Correlation Between Biochemical and Anthropometric
advertisement

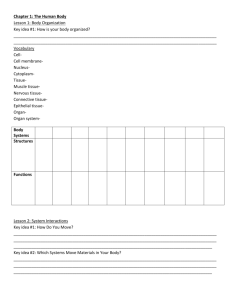
Correlation between anthropometric measures and biochemical cardiovascular risk markers in hypertensive elderly Correlación entre parámetros antropométricos y marcadores bioquímicos de riesgo cardiovascular en ancianos hipertensos Asdrúbal Nóbrega Montenegro-Neto, Mônica Oliveira da Silva-Simões, Ana C. Dantas de Medeiros1, Alyne da Silva Portela1, Maria do Socorro Ramos de Queiroz1, Ramon Cunha-Montenegro2 and Maria Irany-Knackfuss3 1 Universidade Estadual da Paraíba–UEPB. Brasil. netotraducao@hotmail.com, moscg@uol.com.br, anacdmedeiros@yahoo.com.br, alyneportela@yahoo.com.br, queirozsocorroramos@yahoo.com.br, 2 Centro Universitário de João Pessoa–UNJPÊ. Brasil. proframon@ig.com.br 3 Universidade Federal do Rio Grande do Norte-UFRN. Brasil. mik@ufrnet.br Recibido 28 Diciembre 2010/Enviado para Modificación 20 Mayo 2011/ RESUMEN Objetivos El objetivo de este estudio fue correlacionar indicadores antropométricos de riesgo cardiovascular adicionales en una población de ancianos hipertensos registrados en el programa HIPERDIA, en Campiña Grande, Paraíba, Brasil, América del Sur. Métodos La muestra contó con 131 ancianos hipertensos, de 60 a 92 años (25,9 % masculino y 74,1 % femenino). Se utilizaron antropometría y encuesta por medio de un cuestionario con informaciones socioeconómicas, demográficas, hábitos de vida, y frecuencia de las enfermedades. En el análisis fue utilizada la correlación de Pearson, estadística descriptiva y para la comparación de las variables antropométricas por sexo Test t de Student y ANOVA One-Way para comparación por edad: 60 a 69, 70 a 79 y ≥ 80. Resultados Los hombres presentaron frecuencias de 14,7 % de sobrepeso y 11,8 % de obesidad, y mujeres 24,7 % y 21,6 %, respectivamente. En el análisis de índice cintura-cadera, 57,0 % de las mujeres y 26,5 % de los hombres presentaron valores de riesgo. Analizando el perímetro de la cintura, 95,9 % de las mujeres y 52,9 % de los hombres presentaron riesgo, y 95,9 % de las mujeres y 38,2 % de los hombres presentaron elevados valores del perímetro abdominal. Despúes de una selección (n=40) para la corrección de posibles factores de confusión, 27 personas presentaron Proteína C Reactiva elevada. Conclusiones Los resultados muestran riesgo cardiovascular adicional, que se demonstra por la alta frecuencia del sobrepeso y obesidad central que se presentan en la población, asociados a inflamación subclínica en hipertensos. Palabras Clave: Antropometría, presión sanguínea, estado nutricional (Fuente: DeCS, BIREME). ABSTRACT Objectives The objective of this study was to correlate anthropometric markers that indicate additional cardiovascular risk in a hypertensive elderly population enrolled in the HIPERDIA program, in Campina Grande, Paraíba, Brazil, South America. Methods The sample was composed of 131 hypertensive elderlies from 60 to 92 years (25,9 % males and 74,1 % females). In the assessment a socioeconomic, demographic, life style questionnaire was used. Information about anthropometry measures and frequency of pathologies were also registered in this questionnaire. In the analysis we used Pearson´s correlation, descriptive statistics, comparison between anthropometric variables by sex using t Student test and ANOVA One-way were used to compare groups by age, form 60 to 69, 70 to 79, and ≥ 80 years. Results Men presented frequencies of 14,7 % of overweight and 11,8 % of obesity, and women presented 24,7 % and 21,6 %, respectively. In the waist-to-rip ratio analysis, 57,0 % of women and 26,5 % of men had presented inadequate values. In the waistline measure, 95,9 % of women and 52,9% of men presented high risk, and 95,9 % of women and 38,2 % of men showed high values in abdominal circumference. After