1 A Self Harm Conference Presentation March 2015

Prevention of Self-Harm and Suicidal
Ideation Conference
26 th March 2015
Welcome
Emma Grinham
Young Person Chair of the Mental Health Anti
Stigma Programme
David Loyd-Hearn
Commissioning Manager Children and Young People
Emotional Health and Wellbeing
Prevention of Self-Harm and Suicidal Ideation
Conference
• Setting the Scene
• Self Harm and serious Case Reviews – lessons learnt
• Acute self harm
• Break
• Northamptonshire Community & Toolkit
• The real story in school
• TaMHS – Mental Health in Schools - setting up an
Emotional Health and Wellbeing Team
• Action planning
• Closing summary
Setting the Scene
Self-Harm = Symptoms
Self-harm across the spectrum
Why is Emotional Well Being and Mental Health for Children important?
Emotional wellbeing underpins being successful at school, making and keeping friendships and making the most of life.
Approximately 50% of lifetime mental illness
starts before the age of 14 and it is estimated that potentially half these problems are preventable.
Self Harm can sometimes be a coping mechanism or fashion, but it can also lead to significant harm and occasionally suicide. It is not the act that matters, but the intent.
Around 1 in 10 children and young people may
have a mental health problem at any one time.
Referrals have increased by 27% in
Northamptonshire over the last 3 years with 6.5% of all children getting support
Self-harming admissions are higher in
Northamptonshire than the national average.
Research suggests self-harming behaviours are average.
Recent Northamptonshire Public Health assessment suggests local wider costs £1347 million due to mental illness
In adulthood half of all women, and a quarter of men will be affected by depression at some stage in their life.
When it comes to children and young people, 1 in
10 children self-harm, with suicide accounting for
20% of deaths in young people between the ages of 15-24.
Key Findings from CYP Survey
(775 Responses)
Unmet needs continue to feature which do not fit in defined Specialist CAMHS criteria e.g. challenging behaviour, self harm as a coping mechanism. We are working together to resolve.
73% of a significant sample of young people have body image concerns, this increases to 90% of the sample of
CAMHS users. Young people suggest this is sometimes a cause for self-harm.
Behaviour Issues account for 52% of
paediatric referrals and a significant number of CAMHS referrals. If untreated, sometimes these cases may lead to selfharm.
We are a national outlier for self harm due to the adherence of NICE guidance, though we are about average in presentation numbers by NHS estimates.
Anxiety and Depression is the number 1
reason for referral (and can lead to eating issues or self harm as a coping mechanism). Young People increasingly find self harm is an acceptable coping
Mechanism.
There is a significant lack of knowledge
of services, what is available and how to access. If in doubt, visit www.asknormen.co.uk
What is self-harm?
• Self-mutilation
• Self-destructive behaviours (compulsively pursued acts that causes self-harm e.g. head banging)
• Self-harm without suicidal intent
• Attempted suicide
• Minority who self-harm attend A&E departments or specialist services
• Most are supported in the community
• Most young people who self-harm do not continue with this into their 20’s
How many young people self-harm?
• Rarer in pre-teens (but locally this is growing)
• 10% of adolescents in the UK self-harm
• At 14yrs; 25% Females & 14% Males experience suicidal ideation
• Only 2-3% present to medical services
• Huge number remain unknown (behaviour self harm has been anecdotally estimated at 50%)
Self Harm is not the issue, it is the cause and intent that matter most. Less than 4% of self harmers go on to have enduring mental health needs.
National and Local Statistics
• 72% of people who seek help for depression are female
• 75% of people who take their own lives are men.
• National rates of self-reported self-harm are 7% for 11-16 year olds but several times higher in those with:
• emotional disorder (28%)
• conduct disorder (21%)
• ADHD (18%).
• Applying national rates to Northamptonshire would mean that 2940 11-16 year olds would report self-harm. Our actual figure is lower, though in schools anecdotal evidence suggests the rates could be as many as 50%.
