evolved into a holistic approach – Children have a physical, intellectual, emotional, and spiritual nature with needs that differ according to their developmental level • Modern medicine has reduced death and disability over the past 100 years – Allows pediatric nurses to focus on improving the scope and quality of their care for each child Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-5 Government Programs • White House Conference on Children and Youth – First one in 1909 – Issued 15 recommendations • E.g.: Children’s Bureau for Child Welfare, est. 1912 • Social Security – Began matching state/federal funds for maternal/child care and child disability in 1935 – Supports preventive health programs; i.e., immunization, screenings Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-6 Government Programs • The Fair Labor Standards Act – Passed in 1938 – Regulates work conditions for children under 18 • Medicaid and the Children and Youth Project – Formed in 1965 – Provides care for children in low-income and inaccessible areas • The Special Supplemental Food Program for Women, Infants, and Children (WIC) – Started in 1966 – Safeguards the health of low-income women and children up to age 5 Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-7 Government Programs • The Child Nutrition Act – Enacted in 1966 – Provides free or reduced-rate meals for lowincome children • The Missing Children’s Act – Passed in 1982 – Established a clearinghouse for efforts and services related to missing children Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-8 Government Programs Safeguarding Uninsured and Underinsured Children • The Children’s Defense Fund – Advocates children’s health care reform • The Balanced Budget Act of 1997 – Established the State Children’s Health Insurance Program (SCHIP) as Title XXI of the Social Security Act • Expands insurance coverage to many uninsured children ineligible for Medicaid • The Patient Protection & Affordable Care Act • The Health Care & Education Reconciliation Act of 2010 – Both address the issue of inadequate health care coverage for children Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-9 Government Programs Health Promotion • Healthy People 2000: National Health Promotion and Disease Prevention Objectives – 1990 – document released by the U.S. Department of Health and Human Services – Presents an opportunity for Americans to take responsibility for their own health – Equal access to health care for all, particularly the most vulnerable (i.e., infants and children) • Healthy People 2010 is a follow-up to Healthy People 2000 • Healthy People 2020 continues to strive for a healthier nation Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-10 Changes in Mortality and Morbidity • Infant Mortality Rate – The number of infant deaths per 1000 live births – Has declined from approximately 200 in 1900 to 20 deaths in 1970 to 6.77 in 2007. – Infant mortality among infants of non-Hispanic black mothers is much higher than nonHispanic whites and Hispanic mothers (Heron, Sutton, Xu, et al., 2010). Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-11 # of infant deaths per 1000 live births U.S. decline in infant mortality rate over the past 100 years 250 200 150 20% 100 50 2% .68% 0 1900 1970 2007 Year Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-12 Changes in Mortality and Morbidity • Childhood morbidity (illness, chronic disease, disability) is affected by – – – – general health socioeconomic status access to health care psychosocial factors • At-risk children who often have more frequent illnesses: – – – – homeless live in poverty attend daycare regularly decreased access to the health care system Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-13 Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-14 Current Practice Education Requirements • Because of the rapid changes taking place in health care today, it is the nurse’s responsibility to update his or her knowledge continually • Nurses have a responsibility to the community and to their profession – Involvement in community and professional organizations is not simply encouraged; it is absolutely essential for continued growth in an ever-changing society Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-15 Current Practice Research and Roles • Evidence-based practice – Through examination of research literature, nurses can analyze important evidence and improve the quality of care for their patients • Anticipatory guidance – Caring for children in today’s society necessitates careful assessment and early identification of children and families at risk Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-16 Current Practice Critical Thinking and the Nursing Process • Critical Thinking – Emphasizes process, inquiry, reasoning, creativity, and ingenuity, so that the nurse can draw the best conclusion regarding a situation – One’s ability to think and find solutions that provide the most effective nursing care • The Nursing Process incorporates five phases – – – – – Assessment Diagnosis Planning Implementation (intervention) Evaluation Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-17 Current Practice Critical Thinking and the Nursing Process • Assessment phase – Also known as the data-gathering phase – The nurse obtains information about the child’s physical, social, and emotional health, as well as the family’s adaptation to health alterations • Diagnostic phase – Lists problems that emerge from the assessment – Diagnoses approved by the North American Nursing Diagnosis Association (NANDA) are listed on the inside back cover of your textbook. Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-18 Current Practice Critical Thinking and the Nursing Process • Planning phase – Nurse uses goal-setting and outcome criteria to construct a plan of care to treat diagnoses • Implementation (intervention) phase – Nurse executes plan of care constructed in the planning phase • Evaluation phase – Nurse appraises the changes experienced by the child or family in relation to achieving goals or outcomes Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-19 Documentation • The nurse must document assessment findings throughout the child’s stay, regardless of setting • Ensures completeness of care • Important legally – Always document time – Each patient’s chart is a legal document – In lawsuits, if something was not charted, it was not done! Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-20 Confidentiality and Informed Consent • Health Insurance Portability & Accountability Act (HIPAA) – Enacted in 1996 – Requires strict observance of confidentiality within the hospital setting • This includes spoken confidentiality and patient records – When working with older children and teens, nurses should explain confidentiality and its limits • Plan to harm oneself or others • Any abuse that may have occurred Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-21 Confidentiality and Informed Consent • Informed consent – Obtained from the parent or legal guardian when written approval is needed to perform a procedure for an underage, not emancipated minor – Nurses are responsible for witnessing the signing of informed consent • Emancipated minor – Adolescent younger than 18 years old, but no longer under parental authority • Mature minor doctrine – Laws designed to afford young people medical care without parental consent – Varies from state to state (NJ has no provision for minor or emancipated minors to consent to routine medical treatment) • [NAEHCY; Faegre & Benson LLP; January 15, 2009; SUBJECT: Unaccompanied Youth and Access to Medical Care] Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 1-22 Health Care Delivery Settings Clinics and Offices • Outpatient facilities and/or community clinics – Run by larger hospital with collaborating group of physicians, or a private physician’s office • Both general and specialty clinics exist – Cardiac, orthopedic, respiratory, etc • Elective surgery in outpatient clinics • Parents/caretakers are taught all of a child’s recovery needs at home for a same-day discharge procedure • Triage – In most offices/clinics, nurses triage (prioritize) and respond to telephone inquiries Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-23 Health Care Delivery Settings Office and Home Care • • • • Pediatric Nurse Practitioner (PNP) – Provide in-clinic patient care, and routine physical exams in collaboration with the physician – Often the primary contact person for children in the health care system Increasingly home care is popular due to technical improvements – Ongoing IV therapy home care – Phototherapy home care for jaundice – Lower cost – Increased patient satisfaction Case Manager – Plays a vital role in home care arrangements by managing complete medical care for the patient – Facilitates linking home care families into a wide variety of network services Hospice – A team of hospice nurses and caregivers assist the families in providing home care for terminally ill children Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-24 Health Care Delivery Settings Other Settings • Support groups – Geared toward family support and learning – Group therapy aids in the prevention of mental health problems for children who have undergone stressful situations • Camps – Many exist in the U.S. for children with chronic illnesses – Camp nurses ensure children receive proper care • Parish nurses – Promote health within the context of a faith community • Long-term care facilities – May be necessary for children with severe mental retardation, multiple disabilities or medical fragility Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-25 The Hospital Setting • Pediatric units differ from adult units – A more cheerful, casual atmosphere in keeping with the child’s emotional and physical needs • Most pediatric departments include a playroom with toys for various age groups run by a child life specialist – Nurses provide age-appropriate toys to children who can’t leave their rooms • A flexible routine is typically maintained in regards to eating, play, and rest • Most hospitals provide beds and encourage parents to stay with their children Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-26 The Child’s Reaction to Hospitalization • Factors – – – – Age Previous illness-related experiences Support of family and health professionals Emotional status MOMMY?!! • Stressors – – – – Separation anxiety Loss of control Bodily injury Pain Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-27 