投影片 1 - 口腔病理科教學網

口 腔 病 理 科
Infection of tooth:
Caries, pulpitis & periapical lesions
齲齒,牙髓炎與根尖病變
陳玉昆副教授 : 高雄醫學大學 口腔病理科
07-3121101~2755 yukkwa@kmu.edu.tw
學 習 目 標
(1)
DENTAL CARIES
Etiology
Epidemiology
Clinical Types
Enamel Caries
Dentin Caries
PULPITIS
Reversible Pulpitis
Irreversible Pulpitis
Pulp Necrosis
學 習 目 標
(2)
Common Diagnostic Techniques
History and Nature of Pain
Reaction to Thermal Changes
Reaction to Electric Stimulation
Reaction to Percussion of tooth
Radiographic Examination
Visual Examination
Palpation of Surrounding Area
Histopathology of Pulpal Diseases
Acute Pulpitis
Chronic Pulpitis
Chronic Hyperplastic Pulpitis
學 習 目 標
(3)
Periapical Lesions
Chronic Apical Periodontitis
Periapical Granuloma
Periapical Cyst
Acute Periapical Conditions
Periapical Abscess
參考資料
References
1.
Sapp JP: Contemporary Oral & Maxillofacial Surgery, p. 61-87
2.
Matalon S et al. Detection of cavitated carious lesions in approximal tooth surfaces by ultrasonic caries detector. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2007;103:109-13
3.
http://www.ne.jp/asahi/fumi/dental/
4.
www.teethwhiteningkits.com/tooth_decay/t5_tooth_decay_children.htm
5.
www.odonto-red.com/cariesdental.htm
6.
www.lezerdent.hu/cariesn.htm
7.
www.areadent.cl/
8.
www.kavo.com/Es
9.
www.uic.edu/classes/dh/dh110/Caries_files
10.
http://iwate8020.jp/know/caries.html
11.
http://www.suwaneedental.com/cariesprevention.htm
12.
http://www.drfarid.com/fluoride.htm
13.
Oral Pathology Department, Kaohsiung Medical University
14.
Opal S, Garg S, Jain J, Walia I. Genetic factors affecting dental caries risk.
Aus Dent J 2015; 60:2-11
15.
維基百科
Etiology
It is a multifaceted disease involving an interplay among the teeth , oral host factors of saliva , microflora , and external factors of diet .
It is a unique form of infection with acidic and proteolytic bacteria for enamel caries
Etiology
Refs. 3, 4
Etiology
Mechanism of dentin sensitivity
(Trabsient receptor potential channel, TRP)
• Neurogenic
•
Hydrodynamic
•
Odontoblastic
Refs. 1, 3
Etiology
Venn diagram showing interplay of genetic factors
Ref. 14
Etiology http://www.experimentalgameplay.com/game.php?g=46
Refs. 4, 6
Etiology
Refs. 10, 11
Etiology
The Caries Balance
Pathological Factors
Acidogenic bacteria
[Streptococci mutans]
Reduced salivary function
Frequency of fermentable carbohydrate ingestion
Protective Factors
Saliva flow & components
Proteins, calcium phosphate fluoride, immunoglobulins in saliva
Extrinsic chlorhexidine
Caries No Caries
Saliva - contains materials for remineralization
- calcium and phosphate ions
Healthy tooth enamel rods Enamel rods demineralized
(broken down by acid)
Enamel rods remineralized, rebuilt, by fluoride & minerals in saliva
Refs. 5, 12
Etiology
製作氟托 (Fluoride tray)
Refs. 13
Epidemiology
1 of common chronic diseases in the world
Prevalence - increased in modern times
Increase associated with dietary changes
Trend beginning to decline in some countries
(i.e. certain segments of US, Western Europe,
New Zealand, and Australia)
Cause of decline?