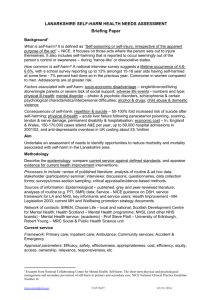
Northamptonshire A&E Admission Rates for Self Harm
Locality
Western Northampton
Kettering
East/Southern Northampton
Central Northampton
East Northants
Daventry North
Corby
Wellingborough
Daventry South
Oundle & Wansford
Not coded
Total
Inpatient
Admissions of 0-19's in
2009-10
Inpatient
Admissions of 0-19's in
2010-11
Inpatient
Admissions of 0-19's in
2011-12
Inpatient
Admissions of 0-19's in
2012-13
51
35
60
51
64
40
55
49
30
44
15
28
48
43
19
30
55
55
20
23
40
28
26
23
29
15
14
1
28
21
17
0
24
14
18
1
25
20
17
4
19
281
15
332
23
337
12
299
200
180
160
140
120
100
80
60
40
20
0
All
Inpatient
All
Inpatient
Admissions Admissions
All
Inpatient
All
Inpatient
Admissions Admissions in 2009-10 in 2010-11 in 2011-12 in 2012-13
Years 0-4
Years 5-11
Years 12-16
Years 17-18
Hospital Admissions (Approx)
• Under 10 yrs Low figures
East Midlands 2010
• 10-14 yrs 350
• 15-19 yrs 1500
• 20-24 yrs 1300
• 25-29 yrs 1000
• 30-34 yrs 800
• 30-39 yrs 1100
• 40-44 yrs 1200
• 45-49 yrs 700
• 50-54 yrs 550
• 55-59 yrs 300
• 60-64 yrs 170
• 65-85+ yrs figures reduce
Under 18’s Hospital Admissions by PCT
East Midlands 2010
• Derbyshire 210 12.4
• Derby City 104 17.4
• Nottinghamshire 164 9.2
• Nottingham City 118 17.3
• Northamptonshire 220 12.8
Per 10,000 area population
• Leicestershire 199 12.2
• Leicester City 91 11.2
• Lincolnshire 155 9.8
• East Midlands Total 1261 12.0
What are we doing about self-harm? Short
Term
• The conference highlights the new self- harm toolkits for Northamptonshire on www.asknormen.co.uk
• Web resources for young people by young people available on http://www.talkoutloud.info/how-do-youfeel/self-harm.aspx
• We have redefined the acute self harm and suicidal ideation pathway
• We are actively working with Northampton and Kettering Locality Forums to embed action plans with excellent examples of best practice at schools such as Northampton Academy & Kettering Buccleuch
Academy.
• Auditing Urgent Care Admissions
• Developing questionnaires for acute self-harmers
What are we doing to reduce self-harm?
Long Term
• The 2014-17 Children and Young People Emotional Wellbeing and Mental Health Strategy looks at improving emotional resilience
• The Partnership are working to improve outcomes relating to challenging sexualised behaviours, drug and alcohol misuse, parental mental health and interpersonal violence
• Initiatives to improve family relationships, resilience and coping strategies o Five to Thrive o Targeted Mental Health in Schools (TaMHS) o Talk Out Loud Anti Stigma Programme o Working with School Nursing as a part of the National Call to Action
• Support of adults with mental health concerns or harmful behaviours
• Developing the Children’s Community Health Services
Priorities for the 2013-17
Emotional Wellbeing and Mental
Health Strategy
• The promotion of positive emotional wellbeing and early intervention
• Improved integration in targeted and specialist services including a single point of access
• Better support for children and young people who are chronically or acutely unwell
• Strengthened thresholds and pathways for behavioural and neurological developmental issues
• Focus on key groups of vulnerable children and young people to prevent poor emotional wellbeing outcomes and ensure there are appropriate interventions when they require additional support
Northamptonshire Children and
Young People Community Health
Transformation Programme
When to make Referrals
Transitions
Occupational
Therapy
Looked
After
Children
Integrated Children & Young People’s
Specialist Health Service
Urgent
Referrals
Single
Specialism
CYP Referral
Management Centre
Integrated
Specialist
Pathway
Non-Urgent
Referrals
Integrated
Assessment &
Treatment
Speech
&
Language
Therapy
Physiotherapy
Countywide offer delivered in
Localities
CAMHS
Community
ADHD &
ASD
Children’s
Specialist
Nursing
Short
Breaks
Community
Paediatrics
CAMHS
In Patients
Children’s
Dietetics
Dealing with Child and Young People presentations within local settings
• Doing Well – expected that universal services engage – e.g. the Talk Out Loud Anti Stigma programme/TaMHS work in schools to promote mindfulness
• Doing alright or with a single issue. Targeted Services to cover –(largely NCC services) – Self Harm as a behaviour may fit into this. School Nursing or Health Visitors may be appropriate
Where professionals are uncertain, it may be worth contacting the CAF Co-ordinator and attending complex case meetings
• SOME NOTICEABLE PROBLEMS – in more than one area. Variable functioning with sporadic difficulties or symptoms in several but not all social areas. Disturbance would be apparent to those who encounter the child in a dysfunctional setting or time but not to those who see the child in other settings. Targeted
Plus services to cover e.g. Counselling services or some services by NCC
If the presentation is largely effecting children within school settings, it may be worth using the pupil premium to commission any support such as family support or education psychology services.