selection (n=40) for correction of potential confounders, it was found that 27 subjects had elevated C-Reactive Protein values, a additional cardiovascular risk factor. Conclusions Results pointed to additional cardiovascular risk that could be demonstrated by the high prevalence of overweight and central obesity presented by the population and the presence of subclinical inflammation between hypertensive ones. Key Words: Anthropometry, hypertension, nutritional status (source: MeSH, NLM). According to the World Health Organization-WHO in a report published in 2003, the world is about 600 million hypertensive patients (1-3). In Brazil, estimates made by the Ministério da Saúde show that the prevalence of hypertension is already high, reaching about 22,3 % to 43,9 % of the population over the age of twenty in some cities (4). Studies have shown that the risk assessment of cardiovascular health, usually performed by determining the Framingham scores, can be improved by measuring plasma markers of inflammation and anthropometric evaluation (5-7). These markers include acute phase proteins like C-Reactive ProteinCRP (6-7). Anthropometry is an effective method of nutritional status assessment (8,9). Its variables have been reported in the literature as important predictors of cardiovascular risk (10,11). HiperDia is a program created by the Ministério da Saúde of Brazil that enrolls hypertension and diabetes patients in all ambulatory clinics of the Sistema Único de Saúde-SUS. Based on this context, this study aimed to correlate biochemical markers (total cholesterol and CRP) with anthropometric measures, indicators of additional cardiovascular risk in a population of elderly hypertensive patients. MATERIAL AND METHODS This was a population-based quantitative study with non-probability intentional sample. The population consisted of 100,0 % of hypertensives (n= 4 108) aged over 60 years, enrolled in HiperDia in Campina Grande, Paraíba, Brazil, from February 2007 to December 2008. The sample consisted 131 elderlies aged over 60 years (n=131) enrolled in HiperDia registered in the major Health Unity of SUS in Campina Grande. Data collection was performed from February 2007 to December 2008, on Monday and Tuesday mornings from 8 to 11 hours, and on Tuesday afternoons from 13 to 16 hours, a period corresponding to the service operation being realized in three stages: The first consisted of research with participants, with form-filling, to obtain socio-economic data, lifestyle and prevalence of diseases, evaluation of blood pressure and anthropometric measurements. Were considered physically active regular participants who performed any kind of physical activity, with regular attendance (at least 3 times a week) in a minimum of 30 minutes daily. Participants who did not practice any form of physical activity with regular frequency were considered sedentary (12). Income was defined as the sum of all family income divided by the number of residents. The education level was defined as the number of study years at regular schools. The information about lifestyle contained the use or not of tobacco and alcohol together with their frequency in years. In the second phase was carried out blood collection for determination of lipids and glucose, which was sent to the Laboratory of Clinical Analysis of UEPB in the same period. Blood pressure was measured twice on the right arm of each patient in the sitting position after at least five minutes rest, whereas the hypertensive subject who had a mean systolic blood pressure–MSBP>140 and Mean diastolic blood pressure–MDBP>90 mmHg(2). For this, it was used a calibrated aneroid sphygmomanometer device, Mark Wan Med®, as well as a stethoscope, the Littmann ® brand. Anthropometric assessment was performed with the subjects without shoes