The Child’s Reaction to Hospitalization Infants and Toddlers • Separation anxiety – The major stressor of hospitalization for toddlers – Occurs in the following stages • Grief – Protesting loudly and crying for their mothers until falling asleep from exhaustion • Despair – Depression, lethargy, refusal to eat • Denial – Deny the need for mother by appearing detached and uninterested in her visits – A disguise to prevent further emotional pain Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-28 The Child’s Reaction to Hospitalization Infants and Toddlers • Loss of control • Regression – Toddlers will abandon recently acquired skills and demand assistance with tasks previously mastered – Nurses should remind parents that this is normal behavior when toddlers are hospitalized • Fear of injury – Minimizing fear of injury stressors Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-29 The Child’s Reaction to Hospitalization Infants and Toddlers • Dealing with the stressors of hospitalization – Toddlers achieve control through choices – Forewarn children about any unpleasant or new experience immediately beforehand – Be honest about procedures, etc., that may hurt – Explain procedures step-by-step as they occur – Encourage play with safe equipment; i.e., stethoscopes under supervision – Administer treatments in a room other than the child’s room – Allow toddlers out of the crib whenever possible Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-30 The Child’s Reaction to Hospitalization Preschoolers • Separation anxiety • Uncooperative; frequently ask for parent • Loss of control – Many preschoolers perceive hospitalization as punishment • Regression – E.g.: bedwetting • Fantasy • – – – Pre-logical thinking; fantasy Fear of hospital machinery Nightmares Fear of bodily harm during procedures Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-31 The Child’s Reaction to Hospitalization Preschoolers • Communication between nurse and patient – Use understandable language when describing procedures – Communicate time as a series of events, not hours and minutes – Be aware of verbal and nonverbal cues – Participate in fantasies in a positive way, giving the child control over imagined situations Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-32 The Child’s Reaction to Hospitalization School-Age Children • Separation anxiety • Miss parents but miss friends more • Loss of control – Children in this age group are learning to control their feelings and actions – Independence is limited – They may have changes in vital signs due to stress when hospitalized, even if making efforts to seem calm • Fear of pain, bodily harm, permanent disability, body disfigurement or death Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-33 The Child’s Reaction to Hospitalization School-Age Children • Dealing with the stressors of hospitalization – Bring items from home for familiarity and control – Drawing – Board games with involved adults – Maintain the child’s privacy – Continue education; connect to the outside world – Encourage classmate correspondence; Oh, the cell phones!!! Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-34 The Child’s Reaction to Hospitalization Adolescents • May be hesitant to have visitors – May be embarrassed by appearance – Fear that illness or procedures will change them • Compliance may be a problem with a chronic disease – Probably afraid and stressed, even if they seem calm • Dealing with the stressors of hospitalization – Fear of the unknown; explain everything in an age-appropriate manner – Offer choices to maintain control and independence – Clear limits and expectations so adolescents feel less confused Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-35 The Hospitalized Child The Family’s Reaction to Hospitalization • Parents may initially feel guilty, helpless, and anxious • Developing a trusting relationship with parents is often the key to helping the child • Hospitalization may cause financial problems for the family • The nurse assesses the family’s needs and develops interventions to meet these needs Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-36 The Hospitalized Child The Family’s Reaction to Hospitalization • Nursing Interventions – Assist parents in obtaining written and verbal information concerning the condition of the child and the treatment plan – Orient the family to hospital and explain all procedures – Refer the parents as needed to social services – Listen to parents’ concerns and clarify information – Involve parents in the care of the child – Provide for rooming-in – Reinforce positive parenting – Provide educational resources as necessary Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-37 The Nurse’s Role Admission Process • Provide a tour for the parents and child before admission, if possible to decrease fear of the unknown • Focus on pleasant and positive aspects—but not to the point where hospitalization seems to involve no discomforts • Security objects from home reduce anxiety in an unfamiliar setting • Explain certain procedures, listen to patients and encourage questions • Document admission information; perform a systems review and physical examination of the child • All medications are