It is attributed to fluoride
Ref. 5
DENTAL PLAQUE = gelatinous mass of bacteria
Clinical Types
Pit and fissure
Smooth surface
Cemental
Recurrent
Clinical Types (1)
Pit and fissure caries : the most common type
: appear at an early age
: on the occlusal & buccal surfaces of the molars
Refs. 1, 4
Clinical Types (2)
Ref. 6
Clinical Types (3)
Low laser
Ref. 8
Clinical Types (4)
Ref. 8
Clinical Types (5)
Ultrasonic caries detector
檢查前先將受檢牙齒吹乾、棉卷擦乾,
再將感應器放置在頰側並且直接面對受檢鄰接面
Ref. 2
Clinical Types (6)
Smooth surface caries: less common
:occurs on the labial surface & proximal area
Ref. 1
Clinical Types (7)
Refs. 1, 6
Clinical Types (8)
Cemental (root) caries
1. Found in older people, especially, gingival recession
2. Progress differently than enamel & dentin caries because root surfaces are soft, thin, and subject to chemical erosion and abrasive action during tooth brushing
3. Both acid and enzyme producing bacteria and thin layer of dentin results in rapid progression into pulp
Ref. 1
Clinical Types (9)
Recurrent caries arises around an existing restoration as a result of marginal leakage
Marginal leakage is a situation predispose the tooth to accumulate bacteria ( av. diameter: 2000 nm ), and food
Clinical Types (10)
Acute (rampant) caries and chronic caries are terms used to denote the rate that dental caries progresses in patients
Ref. 4
Clinical Types (10)
Rampant caries
Frontal view
Upper view Lower view
Ref. 13
Enamel Caries (1)
Smooth surface enamel caries is most commonly located on the mesial and distal surfaces at the point of contact with the adjacent tooth (“interproximal caries”).
The less common lesions on the buccal and lingual surfaces
Arrested form
chalky appearan ce
Advanced form
Cavitation
Ref. 1
Enamel Caries (2)
Hypocalcified enamel - structure is abnormal
- not weakened, surface is hard
Incipient caries - porous weakened structure
- surface is softened
Arrested caries (remineralized) - strong, surface is hard
Active caries - cavitated, weak enamel, surface is soft
Ref. 1
Enamel Caries (3)
Hypocalcified enamel
– restore only for esthetics
Incipient caries
–
anti-microbial (remineralization)
restore (after remineralization)
only for esthetics
Arrested caries (remineralized)
–
restore only for esthetics
Active caries
–
anti-microbial + restorative
Enamel Caries (4)
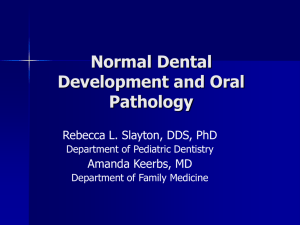
Histopathology – Four zones on ground section
1. Translucent zone: advancing front of initial demineralization
2. Dark zone: remineralization
3. Body of lesion: region of maximal demineralization
4. Surface zone: remain unaffected until it is collapsed forming a cavity
Surface zone
Body of lesion
Dark zone
Translucent zone
Enamel
Ref. 1
Enamel Caries (5)
Incipient Lesion - 4 Zones
Zone 1 - translucent zone
Zone 2 - dark zone
Zone 3 - body of the lesion
Zone 4 - surface zone lesion = cone shaped
B SZ
Ref. 9 body of lesion (B) appears dark beneath relatively INTACT SURFACE ZONE
Enamel Caries (6)
Incipient Lesion - 4 Zones
Zone 1 - translucent zone
Zone 2 - dark zone
Zone 3 - body of the lesion
Zone 4 - surface zone
TZ
DZ
B
Ref. 9
TRANSLUCENT ZONE (TZ) present at advancing front of lesion
DARK ZONE superficial to TZ
Enamel Caries (7)
Zone 1 - translucent zone
1. deepest zone - closest to pulp
2. advancing front of lesion
3. appears structureless - (polarized light)
4. pore volume - 1% - > 10
normal enamel
5. pores/voids form along prism boundary due to ease of hydrogen ion penetration from caries process
Enamel Caries (8)
Zone 2 - dark zone
1. does not transmit polarized light
2. caused by presence of lots of tiny pores which are too small to absorb quinoline
( 奎林 ) ( C
9
H
7
N ) (polarized light)
3. air/vapor filled pores - opaque
4. pore volume - 2 to 4 %
5. remineralization - increase in size of dark zone
6. size of dark zone indication of amount of remineralization
Ref. 15
Enamel Caries (9)
Zone 3 - body of lesion
1.
largest portion of lesion
– in demineralization phase
2. largest pore volume - 5% at periphery
25% at center
3. straie of Retzius well marked
4. first penetration of caries enters enamel via the striae of Retzius
– which provides access to rod prism cores
5. BACTERIA may enter if pores large enough
Enamel Caries (10)
Zone 4 - surface zone
1. relatively unaffected by caries attack
2. lower pore volume than body of lesion
3. radiopacity - similar to unaffected enamel
4. surface in contact with saliva
– hypermineralized by fluoride
5. serves as barrier to bacterial invasion arresting caries process
– may result in rough, but hard surface
Dentin Caries (1)
This stage of caries progression requires a different mixture of bacterial colonies than is necessary for enamel caries.
Bacteria strains capable to produce large amounts of proteolytic & hydrolytic enzymes , rather than acid-producing types of enamel caries.