When to make a referral to the Referral Management
Centre for CAMHS/Paediatrics?
• Specialist Services (e.g. CAMHS) to cover - OBVIOUS PROBLEMS – moderate impairment in most areas or severe in one area - Moderate degree of interference in functioning in most social areas or severe impairment functioning in one area, such as might result from, e.g. suicidal preoccupations and ruminations, school refusal and other forms of anxiety, obsessive rituals, major conversion symptoms, frequent anxiety attacks, frequent episodes of aggressive or other antisocial behaviour with some preservation of meaningful social relationships.
• SERIOUS PROBLEMS – major impairment in several areas and unable to function in one area
Major impairment in functioning in several areas and unable to function in one of these areas, i.e. disturbed at home, at school, with peers or in the society at large, e.g. persistent aggression without clear instigation; markedly withdrawn and isolated behaviour due to either mood or through disturbance, suicidal attempts with clear lethal intent. Such children are likely to require special schooling and/or hospitalisation or withdrawal from school (but this is not a sufficient criterion for inclusion in this category).
If uncertain, there is a CAMHS PROFESSIONAL CONSULTATION LINE
Monday to Friday
9.30am—1.00pm
Tel: 0300 1111 022
When issues are treated as urgent?
• Highly Specialist Services (e.g. Crisis team/Inpatient) - SEVERE PROBLEMS - unable to function in almost all situations - Unable to function in almost all areas, e.g. stays at home, in ward or in bed all day without taking part in social activities OR severe impairment in reality testing OR serious impairment in communication (e.g. sometimes incoherent or inappropriate).
• VERY SEVERELY IMPAIRED -considerable supervision is required for safety Needs considerable supervision to prevent hurting others or self, e.g. frequently violent, repeated suicide attempts OR to maintain personal hygiene! OR gross impairment in all forms of communication, e.g. severe abnormalities in verbal and gestural communication, marked social aloofness, stupor, etc.
• EXTREMELY IMPAIRED - constant supervision is required for safety Needs constant supervision
(24-hour care) due to severely aggressive or self-destructive behaviour or gross impairment in
reality testing, communication, cognition, affect or personal hygiene.Working as a self- harm team, consider peer support/supervision and confidentiality issues.
Websites and Links
Northampton Young Healthy Minds Gatewaywww.asknormen.co.uk
CAMHShttp://www.nhft.nhs.uk/main.cfm?type=CONTENTCAMHS
Northampton Youth Forumhttp://www.northampton.gov.uk/info/200124/forums/329/northampton_youth_forum
Northamptonshire Parent Forum Groupwww.northantspfg.co.uk
Out Therehttp://www.thelowdownevents.info/new-youth-group-out-there/
Shooting Starshttp://www.northantspfg.co.uk/shooting-stars/
Talk Out Loud – www.talkoutloud.info
Young Mindshttp://www.youngminds.org.uk/
Youth Space www.youthspace.me
Northamptonshire CAMHS Review: http ://www.neneccg.nhs.uk/cyp-services/
NORTHAMPTONSHIRE’S STRATEGY FOR THE EMOTIONAL WELLBEING AND MENTAL HEALTH OF CHILDREN
AND YOUNG PEOPLE 2014 –2017 http://www.neneccg.nhs.uk/modules/downloads/download.php?file_name=1156
Websites and Links – Youth Counselling
• Youth Counselling across the county http://www.servicesix.co.uk/
• Northampton http://thelowdown.info/
• Daventry http://www.time2talk.org.uk/
• Kettering and Corby http://kyi.org.uk/
• Oundle http://www.oundle.gov.uk/oundle-town-council-properties/courthouse/chat/
• Wellingborough http://www.servicesix.co.uk/
• ADHD Support http://www.autismconcern.net/index.php?option=com_content&view=article&id=195:newadhd-a-as-dual-diagnosis-provision-in-northamptonshire
• Prevention of Self-Harm and Suicidal Ideation Toolkit http://www.asknormen.co.uk/self-harm-andsuicidal-ideation-conference-resources/
• And new for supporting training in 2015/2016 https://www.minded.org.uk/
Self Harm and serious Case
Reviews – lessons learnt
Case Vignette
Maggie Beer
Was her death predictable or preventable?