reconciled upon admission, transfer, and discharge Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-38 The Nurse’s Role Health History • Statistical information (name, address, phone number) • Patient profile (eating and sleeping habits, educational level, developmental level, etc.) • Health history (birth history, illnesses, immunizations, previous hospitalizations, allergies, etc.) • Family history (information concerning the health status of the immediate family) • Lifestyle and life patterns (social, psychological, physical, and cultural environment) • Review of systems Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-39 Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-40 The Nurse’s Role Systems Review • When examining the child, generally proceed in a head-to-toe manner while collecting vital signs • Note the facial expression and the general appearance of the child • Always talk to the parents about how they think their child is doing, because they know their child best • Be sure to document and report any unusual or abnormal findings Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-41 The Nurse’s Role Systems Review • Pulse – The pulse rate varies considerably in different children of the same age and size – Apical pulse is preferred for infants and small children • The apical rate /respiratory rates of the newborn infant are high and gradually decrease with age until adult values are reached • Respirations – Observe the movement of the abdominal wall as respirations are mostly abdominal at this time – After about age 7 years, measure respirations the same way as the adult’s – Lungs should be clear to auscultation with no adventitious or abnormal breath sounds Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-42 Blood Pressure • Ensure the blood pressure cuff’s bladder length is 80-100% circumference of the arm and the width is 40% of the circumference of the arm Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-43 The Nurse’s Role Cultural and Religious Preferences • Cultural beliefs affect how a family perceives health and illness • Some practices raise concerns of abuse – E.g.: Coining; cupping • Educate families that strict disciplinary practices may place them in jeopardy with child protective services • Respect any rites, dietary restrictions, etc., associated with a family’s religion, as long as it does not interfere with the child’s well-being Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-44 The Nurse’s Role Discharge Planning • Preparation for discharge begins on admission • Directions for home treatment should be given to parents gradually throughout their child’s hospitalization • Documentation includes time of departure, person with whom the child departs, patient’s behavior, instructions/medications given to the patient or parents, and weight/vital signs upon discharge Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-45 The Nurse’s Role Discharge Planning • Prepare parents for potential post-hospitalization behavior problems – Clinging, regression in bowel and bladder control, aggression, fears, nightmares, negativism – Return former family responsibilities within the limits of the child’s present abilities as soon as possible – Avoid making the child a center of attention because of illness. Praise accomplishments unrelated to illness – Be kind, firm, and consistent if the child misbehaves – Be truthful to maintain trust – Provide suitable play materials: Clay, paints, doctor/nurse kits. Allow free play – Listen to the child, clear up misconceptions about the illness – Don’t leave child alone for a long period or overnight until a sense of security is regained Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-46 Safety Transporting, Positioning, and Restraining the Child • Means of transportation varies with a child’s age • Ensure that a patient’s identification band is secure before leaving the unit • Holding a baby – Head and back support is necessary for young infants – Random movements of small children necessitate secure holding • Restraints should rarely be used – Detailed documentation is required – Restraints must be removed at least every 2 hours to avoid impairing circulation and assess skin status • Therapeutic holding – Holding a child in a secure, comfortable manner Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-47 Safety Transporting, Positioning, and Restraining the Child Do • Lock wheelchairs and stretchers before placing patients in them • Use safety straps with children when sitting • Apply restraints correctly to prevent constriction of a part. Check institutional policy on frequency of releasing restraints and providing range of motion • Handle infants and small children carefully. Use elevators rather than stairs. Walk at the child’s pace • Place a hand on the infant or child’s back or abdomen when you turn your back to the child • Always look for small objects which can become choking hazards Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-48 Safety Transporting, Positioning, and Restraining the Child Do • Protect children from entering the treatment room, elevator, utility rooms, and stairwells • Keep crib sides up at all times when unattended in bed. Use enclosed (bubble top) cribs for older infants and