and coats, wearing only light clothing, upright, with feet together. Techniques proposed by De Groot (13) and Lohman (14). The following indicators were evaluated: a. Body Mass Index-BMI, with the cutoff values proposed by the Pan American Health Organization-PAHO, used in the research Health Welfare and Aging HWA: Low weight<23 kg/ m², normal weight 23–27,99 kilograms/m², Overweight 28 to 29,99 kg/m² and obesity≥30 kg/m² (15); b. To obtain measurements were used: electronic digital scale Tanita ® (Model VM-080), with a capacity of 150 kg, varying from 100 g; tapemeasure type inextensible Sanny ®, and stadiometer SEA ® - 206, with capacity for 220 cm; c. Waist-Hip Ratio-WHR, being considered as having central obesity female subjects who had WHR>0.85 and males who had WHR>1.0 (13,14); d. Abdominal Circumference–AC, were considered at risk for metabolic and cardiovascular diseases, males who had the measure not less than 102 cm and female individuals that presented less than 88 cm (13,14). e. Waist circumference-WC, considering as reference indicate risk values for men ≥ 94 cm and for women ≥ 80 cm (13,14). The lipid profile was analyzed in accordance with the IV Brazilian Guidelines on Dyslipidemia of the Brazilian Society of Cardiology–BSC (16), with the collection of blood taken after 12 hours fasting minimum, calculated by the Friedewald method (16). Was considered diabetic individuals who had fasting plasma glucose>126 mg/dl on two occasions. The method used for determination of blood glucose after at least 12 hours fasting minimum was the enzyme colorimetric (17). The third phase consisted of collecting blood for serum high-sensitivity C Reactive Protein–hs-CRP. Which was preceded by pre-selection of individuals, being invited to take the examination who had only hypertension. Blood samples were sent for analysis to Hermes Pardini Institute, Belo Horizonte, Minas Gerais, Brazil, in the same period. The analysis method used was the nephelometry, whereas increased cardiovascular risk in subjects who had values of hs-CRP above the 3rd quintile (1,2–1,9 mg/dL) distribution according to BSC (16). Statistical analysis description The analysis was realized in 2 steps, using the Kolmogorov-Smirnov test, regarded as a significant (p <0.05). In the first step, comparison of anthropometric variables, it was formed two groups, one male and one female. The mean BMI, AC and WHR were compared by sex using the Student t test. Subsequently, to investigate the influence of age on anthropometric variables, it was formed three groups of participants to comparison according to age: Group 1 (60 to 69 years), Group 2 (70 to 79 years) and Group 3 ( ≥ 80 years). Then, it was performed using ANOVA One-Way. In the second stage, in order to identify a correlation between the anthropometric and biochemical variables, it was used the Pearson Correlation Test (r). Following recommendations of Ford´s (6) study, to minimize the influence of confounding factors in the value of hs-CRP, were selected elderly patients who, only, arterial hypertension. Those who were classified as overweight or obesity, diabetes, arthritis, and any inflammatory and/or infection in the previous two weeks for blood tests did not dosage hs-CRP. The results were considered as statistically significant were those who had p <0.05. RESULTS At the age stratification by sex, population (n=4 108, 1 399 men and 2 709 women) showed: for male (n= 672) aged 60-69, (n=488) of 70-79 years and (n=239) more than 80 years and for females (n=1 408) aged 60-69, (n=887) 70-79 years and (n=414) of 80 or more years old, data found on the system HiperDia (17). In this sample, 25,9 % of the participants were male and 74,1 % female (n=131). The age ranged from 60 to 92 years, with an average of 71 years. The monthly family income of the