Who was she?
She was bright, capable and articulate. She had experienced significant neglect in the first 5 years of her life and had been looked after since then.
She took her own life just before her 18 th birthday.
What did we learn?
History was not shared and therefore her journey was not understood.
Agencies did communicate but it was limited and not followed through.
As an articulate young person she was able to ‘keep people away’ but her ‘voice’ was not present.
Was her death predictable or preventable?
Who was she?
She was bright, capable and articulate. She had experienced significant neglect in the first 5 years of her life and had been looked after since then.
She took her own life just before her 18 th birthday.
What have we done?
What did we learn?
Who was she?
History was not shared and therefore her journey was not understood.
Agencies did communicate but it was limited and not followed through.
She was bright, capable and articulate. She had experienced significant neglect in the first 5 years of her life and had been looked after since then.
As an articulate young person she was able to ‘keep people away’ but her ‘voice’ was not present.
Was her death predictable or preventable?
She took her own life just before her 18 th birthday.
What have we done?
• Self-harm pathway developed
• Challenged National protocol for leaving care in terms of the information shared when young people subject to leaving care legislation move from one area to another.
• Reiterated the need to access young people’s history – this is a recurrent theme from local serious case reviews, where for adolescents or infants.
Is it suicide?
•
27 different definitions and Coronial process apply rules subjectively across country so different rates-affects ONS data
•
Small numbers of suicides in each local centre so learning impaired
Nottinghamshire’s
Experience
•
2012 audit
•
Majority of deaths were unpredicted
•
Minority were high levels of previous emotional health concern/deliberate self harm/child protection
•
So how do we PRECICT risk and learn?
Self-Harm – the acute story
Julie Quincey
Named Nurse Safeguarding Children
Northampton General Hospital
Young person up to 18 years presents at A&E following Deliberate Self-harm act
Triaged in A&E, and if no medical treatment is required, transfer to ward (Child or Adult setting) with child self-harm pathway documentation started by A&E staff
Clerked on the ward and medically assessed
Ward ring Child and Adolescent Mental
Services (CAMHS) to request risk assessment
• Prior to 12.00 midday Mon – Fri 9 – 5 call
CAMHS Newland House, 01605 656060
• Between 17.00-22.00 the CAMHS CRISIS team can be contacted for consultation via Berrywood hospital reception on
01604 682682
Patient refuses treatment and absconds from Hospital
Inform police (999) and ask for welfare check clearly record the incident number in the patient record
Police return with patient - continue with pathway
If patient admitted out of hours, they should be kept in overnight and CAMHS informed next working day
CAMHS undertake mental health risk assessment. If safeguarding concerns request ward contacts social care for joint assessment and inform Hospital Safeguarding team
Patient refuses to return, inform GP and refer to children’s social services and ask them to consider referral to CAMHS
Once assessment is completed, and medical review taken place, the patient can be discharged home. If there are safeguarding concerns then a joint discharge planning meeting with children’s social services should ensure safe discharge.
Ensure Paediatric Liaison Form is completed and copied to school nurse and GP, or if Interagency referral to social services has been completed, a copy of this will be sent to GP and School Nurse. Ensure
Safeguarding team is copied in. DOCUMENT EVERYTHING IN THE
PATHWAY, COMPLETE SAFEGUARDING CHRONOLOGY.