toddlers to keep them from falling or climbing out of the crib • Turn an infant perpendicular to the side of the bed when rails are down. Ensure that the infant will not roll off when rails are down • Place cribs so that children cannot reach electrical outlets and appliances • Check hospital policy for children who are alone (for instance, policy may recommend that the door be kept open) Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-49 Safety Transporting, Positioning, and Restraining the Child Don’t • Don’t force-feed children. There is a danger of choking, which may cause lung disease or sudden death • Don’t allow patients to use wheelchairs or stretchers as toys • Don’t leave a child unattended in a highchair, infant seat (if it is placed on any area above the floor), swing or stroller or in a bath tub • Don’t leave a child unattended on an examination table – Always keep your hand on the child • Don’t leave small children unattended out of their cribs in their rooms • Do not tie balloons to the crib rails Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-50 Safety Medical Asepsis • Contaminated – A person/object that has come into contact with an infected patient • Disinfected – Killing microorganisms physically or chemically Do • Wash your hands before and after caring for each patient • Properly disinfect any item brought out of an isolation room • Do wear a gown if holding a patient; change between patients Don’t – Don’t cause cross-infection • Diapers, toys, and materials that belong in one patient’s storage unit should not be borrowed for another patient’s use Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-51 Safety General Safety Guidelines Do • Inspect toys for sharp edges and removable parts • Identify the patient properly before giving medications • Keep medications, solutions lotions, tissues, disposable pads and diapers, and safety pins out of infant’s reach • Keep the medication room locked when not in use • Locate fire exits and extinguishers on the unit and learn how to use them properly. Become familiar with the facility's fire manual • Supervise playroom activity • Take proper precautions when oxygen is in use • Use electrical outlet safety plugs on the unit • Continually assess the patient setting for safety issues Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-52 Safety General Safety Guidelines Don’t • Don’t leave medications at the bedside • Don’t leave any medication administration materials in the child’s bed or infant’s crib • Be aware of wear you place the caps from the pediatric oral syringes. Do not leave in the bed! Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-53 Implications of Pediatric Surgery Patient Preparation • The nurse should give simple information about the system that will be affected – Stress that this is the only area of the body that will be involved • Children need to know what to expect on the day of surgery; use a doll to demonstrate • Children are particularly fearful of surgery and need both physical and psychological preparation • The child should be able to easily understand explanations and information given in simple terms • It is important to always be truthful; this establishes trust Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-54 The Child in Pain Definition and Challenges • Children of all ages experience pain and are entitled to appropriate pain management • Pain is an individual, subjective experience, and health care providers need to identify and treat pain adequately • Always ask the child and/or the parents about past pain experiences and known coping mechanisms Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-55 The Child in Pain Evaluation • When evaluating the child, include precipitating factors, location, onset, duration, quality, intensity, and characteristics of the pain • Pain scales – 1 to 10 Pain Rating Scale – FLACC • Infants and young children – Oucher Scale • 2- to 7-year-olds – Wong-Baker FACES Pain Rating Scale • Preschool and young school-age Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-56 FLACC pain scale Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-57 The Child in Pain Intervention • Oral administration is generally used for mild to moderate pain • When the child needs immediate pain relief for more intense pain, intravenous administration is indicated • For moderate to severe pain that is expected to persist, continuous dosing or around-the-clock dosing at fixed intervals is recommended • Pain medication may also be administered rectally, by intramuscular (IM) injection, transdermally, or topically (EMLA, LMX) • Nonopioid analgesics are most effective for mild to moderate pain and have antipyretic effects as well • Opioids are used to manage most forms of moderate to severe acute and chronic pain Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-58 The Child in Pain Intervention • Nonpharmacologic interventions – Used in conjunction with pharmacologic interventions or by themselves – Complementary or alternative medicine (CAM) • Hypnosis • • • • – Altered state of consciousness. Suggestions can lead to changes in behavior or physical sensations TENS unit Acupuncture Chiropractors Massage therapy Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 2-59