group in the study ranged from 32,05 to 800,00 $ Reais per person, with an average of 268,85 $ Reais. About the type of disease, 73.5 % are hypertensive, 26.5 % are diabetic and hypertensive, and none of them is exclusively diabetic. Knowing that the whole population is under pharmacological treatment for hypertension: the mean systolic blood pressure for men was 123,3 mmHg and 133,4 mmHg for women. Mean diastolic pressure for men was 76,7 mmHg and for women 80,2 mmHg. Concerning to living habits, 94,7 % of respondents stated that they did not smoke, being considered nonsmokers individuals who reported having stopped smoking for at least one year, 98,5 % did not use alcohol for over a year and 75,8 % of the elderly did not exercise regularly. In both gender, there was a high prevalence of obesity and overweight. Since 14,5 % of the aged are underweight, 44,3 % were normal weight, 22,1 % were overweight and 19,1 % are obese. The prevalence of underweight were 20,6 % in males and 12,4 % in females. Among men, overweight was 14,7 % and obesity 11,8%, as women these values were higher, respectively 24,7 % and 21,6 % (Table 1). In the comparison of averages by gender, it was used the Student t test. It was found a BMI average equal to 25,8 (SD: 3.3) for males and 27,5 for females (SD: 3.6), statistically significant differences between genders (p=0,0143). For the WC in men, it was obtained an average of 96 cm (SD: 10.9) and women an average of 94.7 (SD=9.9), no statistically significant differences between genders (p=0, 5206). According to WC, Figure 1 shows among women, 95,9 % showed increased cardiovascular risk. The percentage of men at high risk was lower, corresponding to 52,9 %. Regarding AC, Figure 1 shows that 95,9 % of women had risk indicative values, in men the percentage was 38,2 %. Since, compared by gender, the AC average of men was 99,4 cm (SD: 10.9) and women of 102.4 cm (SD: 9.7), indicating no statistically significant difference between sexes (p=0,1258). In the analysis of WHR was observed that 57,0 % of women and 26,5 % of men had values equal to or above the recommended (Figure 1). The overall average WHR for men was 0,94 (SD=0,06) and for women of 0,90 (SD=0,07), indicating the existence of differences between the genders. In the analysis of variance, the elderly were divided into 3 groups by age, 60 to 69 (n=59), 70 to 79 (n=58) and ≥80 (n=14) years. WHR showed a statistically significant difference seen regarded to age, group 1 compared to the others, which can be viewed in Table 2 (p= 0,0418), but BMI, AC and WC showed no significant difference (p<0,05). After the anthropometric data collection all subjects were asked to perform a blood test for lipids profile determination, however, it was only assessed in 83 participants. These data are presented as averages in Table 3. Based on BSC (4), lipids and 12 to 14 hours fasting plasma glucose, individuals aged ≥ 20 years, it was verified the suitability of the average values obtained in this study (Table 4). Hs-CRP was evaluated in 41 subjects, 11 males and 30 females, who were selected following the criteria established in the methodology of this study to eliminate confounding factors (Table 5). It was verified statistically significant difference of hs-CRP regarding to gender, with an average of 1,9 for males and 3,2 for females (p=0,03). Twenty-seven subjects had values above the 3rd quintile of the population distribution, and 18 above the 4th quintile and 9 above the 5th quintile. Finally, it was performed the Pearson correlation test between hs-CRP, lipid profile and anthropometry of hypertensive individuals, selected for exclusion of confounding factors mentioned in the methodology of this study (n=41). It was found that BMI and the WC and AC average were strongly associated positively (r=0,7, p <0,001): the higher the BMI greater the WC. The BMI also showed a positive correlation, even stronger, with the Hip circumference average–HC (r=0,8, p<0,001). The results obtained with the correlation test, with a value of Pearson's r ranged from 0,00 to 0,19, which indicates association classified as poor between hs-CRP and lipid profile and anthropometric evaluated in this study. DISCUSSION In the period of this research, Campina Grande, the second most populous city in Paraíba, there were 6 682 hypertensive patients enrolled in the program (17). The multiplicity and interaction between various cardiovascular risk factors may be involved in the development and progression of many diseases (18,19). Despite low prevalence of smoking and alcohol, both (5,3 %), this sample has high rates of physical inactivity (75,8 %). According to Siqueira (20), the latter is above the average in the northeast region of Brazil (58,0 %). No significant difference regarding the prevalence of obesity in the age groups 60 to 69, 70 to 79 and ≥80 years. However, as the study of Abrantes (21) it was observed that the prevalence of obesity is significantly higher among females (2,6 %), reaching almost twice the value of males (11,8 %). In WC analysis, it was found that gender and not age has a significant influence on this variable. Women are the majority in this study (74,1 %), and (95,9 %) showed measures indicative of increased cardiovascular risk, compared with a frequency (52,9 %) among men, which contradicts the literature, which states that central obesity is more common among men (22). It is emphasized that fat distribution pattern could be associated with a long and healthy life presented by men is this sample. Only WHR showed a statistically significant difference regarding age (p=0,0418), and respected to gender (p=0,0046). Of the women studied 90,6 % had AC≥the recommended amount, and 26,7 % of men were with high values. The pattern of body fat distribution has great importance, because the accumulation of abdominal fat has close relationship with metabolic and cardiovascular diseases such as diabetes mellitus and hypertension, respectively (23). In the lipid profile test, the population, generally, did not present high risk, with averages considered advisable by BSC (16). However, as already discussed, the anthropometric average had a high frequency of inadequacy, with values above those recommended in the literature, which indicates the additional cardiovascular risk promoted by hypertension in the studied population (14,21-23). The correlations between hs-CRP and lipid profile performed after rigid control of confounding variables (6) were considered weak. Knowing that CRP is an independent risk factor for cardiovascular disease, it was emphasized, as in Ford (6) and Mendall (24), the importance of hs-CRP and anthropometry (25) in improving cardiovascular risk stratification. Regarding the correlation of CRP with anthropometric variables, these were also regarded as weak, but because they are poorly studied, had no data in the literature for comparison for this age group. Considering hs-CRP as an independent cardiovascular risk factor, and the strict control applied in the selection of a homogeneous sample, this sample presents additional risk for future cardiovascular events(6). The average of years of study among the participants was 3. This low education level, as well Cavalini (26) affirms, may influence the treatment of hypertension in the elderly, since it hinders the understanding of drug prescription and treatment compliance. The low average monthly income of only 268,85 $ Reais per person may influence the treatment in a negative way (26). The high prevalence of overweight and central obesity, high rate of subclinical inflammation represent additional cardiovascular