Ch5-Genetics
advertisement

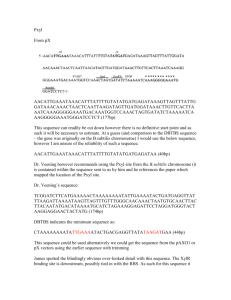
•GENETIC DISORDERS • • • • • • Marfan syndrome Ehlers-Danlos syndrome Familial hypercholesterolemia. Alkaptonuria Turnes syndrome Neurofibromatosis DISEASES •GENETIC •ENVIRONMENTAL •BOTH MUTATIONS • PERMANENT change in DNA GENOME MUTATION: (whole chromosome) –CHROMOSOME MUTATION: (visible chromosome change) –GENE MUTATION: (may, and often, result in a single base error) GENE MUTATION • DELETION OF A SINGLE BASE • SUBSTITUTION OF A SINGLE BASE POINT MUTATION GENE MUTATION • POINT MUTATION within a coding sequence: VAL-GLU • MUTATIONS in NON-coding sequences defective transcription, regulation • DELETIONS/INSERTIONS frameshift mutation, involvement is NOT a multiple of 3 • Tri-nucleotide REPEATS, e.g., CGG repeats many times in fragile X syndrome GENE MUTATIONS • • • • • INTERFERE with protein synthesis SUPPRESS transcription, DNARNA PRODUCE abnormal mRNA DEFECTS carried over into TRANSLATION ABNORMAL proteins WITHOUT impairing syntheses GENETIC DISORDERS • SINGLE gene mutations, following classical MENDELIAN inheritance patterns the most • MULTIFACTORIAL inheritance • CHROMOSOMAL disorders DISORDERS WITH MULTIFACTORIAL INHERITANCE • Multifactorial (polygenic) • A multifactorial physiologic or pathologic trait may be defined as one governed by the additive effect of two or more genes of small effect, conditioned by environmental, nongenetic influences. • The risk of expressing a multifactorial disorder is conditioned by the number of mutant genes inherited. • The risk is greater in siblings of patients having severe expressions of the disorder • • • • • • • Diabetes mellitus, Hypertension, Gout, Schizophrenia, Bipolar disorder, Congenital heart disease, Some skeletal abnormalities. Hypertension provides an excellent example of multifactorial inheritance • An excellent example of multi factorial inheritance is • Hypertension MENDELIAN inheritance patterns • AUTOSOMAL DOMINANT • AUTOSOMAL RECESSIVE • SEX-LINKED (recessive), involving “X” chromosome AUTOSOMAL DOMINANT • Disease is in HETEROZYGOTES • NEITHER parent may have the disease (NEW mut.) • REDUCED PENETRANCE (env?, other genes?) • VARIABLE EXPRESSIVITY (env?, other genes?) • May have a DELAYED ONSET • Usually result in a REDUCED PRODUCTION or INACTIVE protein AUTOSOMAL DOMINANT • • • • • • • • • • • CNS HUNTINGTON DISEASE NEUROFIBROMATOSIS MYOTONIC DYSTROPHY TUBEROUS SCLEROSIS Renal GIT-----Familial polyposis POLYCYSTIC KIDNEY Hematopoietic HEREDITARY SPHEROCYTOSIS VON WILLEBRAND DISEASE Skeletal • • • • • • • MARFAN SYNDROME EHLERS-DANLOS SYNDROMES(some) OSTEOGENESIS IMPERFECTA ACHONDROPLASIA Metabolic FAMILIAL HYPERCHOLESTEROLEMIA ACUTE INTERMITTENT PORPHYRIA AUTOSOMAL DOMINANT PEDIGREE 1) BOTH SEXES INVOLVED 2) GENERATIONS NOT SKIPPED AUTOSOMAL RECESSIVE • Disease is in HOMOZYGOTES • More UNIFORM expression than AD • Often COMPLETE PENETRANCE • Onset usually EARLY in life • NEW mutations rarely detected clinically • Proteins show LOSS of FUNCTION • Include ALL inborn errors of metabolism • MUCH more common that autosomal dominant AUTOSOMAL RECESSIVE • • • • • • • • • • Metabolic CF PKU GALACTOSEMIA HOMOCYSTINURIA LYSOSOMAL STORAGE Α-1 ANTITRYPSIN WILSON DISEASE HEMOCHROMATOSIS GLYCOGEN STORAGE DISEASES hematopoetic Hgb S THALASSEMIAS Endocrine CONG. ADRENAL HYPERPLASIA Skeletal EHLERS-DANLOS (some) ALKAPTONURIA nervous NEUROGENIC MUSC. ATROPHIES FRIEDREICH ATAXIA SPINAL MUSCULAR ATROPHYH AUTOSOMAL RECESSIVE PEDIGREE 1) BOTH SEXES INVOLVED 2) GENERATIONS SKIPPED SEX (“X”) LINKED • • • • MALES ONLY HIS SONS are OK ALL his DAUGHTERS are CARRIERS The “Y” chromosome is NOT homologous to the “X”, i.e., the concept of dominant/recessive has no meaning here • HETEROZYGOUS FEMALES have no phenotypic expression (carriers)….usually, this