Ref. 1
Dentin Caries (2)
Dentin caries advance through 3 changes
1. weak organic acid demineralizes dentin
2. organic material of dentin ( mostly collagen ) is degenerated and dissolved
3. loss of structural integrity, followed by bacterial invasion
Five microscopic zones
5
4
3
2
1
Dentin Caries (3-1)
Enamel
Dentin
Ref. 1
Dentin Caries (3-2)
Zone 1 : deepest zone, fatty degeneration the earliest changes where bacterial enzymes in dentinal tubules causing breakdown of cell membrane of dentin releasing lipid
Zone 2 : translucent zone, a band of hypermineralized dentin and sclerotic
Zone 3 : demineralization, softer dentin due to bacterial enzymes
Zone 4 : brown discoloration, reduction of mineral with bacteria within dentinal tubules
Zone 5 : cavitation, no mineralization and organic component is partially dissolved by the bacteria
Bacteria in dentin tubules
Liquefaction
Ref. 1
Dentin Caries (4)
Dentin - 5 zones of slowly progressing lesion
Zone 1 - Normal dentin
Zone 2 - Subtransparent dentin (affected)
Zone 3 - Transparent dentin
Zone 4 - Turbid dentin
(in advanced lesions - infected)
Zone 5 - Infected/Necrotic dentin
Dentin Caries (5)
Zone 1 - Normal dentin
dentinal tubules with smooth odontoblasts
no crystals in lumen
NO BACTERIA in tubules stimulation - elicits pain
Dentin Caries (6)
Zone 2 - Subtransparent dentin
AFFECTED - not infected
zone of demineralization - by acid from caries
capable of remineralization
damage to odontoblastic processes
NO BACTERIA
stimulation - elicits pain
Dentin Caries (7)
Zone 3 - Transparent dentin
softer than normal dentin
AFFECTED - not infected zone of demineralization - by acid from caries
capable of remineralization large crystals
NO BACTERIA stimulation - elicits pain
Dentin Caries (8)
Zone 4 - Turbid dentin
zone of bacterial invasion
filled with BACTERIA very little mineral present
collagen irreversibly damaged will not self-repair / no re-mineralization must be REMOVED
Dentin Caries (9)
Zone 5 - Infected dentin
NECROTIC dentin in advanced lesions
decomposed dentin lots of BACTERIA
no recognizable dentin structure no collagen / no mineral must be REMOVED
Pulpitis
It is an inflammation of the pulpal tissue that may be acute or chronic, with or without symptoms, and reversible or irreversible.
Ref. 1
Reversible Pulpitis
Decision of reversible or irreversible pulpitis
1. Conservatively restore the defective tooth structure
2. Removed the disease pulp disease
3. Remove the entire tooth
1. Whether pain is spontaneous or stimulated
2. Duration of pain
3. Nature of pain described by patient
Ref. 7
Reversible Pulpitis
Reversible pulpitis/hyperemia limited inflammation of pulp tooth can recover - if caries producing irritant removed
ASAP clinically - pain that lingers <10 seconds hyperemia = increased blood flow and volume pulp surrounded by dentinal walls which limits drainage of this increased blood flow/ volume
Irreversible Pulpitis
Inflammation of pulp
Tooth can NOT recover
– if caries producing irritant removed ASAP
Clinically - pain that lingers > 10-15 seconds
Throbbing, continuous pain
Pain upon heat relieved by cold
Partial / total pulp necrosis
Treatment
– endo / extraction
Ref. 3
Differences between Pain Symptoms
Reversible
Elicited
Sharp
< 20 minutes’ duration
Unaffected by body position
Easily localized
Irreversible
Spontaneous
Dull
> 20 minutes’ duration
Affected by body position
Difficult to localize
Refs. 1, 3
Pulp Necrosis
It is the term applied to pulp tissue that is no longer living
A result of a sudden trauma (e.g. a blow to the tooth in which blood supply has been severed), there will be no symptoms for a time
Discoloration of tooth
Ref. 1
Common
Diagnostic Techniques (1)
1.
History and nature of the pain
2.
Reaction to thermal changes
3.
Reaction to mild electric stimulation
4.
Reaction to percussion of the tooth
5.
Radiographic examination
6.
Visual clinical examination
7.
Palpation of the surrounding tissue
Common
Diagnostic Techniques (2)
History and Nature of Pain
Reversible pulpitis: sharp and intense
Irreversible pulpitis: dull, nagging, vague in location
Common
Diagnostic Techniques (3)
Reaction to Thermal Changes
Reversible pulpitis: immediate, sharp pain, last for up to 20 minutes
Irreversible pulpitis: less sharp, last for a much longer time
Common
Diagnostic Techniques (4)
Reaction to Electric Stimulation
Reversible pulpitis: nerves will be easily excited respond at a lower than normal voltage
Irreversible pulpitis: nerves severely damaged a higher level of voltage
Common
Diagnostic Techniques (5)
Reaction to Percussion of Tooth
Percussion pain indicates an inflammation in the apical periodontal tissue.