Why do we assess the next working day
•
As per NICE guidelines we do the following
•
First they need to be medically stable
•
Secondly they need time out to sleep, to reflect and to rest
•
Then CAMHS will come and assess
Catherine’s Story
Catherine’s story
• Catherine was admitted to NGH having taken an overdose of 24 paracetamol, 8 ibruprofen, 3 nytal and her father’s anti-depressants 15 tablets were missing
• I was present when Catherine was admitted she had come via ambulance
• She was in secondary school, looked very thin, nicely dressed and otherwise looked well looked after
• She came with her older brother, her father and her step-mother
• Her father and step mother were distressed and were struggling to come to terms with
Catherine’s actions, her brother seemed detached
The treatment
• Catherine’s paracetamol levels were high and therefore she required a parvolex drip and stayed in over night
• We weighed her and checked her eating pattern though thin she had a normal BMI and we observed her eating well on the ward
• The next morning she was pronounced medically fit for discharge
• CAMHS attended and did their assessment they felt she was not mentally ill but would follow her up in the community
Catherine and her family tell their story
• I told Catherine she could go home but she refused she said her brother was hitting her and she was not going to go home anymore, she had not shared this with the CAMHS worker
• As the safeguarding nurse I needed to understand more
• It took the next three hours to unpick the story. Catherine had originally lived with her birth mother who struggled with mental health problems both children suffered emotional abuse and after a case conference were placed with their father
• Catherine’s step mother was very calm and understanding but had found
Catherine emotionally shut down and non-communicative
Catherine and her family tell their story
• Catherine shared that her brother Toby was really hard to live with as he had behavioural problems
• I had observed Toby for a number of hours and he struck me as being on the autistic spectrum, I discussed this with his father and step-mother and they agreed to a referral to CAMHS to have him assessed, I later found out he had been diagnosed with high functioning autism
• Catherine agreed to go home once she knew Toby would get help
Catherine
• With the parents agreement we referred Catherine as a child in need to social services, the family were assessed and were eventually signed posted to a life story worker who worked with Catherine
• Though Catherine was not mentally ill she was struggling to make sense of her world as was her brother
• The family had been through a lot of trauma they needed time and help to make sense of the many changes
• To my knowledge Catherine did not self-harm again
Jack’s story
How Jack came to hospital
• Jack was seen by the police he was standing outside his girlfriends house at 3 am in the morning it was snowing heavily, his head and shoulders were covered in snow
• Jack was not making sense when the police spoke to him his words were slurred and his eyes looked dilated, he eventually admitted to the police he had taken an overdose
• The police brought him to A&E and he was admitted to the children’s ward, he was 17 years old effectively homeless and sofa surfing he originally was from out of county
The treatment
• Jack also required a parvolex drip
• He had also self harmed through cutting and required steristrips to his arms and the cuts to his legs were cleaned up
• He appeared to have a chest infection and bloods were taken
• During the night Jack slept deeply
• The next morning he was ready to see CAMHS
Jack takes his leave
• I was rung by the ward, Jack was refusing to stay as he was worried about his girlfriend
• We managed to calm Jack whilst we waiting for CAMHS Jack started to tell me that he had stood every night for the past week outside his girlfriends house, she and her mother didn’t know. He felt it was the only way he could keep her safe and he felt compelled to do it
• Jack appeared to be highly distractible and appeared to be listening to something, I shared my concerns with the CAMHS worker I was beginning to wonder if Jack was manic or indeed psychotic
CAMHS assessed
• CAMHS agreed that Jack was showing pressure of speech, had distorted thinking he believed his mobile was sending him messages but his mobile was completely dead and had been for a number of days
• He was also stating if he left the hospital he would jump from a building
• The CAMHS worker explained to Jack he was ill and said he needed to be admitted to psychiatric hospital
Jack ran
Jack
• Jack was returned to the ward by the police
• Eventually Jack was transferred to psychiatric hospital by the police and the AMHP worker under section 3 of the mental health act
• I do not know the outcome of Jack’s story
Kelsie’s story
Kelsie’s story
• Kelsie had over 20 admissions to NGH in a three month period in her late teens
• She allegedly took overdoses however the tox screen never showed toxic levels in her blood