means autosomal “recessive”, right? SEX (“X”) LINKED • • • • • • • • DUCHENNE MUSCULAR DYSTROPHY HEMOPHILIA , A and B G6PD DEFICIENCY AGAMMAGLOBULINEMIA WISKOTT-ALDRICH SYNDROME DIABETES INSIPIDUS LESCH-NYHAN SYNDROME FRAGILE-X SYNDROME SEX LINKED PEDIGREE 1) MALES ONLY 2) GENERATION SKIPPING DOESN’T MATTER SINGLE GENE DISORDERS • ENZYME DEFECT (Most of them, e.g., PKU) – Accumulation of substrate – Lack of product – Failure to inactivate a protein which causes damage • RECEPTOR/TRANSPORT PROTEIN DEFECT (Familial Hypercholesterolemia) • STRUCTURAL PROTEIN DEFECT (Marfan, Ehl-Dan) – Structure – Function – Quantity • ENZYME DEFECT WHICH INCREASES DRUG SUSCEPTIBILITY: G6PDPrimaquine STRUCTURAL PROTEIN DEFECTS • Marfan Syndrome – Fibrillin-1 defect (not -2 or -3) – Tall, dislocated lens, aortic arch aneurysms, etc. • Ehlers-Danlos Syndromes (AD, AR) – Multiple (6?) different types – Classical, Hypermob., Vasc., KyphoSc., ArthChal., Derm – Various collagen defects – Hyperelastic skin, hyperextensible joints Marfan Syndrome • It is a connective tissue disorder manifest in skeleton, eyes and CVS. • 70 to 80% are familial and A.D inheritance • Pathogenesis • Inherited defect in extracellular glycoprotein FIBRILLIN-1( component of mircrofibril) • Microfibril more widely distributed in aorta, ligaments, ciliary zones. • Two froms are Fibrilin 1 and 2 • Microfibril regualte the TGF beta lack of this protein leads to defect in smooth muscle chamges in the vascular system Morphology • Skeletal system • Tall long extremities, • Tapering fingers and toes,Hyperextensible thumb upto the wrist joint • Kyphosis scoliosis • Pectus excavatum • Ectopia lentis(subluxation of the lens) • ocular change is bilateral dislocation, or subluxation, of the lens owing to weakness of its suspensory ligaments CVS • TGF beta signaling contribute to the aortic dilation, • Weakening of the media,intimal tear • MVP(loss of connective tissue support) • Aortic incompetence, • Histologically cystic medial necrosis of the media Ehlers-Danlos Syndromes • Ehlers-Danlos syndromes (EDSs) are characterized by defects in collagen synthesis or structure • tissues rich in collagen, such as skin, ligaments, and joints, are frequently involved in most variants of EDS. Because the abnormal collagen fibers lack adequate tensile strength, skin is hyperextensible and joints are hypermobile • Deficiency of the enzyme lysyl hydroxylase • Deficient synthesis of type III collagen resulting from mutations affecting the COL3A1 gene. This variant (vascular typeIV) • Defective conversion of procollagen type I to collagen, resulting from a mutation in two type I collagen genes (COL1A1 and COL1A2) in arthrochalasia-type EDS • The skin is extraordinarily stretchable, extremely • fragile, and vulnerable to trauma • Minor injuries produce gaping defects, and surgical repair • The basic defect in connective tissue may lead to serious internal complications, including rupture of the colon and large arteries. RECEPTOR PROTEIN DEFECTS • FAMILIAL HYPERCHOLESTEROLEMIA – LDL RECEPTOR defect – Mutations in the gene encoding the LDL receptors which is involved in the transport and metabolism of the cholesterol. – There is loss of feed back control and elevated levels of cholesterol that induce premature atherosclerosis and increased risk of MI. familial hypercholesterolemia • Mutations in the LDL receptor gene impair the intracellular transport and catabolism of LDL, resulting in accumulation of LDL cholesterol in the plasma. • Familial hypercholesterolemia is an autosomal dominant disease. • Heterozygotes have a two- to threefold elevation of plasma cholesterol levels, Homozygotes may have in excess of a fivefold elevation. • Absence of LDL receptors on liver cells also impairs the transport of IDL into the