risk for individuals already affected by hypertension. Even with lipid profile values considered normal and anthropometric measurements, some individuals were at increased cardiovascular risk, which could be demonstrated by measuring levels of hs-CRP. We hypothesize that a full assessment of cardiovascular risk in an hypertensive elderly population must include lipid profile, anthropometry and CRP in order to improve cardiovascular risk stratification. REFERENCES 1. Wong LLR, Carvalho JA. The rapid process of aging in Brazil: serious challenges for public policies. R. Bras. Est. Pop. 2006; 23(1):5-26. 2. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003; 42(6): 1206-52. 3. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. (2005) Lancet; 365(9455), pp. 217-23. 4. V Diretrizes Brasileiras de Hipertensão Arterial. Arq Bras Cardiol. 2007; 89(3): e24-e79. 5. Rosini N, Machado MJ, Xavier HT. Study of the prevalence and multiplicity of cardiovascular risk factors in hypertensive individuals from the city of Brusque, SC, Brazil. Arq Bras Cardiol. 2006; 86(3):219-222. 6. Ford ES. Does exercise reduce inflammation? physical activity and C-Reactive Protein among U.S. adults. Epidemiology. 2002; 13(5): 561-568. 7. Fabijanic D, Banic M, Kardum D. C-reactive protein in cardiovascular risk evaluation. Lijec Vjesn 2006; 128(5-6):167-74. 8. Litwin SE. Which Measures of Obesity Best Predict Cardiovascular Risk? J Am Coll Cardiol 2008; 52(8): 616-619. 9. Koh-banerjee P, Wang Y, Hu FB, Spiegelman D, Willett WC, Rimm EB. Changes in Body Weight and Body Fat Distribution as Risk Factors for Clinical Diabetes in US Men. Am J Epidemiol. 2004; 159:1150-1159. 10. De Onis M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr 1996; 64:650-8. 11. Barbosa AR, Souza JMP, Lebrão ML, Laurenti R, Marucci MFN. Anthropometry of elderly residents in the city of São Paulo, Brazil. Cad Saúde Pública. 2005; 21(6):1929-1938. 12. Bomam K, Olofsson M, Dahlõf B, Gerdts E, Nieminen MS, Papademetriou V et al. Left ventricular structure and function in sedentary and physically active subjects with left ventricular hypertrophy (the Life Study). Am J Cardiol 2005; 95:280-3. 13. De Groot LC, Sette S, Zajkas G, Carbajal A, Amorim JA. Euronut SENECA investigators. Nutritional status: anthropometry. Eur J Clin Nutr. 1991; 45(45s3):31-42. 14. Callaway CW, Chumlea WC, Bouchard C, Himes JH, Lohman TG, Martin AD, et al. “Circunferences”. In: Lohman TG, Roche AF, Martorel R (Editors). Anthropometric standardization reference manual. Champaign: Human Kinetics Books ed.; 1988. pp 39-54. 15. Lebrão ML, Laurenti R. Health, well-being and aging: the SABE study in São Paulo, Brazil. Rev Bras Epidemiol. 2005; 8(2):127-141. 16. IV Brazilian Guidelines in Arterial Hypertension. Arq Bras Cardiol 2007; 88(S1):2-18. 17. Departamento de Informática do SUS [Internet]. Sistema de Gestão Clínica de Hipertensão Arterial e Diabetes Mellitus da Atenção Básica. Disponible en: http://hiperdia.datasus.gov.br/. Consultado Agosto del 2010. 18. The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care. 2003: 26(11):3160-7. 19. Polanczyk CA. Cardiovascular Risk Factors in Brazil: The Next 50 Years! Arq. Bras Cardiol. 2005; 84(3):199-201. 20. Siqueira FV, Facchini LA, Piccini RX, Tomasi E, Thumé E, Silveira DS, et al. Physical activity in young adults and the elderly in areas covered by primary health care units in municipalities in the South and Northeast of Brazil. Cad Saúde Pública. 2008; 24(1):39-54. 21. Abrantes MM, Lamounier JA, Colosimo EA. Overweight and obesity prevalence in Northeast and Southeast Regions of Brazil. Rev Assoc Méd Bras 2003:49:2. 22. Lakka HM, Lakka TA, Tuomilehto J. Abdominal obesity is associated with increased risk of acute coronary events in men. Eur Heart. J 2002; 23:706-13. 