• She frequently self-harmed by cutting, burning and using ligatures
• Kelsie during this time became looked after by social services
• As her story slowly unfolded it was discovered she had been sexually exploited
• Kelsie has learning difficulties
Kelsie to date
• Kelsie has been very hard to help
• Though she is not mentally ill she does use self-harming behaviour to express her feelings
• She frequently disappears from her foster carers
• She will return to her mother’s and then go missing again
• She is potentially at risk when she does not engage
• Kelsie is now a young adult and continues to be admitted to
NGH with self-harm
What can we learn
• These cases are pretty typical
• Catherine’s was due to the effect of coping with emotional abuse
• Jack had developed bi-polar
• Kelsie has a troubled background, learning disability and is at risk of sexual exploitation
Catherine
• Catherine had had many changes, her new school was aware of the troubles she had experienced with her birth family, but as Catherine was quiet and a good student it was assumed both by school and her parents that she was coping
• Catherine’s history is a high risk for vulnerability to self harm
• Parental mental illness
• Child protection proceedings
• Brother with emerging developmental disorder
• Mentoring at school may have helped
Jack
• Jack was homeless and only became known to services after admission
• Though his girlfriends mother knew Jack was troubled he had hid the homelessness from her and his girlfriend agreed to keep quiet
• The police responded really well, Jack has got an early diagnosis and if he follows his medical regime he should have better outcomes
Kelsie
• Kelsie had been permanently excluded on more than one occasion
• She was well known to social services
• Her learning difficulty had never been formally diagnosed
• Her mother rarely reported her missing
• Kelsie’s vulnerabilities made her ideal for men to sexually exploit
• All workers should be familiar with the CSE toolkit to spot the risk factors and take action sooner
Break
The Community & Schools Pathway and Toolkit
Cazz Broxton
CAMHS Community Liaison Lead
Mike Simons
Senior Educational Psychologist, NCC
& Lead for Northamptonshire TaMHS Programme
Annie Head
Counsellor, Northampton Academy
What is Self-harm?
• Self-harm in the literature is used to cover deliberate acts of injury which may or may not involve a wish to die.
• One example is that of physical mutilation e.g. cutting the skin, repeatedly banging a part of the body etc.
• Most people who injure themselves in what they call selfharm do not intend to intentionally risk their lives
Why do young people Self Harm ?
• Act of self-harm or self injury can be symptoms of distress
• The importance of the act is meaningful to the individual who carries it out
• It is important not to generalise about young people who selfharm
• It can be a way of coping with many different emotions
Explanation from people who Self-harm
To be able to feel anything
A sense of control
The pain proves your human
For the physical pain to overtake the emotional pain
To let the anger out
It is like an addiction
To break numbness
A way of punishing myself
I like watching the blood run
Cycle of self-harm
Negative emotions
Sadness, anger and despair
Tension
Inability to control emotions, maybe using dissociation to cope with tension
Self- harm act
Cutting, burning etc
Positive effects
Endorphins released, tension and negative feelings dispelled for a short period
Negative effects
Shame and guilt over self-harm act
Definition
‘Self-poisoning or self-injury, irrespective of the apparent purpose of the act’
NICE, 2004
The Two Pathways
•
The Community & School pathway and acute pathway
Community
& School
Pathway
If necessary,
Acute
Pathway
The Community & School Pathway
• Improved communication home, school and other agencies
• Self- harm team
• CAMHS consultation through liaison line
• Checking with safeguarding protocols
• Consideration of informing parent/carer
• Risk assessments and forms
The Toolkit
• Toolkit has been developed by Northamptonshire Multi-agency pathway development team and also includes guidance from other national and regional organisations
• Guidance for schools to support children, young people and families at an individual and systemic level
• Bringing a national perspective into the local framework including example policies for schools
• Tools can be used in either a preventative or supportive capacity
• Toolkit contains both practical and theoretical evidence based approaches to helping and supporting young people
Using the Toolkit and Pathway
Scenario....
You are approached by a young person who attends your organisation e.g. school/ community group who has indicated that they have self-harmed by cutting them self. They have shown you the cut on their forearm.
For five minutes on your tables, discuss how you would use the pathway and toolkit to help you to support this young person and decide on a plan of support...