liver, and hence a greater proportion of plasma IDL is converted into LDL. • Two-thirds of the resultant LDL particles are metabolized by the LDL receptor pathway, and the rest is metabolized by a receptor for oxidized LDL (scavenger Receptors) • The LDL receptor binds to apolipoproteins B-100 and E and hence is involved in the transport of both LDL and IDL. •IDL is the immediate and major source for LDL • The receptor-mediated transport of LDL involves binding to the cell surface receptor, followed by endocytotic internalization Within the cell, the endocytic vesicles fuse with the lysosomes, and the LDL molecule is enzymatically degraded, resulting ultimately in the release of free cholesterol into the cytoplasm. NEUROFIBROMATOSIS TYPE 1 AND 2 • Neurofibromatoses compromise two autosomal dominant disorders 100,00 people in USA. • Type 1 Neurofibromatosis is also called as VON RECKLING HAUSEN disease and • Type 2 neurofibromatosis is also called as ACOUSTIC NEURROFIBROMATOSIS. NEUROFIBROMATOSIS • 1 and 2 • 1-von Recklinghausen • 2- “acoustic” neurofibromatosis • 1 – Neurofibromas, café-au-lait, Lisch nodules • 50% of the patients with definite family history and remainder with new mutations. CLINICAL FEATURES • 1.Multiple neural tumors present in or on the body. • 2.Numerous pigmented skin lesions called Café au lait spots • 3. Pigmented iris hamartomas. called as Lisch nodules. Morphology • Neurofibromatoisis type 1 • 3 types of neurofibromas are found in individuals with type 1 • 1. Cutaneous, • 2. subcutaneous and • 3. plexform lesions.(thickened tortuous nerves) Microscopic • Proliferation of all the elements in the peripheral nerves, including neurites, schwann cells, fibroblasts. • Plexform neurofibromas become malignant in 5% of the patients. • Cutaneous pigmentations is second major component which is present in more than 90% of the patients. • They are light brown café au lait macules with smooth borders. • Lisch nodules are iris hamartomas which helps in diagnosis but remain harmless. Café au lait spots Cutaneous Subcutaneous type LISCH NODULES Neurofibromatosis type 2 • It is a autosomal dominant disorder where bilateral acoustic shwannomas and multiple meningiomas are commonly present. • Café au lait spots are present but Lisch nodules are absent. • It is less common compared to type 1. NEUROFIBROMATOSIS • 1 and 2 • 1-von Recklinghausen • 2- “acoustic” neurofibromatosis • 2 – Bilateral acoustic neuromas and multiple meningiomas ENZYME DEFICIENCIES • BY FAR, THE LARGEST KNOWN CATEGORY – SUBSTRATE BUILDUP – PRODUCT LACK – SUBSTRATE could be HARMFUL • LYSOSOMAL STORAGE DISEASES comprise MOST of them LYSOSOMAL STORAGE DISEASES • • • • • • GLYCOGEN STORAGE DISEASES SPHINGOLIPIDOSES (Gangliosides) SULFATIDOSES MUCOPOLYSACCHARIDOSES MUCOLIPIDOSES OTHER – Fucosidosis, Mannosidosis, Aspartylglycosaminuria – WOLMAN, Acid phosphate deficiency • • • • Lack of enzyme activator Lack of subtrate activator protein Lack of transport protein Enzyme replacement therapy is the current use of treatment NIEMANN-PICK • TYPES A, B, C(inherited deficiency of spingomyelinase) • SPHINGOMYELIN BUILDUP • MASSIVE SPLENOMEGALY • ALSO in ASHKANAZI JEWS • OFTEN FATAL in EARLY LIFE, CNS, ORGANOMEGALY TYPE A • Sever infantile form with extensive neurological involvement, • Progressive wasting • Death in early life with in 3 years of life. TYPE B • • • • Organomegaly But no CNS involvement Genetic inheritence The spingomyelinase gene on chromosome 11p5.4 • Missense mutation in TYPE A • Diagnosis spingomyelinase activity by liver and bone marrow biopsy TYPE C • • • • • • Primary defect in the lipid transport Mutation in NPC1 and NPC2 gene. It might be seen in Hydrops fetalis Neonatal hepatitis And still births • • • • • Clinicla features Ataxia Supranuclear gaze palsy