It is useful when pain is vague and offending tooth is not apparent.
Common
Diagnostic Techniques (6)
Radiographic Examination
It is useful to determine if the inflammatory response has reached the periapical tissue.
The presence of a radiolucency at tooth apex is a great help to determine the vague pain in mandible or maxilla.
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 4
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 4
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 3
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 3
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 3
Common
Diagnostic Techniques (6)
Radiographic Examination
Ref. 3
Common
Diagnostic Techniques (7)
Visual Examination
It may reveal a cortical expansion of alveolar bone
A small, raised, reddish papule (parulis) over tooth apex indicating an opening of the sinus tract of periapical abscess
Ref. 1
Common
Diagnostic Techniques (8)
Palpation of Surrounding Tissues
It indicates that the inflammation has reached the tissue surround tooth apex
This is an indication that pulp is necrotic required treatment
Histopathology of
Pulpal Disease
Acute Pulpitis
Pulp horn
Intrapulpal hemorrhage
Ref. 1
Histopathology of
Pulpal Disease
Chronic Pulpitis
Spherical calcification
Dystrophic
(linear) calcification
Ref. 1
Histopathology of
Pulpal Disease
Chronic Hyperplastic Pulpitis
1. It is a rare condition that is primarily confined to the molars of children
2. It is the result of rampant acute caries in young teeth that quickly reaches the pulp before it becomes completely necrotic
Periapical Lesions
Major factors involve
Presence of an open or closed pulpitis
Virulence of the involved microorganisms
Extent of sclerosis of the dentinal tubules
Competency of the host immune response
Chronic Apical Periodontitis
It is the earliest radiographic evidence of extension of the inflammatory process from the pulpal chamber into the adjacent periodontal membrane around the apical foramen
Chronic Acute
Chronic apical periodontitis
Periapical granuloma
Periapical cyst
Periapical abscess
Osteomyelitis
Chronic
Osteomyelitis
Cellulitis Garre’
Osteomyelitis
Ref. 1
Periapical Granuloma
1. It occurs when a pulpitis progresses into a periapical lesions
2. The most common lesion occurs after pulpal necrosis
3. It is usually painless, progresses slowly, and seldom becomes very large
Radiography
Well-defined radiolucency with corticated outline
Ref. 1
Periapical Granuloma
Histopathology
Remodeling cortical bone
Fibrous tissue
Granulation tissue
Root apex
Ref. 1
Radicular (Periapical) Cyst
1. It is a common development of long-standing, untreated periapical graunoma
2. The epithelial lining is derived from rests of Malassez
3. The rests are stimulated to proliferate by low-grade inflammation of the periapical granuloma
Epithelial proliferation
Histopathology
Cystic space
Epithelial distintegration
Ref. 1
Radicular (Periapical) Cyst
Histopathology
Cystic lumen
Epithelial lining
Cholesterol
Fibrous capsule
Ref. 1
Radicular (Periapical) Cyst
Radiography
Ref. 1
Acute Periapical Conditions
Factors associated
Young tooth with open tubules
Rampant caries
Closed acute pulpitis
Presence of high virulent microorganisms
Weakened host defense system
Ref. 3
Periapical Abscess
1. It is the initial lesion that develops when the circumstances are adverse
2. The most painful patient condition and is potentially one of the most dangerous
3. Progression of acute pulpitis that has exudates extending to adjacent soft and hard tissues
Histopathology
Ref. 1
Periapical abscess
Ref. 7
Periapical abscess
Ref. 7
下列何者是 reversible pulpitis 的特徵 ?
a)Difficult to localize b)Sharp pain c)Dull pain d)Spontaneous pain e)Long duration
(1) a, b, d (2) b (3) c, d (4) e
SUMMARY (1)
DENTAL CARIES
Epidemiology
Clinical Types
Enamel Caries
Dentin Caries
SUMMARY (2)
PULPITIS
Reversible Pulpitis
Irreversible Pulpitis
Pulp Necrosis
SUMMARY (2)
Common Diagnostic Techniques
History and Nature of Pain
Reaction to Thermal Changes
Reaction to Electric Stimulation
Reaction to Percussion of tooth
Radiographic Examination
Visual Examination
Palpation of Surrounding Area
Histopathology of Pulpal Diseases
Acute Pulpitis
Chronic Pulpitis
Chronic Hyperplastic Pulpitis
謝 謝