Key aspects to consider
• Working as a self- harm team, consider peer support/supervision and confidentiality issues.
• Informing parents and use of scripts for telephone conversation/ letter to parents to arrange meeting
• Any necessary further referral e.g. Safeguarding, CAMHS, Educational Psychologist,
Community Support?
• Tools that may be useful e.g. proactive support plan, script for talking to a young person, coping strategies and distractions, risk assessment, protective behaviours
• Documenting the support- appropriately evidencing a plan of support in school and ensuring paperwork is clear and relevant should an ongoing referral need to be made
• Consistent documentation to be handed over when relevant between the two pathways in order that all agencies recognise plans of support.
Look after you-supervision and team support are paramount!
The Real Story in School
Northampton Academy
Responding to Self-harm Through an Emotional Health
& Wellbeing Team
Annie Head
Counsellor
Northampton Academy
The Pastoral Support Team
The aim of the Pastoral Support Team is to meet the Social, emotional and Mental Health needs of students. The team consists of two
Pastoral Support Managers, a Counsellor and an
Early Intervention Coordinator who works with families through the CAF process. The Team works alongside the SEND team within the
Inclusion faculty and is part of a graduated response
Responding To The Emotional
Health and Wellbeing of Students
Good referral policies and procedures are key in developing and maintaining a well-functioning team and should be revisited termly to be consistently good.
• They allow containment for students, staff and families.
• They remove reactionary behaviours and the risk of catastrophizing which can potentially increase stress and anxiety.
• They allow good communication and discussion. Confidentiality is always adhered to, yet a degree of transparency is required in the best interest of the student.
• They involve good record keeping, tracking referrals, both internally and externally. This allows us to identify emotional needs through trends and patterns of behaviour. Preventative work can then be tailored to meet the needs of students.
• They ensure the work is allocated appropriately to the right person with the right skill set who will assess the needs of the student accordingly and be able to make good onward referrals if necessary.
Self Harm Cases Presented To The PST
2013-2014
Self- Harm Cases Presented To
The PST 2013-2014
• 92 students – 7% (1:14) engaged in a form of self harm; cutting, scratching, drug use, alcohol, group identity activities (99 scratches, ice cube challenge etc), sexual activity, risky behaviours, negative influences of social media
• The most prevalent year group was 11 with 11% (1:9) of the year group presenting. This is very much in line with national trends. Of this, 48% were girls and 52% boys.
• The second most prevalent year group was 9 with 10% ( 1:10) of students presenting. Again this reflects national trends and thoughts about the developmental conflicts at this age; self and identity. 87% were girls and 13% boys.
• It is anticipated that figures for this academic year will be consistent with 2013-2014.
Responding To Self Harm
To manage this challenge within school it was evident that in addition to the established referral procedures ,the efficacy of which had already been tested, a stringent self harm policy was required.
Following discussions with key staff in school, including the
PST, the Lead Safeguarding manager, School Nurse and the
NHS Nurse:
• A pathway of support was drawn up
• The Self Harm toolkit, launched in October 2014, was tailored to meet the needs of the school
• Both documents were presented as one policy to the
Governing Body who ratified it as a working policy.
• All staff were made aware of this new policy.
9. PATHWAY OF SUPPORT
What you should do if you discover/ have concerns that a student is self-harming
If the student requires If Not
Medical attention
↓ ↓
Contact Mrs Head (0034)
Mrs Smith or Miss Grimes
(Pastoral Team 0047)
Assessment completed with
Contact Mrs Cason Student
School Nurse (0091) ↓
↓ Consider consultation with
If serious or in doubt CAMHS Liaison Line
Paramedics called
Parents/Carers informed ↓
CPO, Safe Guarding
Manager informed.
↓
School Counsellor to
Consider a risk assessment
If yes, staff informed and
If meets CAMHS ← placed on T drive
threshold ↓
↓ School NHS nurse
Informed.
Referral to CAMHS
If not, referral to school
Counsellor. Liasion with
Consider a CAF ← parents/carers support
offered through school or CAMHS
A Case Study- Jane
Jane is 14 years old and is in year 9. Her friends took her to a member of staff as she had told them she had taken some tablets in school after her friends became concerned about her. She had become very anxious and was unable to catch her breath.