Dystonia Psychomotor regression GLYCOGEN STORAGE DISEASES • MANY TYPES (at least 10) • Type 2 (Pompe), von Gierke, McArdle, most studied and discussed, and referred to • Storage sites: Liver, Muscle, Heart MUCOPOLYSACCHARIDOSES • HURLER/HUNTER, for I and II, respectively • DERMATAN sulfate, HEPARAN sulfate buildup – coarse facial features – clouding of the cornea – joint stiffness – mental retardation – URINARY EXCRETION of SULFATES COMMON ALCAPTONURIA • It is autosomal recessive disorder • HOMOGENTISIC ACID metabolism defect DEFICIENCY OF HOMOGENTISIC OXIDASE • Clinically become evident after 30 years. BLACK URINE –BLACK NAILS (OCHRONOSIS), SKIN –BLACK JOINT CARTILAGE (SEVERE ARTHRITIS) • Homogentisic acid binds to collagen cartilages and ligaments ,imparting to these tissues black color(Ochronosis) most evident in ears ,cheeks and nose. • Because of pigmentation the cartilage looses its resilience and become brittle. • The vertebral column(intervertebral discs) mainly involved next knee and shoulders involved. complications • Severe crippling • Osteoarthritis in elderly persons. • Alkaptonuria arthropathy in early age. “MULTIFACTORIAL” DISORDERS • • • • • • • • Cleft lip, palate Congenital heart disease Coronary heart disease Hypertension Gout Diabetes Pyloric stenosis MANY, MANY, MANY, MANY MORE KARYOTYPING • Defined as the study of CHROMOSOMES • 46 = (22x2) + X + Y • Conventional notation is “46,XY” or “46,XX” MORE DEFINITIONS COMMON CYTOGENETIC DISEASES • AUTOSOMES – TRISOMY-21 (DOWN SYNDROME) – 8, 9, 13 (Patau), 18 (Edwards), 22 – 22q.11.2 deletion • SEX CHROMOSOMES –KLINEFELTER: XXY, XXXY, etc. –TURNER: XO TRISOMY-21 TRISOMY-21 • Most trisomies (monosomies, aneuploidy) are from maternal non-disjunction • (non-disjunction or anaphase lag are BOTH possible) • #1 cause of mental retardation • Maternal age related • Congenital Heart Defects, risk for acute leukemias, GI atresias • Most LOVABLE of all God’s children SEX CHROMOSOME DISORDERS • Problems related to sexual development and fertility • Discovered at time of puberty • Retardation related to the number of X chromosomes • If you have at least ONE “Y” chromosome, you are male KLINEFELTER (XXY, XXXY, etc.) • Hypogonadism found at puberty • #1 cause of male infertility • NO retardation unless more X’s • 47, XXY 82% of the time • L----O----N----G legs, atrophic testes, small penis TURNER (XO) • 45, X is the “proper” designation • Complete or partial monosomy of the X chromosome charcteised by hypogonadism in females. • Three types of karyotyping abnormalities in turners syndrome. • 1.57% missing the entire X chromosome result in 45X. • 2.14% have structural abnormalities of the X chromosomes. • 3.29% are mosaics. In infants and Children • The most severely affected patients present since infancy with lymph edema dorsum of the hand and foot. • Swelling of the nape of the neck.(Cystic hygroma) • Bilateral neck webbing • Congenital coarctation of the aorta and biscupid valve. Adults • Failure to develop normal 2ry sexual characteristics. • The genitralia infantile underdeveloped breasts and little pubic hair. • Single most important cause for primary Amenorrhea. • Hypothyroidism and insulin resistance. STREAK OVARIES • In Turner syndrome the fetal ovaries develop early in embryogenesis but due to absence of X chromosome leads to acclerated loss of oocytes which completes by 2nd year. • Menopause occurs before menorche. • Ovaries are reduced and atrophic fibrous strands devoid of ovarian follicle called as STREAK OVARIES. • SHORT STATURE HOMEOBOX gene. • Haploinsufficiency in this gene gives rise to short stature. MOLECULAR DX by DNA PROBES • • • • • • • BIRTH DEFECTS, PRE- or POST- NATAL TUMOR CELLS CLASSIFICATIONS of TUMORS IDENTIFICATION of PATHOGENS DONOR COMPATIBILITY PATERNITY FORENSIC