23. Navarro AM, Stedille MS, Unamuno MRDL, Marchini JS. Body fat distribution in patients with and without chronic-degenerative diseases: use of the waist to hip relationship and arm fat index. Rev Nutr. 2001; 14(1):37-41. 24. Mendall MA, Patel P, Ballam L, Strachan D, Northfield TC. C Reactive protein and its relation to cardiovascular risk factors: a population based cross sectional study. BMJ 1996; 312:1061-1065. 25. Montenegro Neto AN, Simões MOS, Medeiros ACD, Protela AS, Dantas PMS, Knackfuss MI. Altered nutritional status and its association with lipid profile and lifestyle in hypertensive elders. Arch Latinoamer Nutr. 2008; 58:350-356. 26. Cavalini LT, Chor D. A survey on hypertension and cognitive deficit in elderly subjects in a geriatric unit. Rev Bras Epidemiol. 2003; 6(1):7-17. Table 1. Percentual distribution of underweight, normal weight, overweight, obesity prevalence, by gender Gender N General Male Female 131 34 97 Under weight 14,5 20,6 12,4 Normal weight 44,3 52,9 41,2 BMI(%) Over weight 22,1 14,7 24,7 Obesity TOTAL 19,1 11,8 21,6 100 100 100 Table 2. Analysis of variance of The Waist-Hip Ratio related to age Groups Group 1 Group 2 Group 3 n 59 58 14 WHR averagE 0,90 0,93 0,93 Deviation 0,069 0,069 0,062 Table 3. Averages of lipid profile by gender Men (n=25) 74,3 26,2 119,1 42,4 186,0 128,9 102,8 Variable Age (Years) HDL (mg/dL) LDL (mg/dL) VLDL (mg/dL) Total Cholesterol(mg/dL) TriglycerideS (mg/dL) Fasting Glucose (mg/dL) Women (n=58) 69,1 36,3 129,8 40,9 200,0 159,8 110,0 Total (n=83) 70,7 33,3 126,5 41,4 196,5 150,5 107,8 Table 4. Average values adequacy of lipid and glucose profile Test HDL N 54 4 2 33 11 10 9 43 40 53 19 14 47 17 19 47 14 22 LDL VLDL Total Cholesterol Triglycerides 12 to 14 hours fasting Glucose Average < 40 mg/dL > 60 mg/dL <100 mg/dL 100-129 mg/dL 130-159 mg/dL 160-189 mg/dL ≥190 mg/dL 6-40 mg/dL > 40 mg/dL <200 mg/dL 200-239 mg/dL ≥240 mg/dL <150 mg/dL 150-200 mg/dL 201-499 mg/dL < 100 mg/dL 100-125 mg/dL ≥ 126 mg/dL Classification Low High Optimum Desirable Limitrophe High Very High Normal High Level Optimum Limitrophe High Optimum Limitrophe High Normal Pre-diabetics Diabetics Table 5. CRP-us distribution in percentiles by gender CRP Quintil 1 2 3 4 Gender Male Female 3 0 1 2 2 6 4 14 Total 3 3 8 18 5 1 11 Total 8 30 9 41 Figure 1. Distribution (%) of cardiovascular risk related to anthropometric variables, according to gender 100% 75% 95,9 95,9 57,0 52,9 38,2 50% 26,5 25% 0% WC AC WHR Men Women WC=Waist Circumference; AC=Abdominal Circumference; WHR=Waist-Hip Ratio AUTORES ASDRÚBAL NÓBREGA MONTENEGRO-NETO. Fisioterapêuta. Ph. D. en Ciencias de la Salud. Universidade Estadual da Paraíba-UEPB. Campina Grande. Brasil. E-mail: netotraducao@hotmail.com MÔNICA OLIVEIRA DA SILVA SIMÕES. Farmacêutica. Ph. D. en Productos Naturales y Sintéticos. Universidade Estadual da Paraíba-UEPB. Campina Grande. Brasil. E-mail: moscg@uol.com.br ANA CLAUDIA DANTAS DE MEDEIROS. Farmacêutica. Ph. D. en Productos Naturales y Sintéticos. Universidade Estadual da Paraíba-UEPB. Campina Grande, Brasil. E-mail: anacdmedeiros@yahoo.com.br ALYNE DA SILVA-PORTELAFarmacêutica. Posgrado en Desenvolvimiento y Innovación Tecnológica de Medicamentos, Mestre en Salud Coletiva.. Universidade Estadual da Paraíba-UEPB. Campina Grande, Brasil. E-mail: alyneportela@yahoo.com.br MARIA DO SOCORRO RAMOS DE QUEIROZ. Farmacêutica. Mestre en Productos Naturales y Sintéticos. Universidade Estadual da Paraíba-UEPB. Campina Grande, Brasil. E-mail: queirozsocorroramos@yahoo.com.br RAMON CUNHA-MONTENEGRO. Educador Físico. Posgrado en Educación Física. Centro Universitário de João Pessoa–UNJPÊ. João Pessoa, Brasil. E-mail: proframon@ig.com.br MARIA IRANY-KNACKFUSS. Educador Físico. Posgrado em Ciencias de la Salud. Universidade Federal do Rio Grande do Norte-UFRN. Natal, Brasil. E-mail: mik@ufrnet.br