The member of staff followed the policy by immediately seeking medical assistance. Jane presented to the school nurse in an extremely agitated manner as her anxiety increased. Other students were present in the medical room.
It was therefore important to contain any anxieties they may be experiencing.
Following immediate observations, the school nurse followed procedures by:
A Case Study - Jane
• Requesting paramedic support
• Contacting the PST
• Contacting parents
Throughout this time, Jane was monitored and kept safe.
I attended the medical room to discover Jane in a very distressed state. She was however able and willing to inform us that she had taken some tablets from home from a family member. She still had the empty blisters packs on her. She also reported that she had disposed of some tablets in a bin in school. Jane was attended to by paramedics who once they had retrieved the tablets from school took Jane to NGH.
• Jane’s friends were informed of events and supported, as was the member of staff who reported the event
• Jane’s tutor, head of year, teaching staff, attendance, the
Lead safe Guarding Manager were all informed.
A Case Study - Jane
Jane was admitted to NGH and assessed by CAMHS. The school NHS nurse was referred to . On her return to school:
• A risk assessment was drawn up and agreed with Jane and her family, to be reviewed monthly.
• A CAF was initiated to support the family. As issues came to light that were impacting negatively on Jane’s emotional well-being it was evident that the family needed support. Concerns were also raised regarding Jane’s risky behaviours and those of her brother, who is now also being supported by school. The case is now being taken to complex case.
• Counselling was arranged for Jane in school.
• Discussions were held with CAMHS who are supporting Jane.
• Jane has a cohesive support plan in place and we hope that through this she will make good progress.
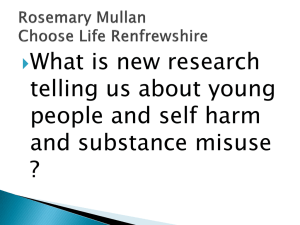
Targeted Mental Health in Schools
•
A holistic approach to promoting MH addressing self-harm and other manifestations of child/young person distress
•
Capacity-building – through training, consultation and coaching.
•
Evidence-based – inc using learning from
TaMHS Project 2009-11
•
Collaborative & Multi-agency
Building-Blocks of Provision for Building
Mentally Healthy Schools in Northamptonshire
January
2015
As informed by
Northamptonshire
Targeted Mental Health in Schools Project & Programme 2009 - 2017
‘Drawing and Emotional Health /
Talking’ Wellbeing Team – to
KS1-4 support students in
KS3&4
Home-Focused Practitioner
Trained in ASD, 123 Magic,
Solihull Approach
Parenting, Theraplay
More Targeted
Programmes or Support
- Wave 3 focused
Peer Support
KS1&2
Peer Mentoring
KS3&4
Building Resilience thru:
‘Zippy’s Friends’ KS1
‘FRIENDS’ KS2/3/4
County PSHE
Prog inc SEAL.
Healthy Schools
Anti Bullying
(inc Cyber)
Shoe Box
& Mental
Health
Handbook
CBT based Group
Work e.g.
‘Growing Optimism’ or ‘RESPECT’
Peer Massage or
Relaxation
Techniques
Headteacher
& Staff Wellbeing
Programmes
Support for child experiencing Insecure
Attachment (inc Theraplay), Anxiety,
Loss, Bereavement, Separation, ADHD,
ASD, Self-harm & Domestic Abuse
Targeted
Programmes or
Support
- Wave 2 focused
Mindful ness
Solihull
Approach & or Protective
Behaviours
Well-Being
Wheels interactive resource
Solution
Focused
Approach
Building
Exam
Resilience
Mental Health
Team or Lead
Person in
School
Whole-School
Behaviour
Management Approach e.g. 123 Magic
Family
SEAL
Parent
Engagement –
Best Practice
Universal
Programmes or
Support-
Wave 1 focused
Essential
Foundation
Programmes
&
Approaches
Mental Health Stigma Programme (MHSP) inc Participation of Children & Young People
Children’s Workforce Core Competencies (from DCSF, ECM 2005)
For evidence base, see www.asknormen.co.uk
For enquiries, please contact tamhs@northamptonshire.gov.uk
Essential Underpinnings for work with children