Appraisal of Stress_FINAL26 June
advertisement

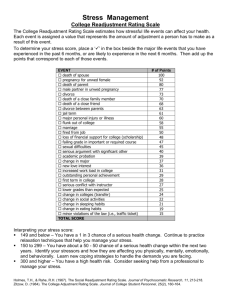
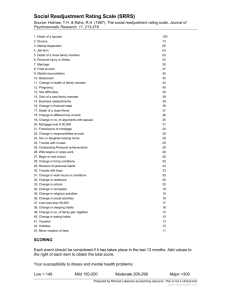
Appraisal of Stress and Coping Difficulties of Hypertensive and Normotensive Males and Females Dr. Sangeeta Rath Professor & Head P.G. Department of Psychology Ravenshaw University Mrs. Stuti Das Correspondence should be sent to Prof. (Dr) Sangeeta Rath, Professor and Head, Department of Psychology, Ravenshaw University, Cuttack – 753003, Odisha, India Abstract Psychologists have been studying stress and its impact on physical and psychological health for decades. Stress is frequently seen as a significant contributor to disease and clinical evidence in mounting for specific effects of stress on immune system and hypertension. Research in this area suggests that genetic susceptibility to hypertension and frequent stress exposure are important modulating factors in stress related hypertension. This study attempts to compare the perception of stress and coping difficulties of hypertensives and normotensives as well as male and female participants. The study adopted a 2 (hypertensives and normotensives) x 2 (males and females) factorial design. Two hundred and forty participants (120 chronic hypertensives and 120 normotensives) are selected from Gurgaon, Delhi. Out of 120 hypertensives, there are 60 males and 60 females. Similarly 60 healthy males and 60 healthy females, not suffering from hypertension or any other disease are selected. The participants of all the four groups are compared with respect to their appraisal of stress and coping difficulties. The result indicates that hypertensives perceived more stress and coping difficulties in personal, family and finance related stressful events compared to normotensives. Males perceived more stress and coping difficulties in personal and finance related events and females in family related events. Introduction : Psychologists and medical professionals have realized that psychological factors affect all aspects of one’s physical well-being. It has been established that belief, attitude, personality and lifestyle of an individual contribute significantly to the onset, cure as well as prevention of the disease. Because of the close interdependence of body and mind, it is increasingly clear that mental and physical healths are intimately related. Hypertension is a psychophysiological disorder characterized by physical symptoms and to some extent caused or worsened by psychological and emotional factors. A person needs some blood pressure to stay healthy, without it, there is no way blood could make it around the body. Throughout the day, the Keywords: stress, coping, hypertension, gender Body adjusts its blood pressure; the normal level for blood pressure is around 120/80. In some people, if blood pressure stays too high all the time, then it is called “Hypertension”. In other words, high blood pressure is a condition in which the force of the blood against artery walls is high enough which may eventually cause health problems. Blood pressure is determined by the amount of blood the heart pumps and the amount of resistance to blood flow in the arteries. The more the heart pumps and the narrower the artery, the higher is one’s blood pressure. The top number (systolic blood pressure) shows the force of the blood vessels when the heart pumps. The bottom number (diastolic blood pressure) shows the force of the blood in the vessels when the heart is between beats. Blood pressure around 140/90 or above is considered high blood pressure or hypertension. -1- High blood pressure is often called a “silent killer” because it has no symptoms, so one may not be aware that it is damaging arteries, heart and other organs. The possible health consequences that can happen over time when high blood pressure is left untreated include damage to the heart, coronary arteries and kidneys and it may lead to brain stroke. It may also lead to loss of vision and loss of memory. Though the exact cause of hypertension is unknown several factors have been empirically proved to be highly associated with the condition. High blood pressure may be caused because of some psychological factors like anger, depression, fright, stress etc. People who experience high level of stress and adopt poorer coping strategies are at increased risk for high blood pressure. Currently India is not as hypertensive as its neighbouring countries, but it appears that the disease will become a major health concern in the coming years. According to World Health Statistics 2012 report, India has low rates of hypertension compared to world figures. In India, 23.10 percent men and 22.60 percent women above 25 years suffer from hypertension. India fares little better than the global average of 29.20 in men and 24.80 in women respectively. Anything that poses a challenge or a threat to an individual’s well-being is a stress. Stress seems to affect some people more than it does to others and researchers have looked for personality variables that might account for the different effects of stress. People exposed to precisely the same stressful life event can experience it in vastly different ways. One person may be overwhelmed physically and emotionally because of the occurrence of a negative event, while another may not notice the event and proceed relatively unconcerned. One person might instantly tackle the source of the stress while another does little but -2- worry about it for days. One person may be able to relax and put the problem out of mind while another is so distressed that restful sleep is out of question. A relationship between antecedent psychosocial stress and illness has been recognised for centuries (Cooper & Payne, 1991). Many recent studies in India also have established the relationship between chronic disease severity and psychosocial stress (Mohan, 1999; Mohan et al., 2000).People vary on their reactivity to stress and reactivity to stress can affect vulnerability to illness. Differences in reactivity are believed to contribute especially in the development of hypertension and coronary artery diseases (Clark, Moore & Adams, 1998). Stress has been suspected as a contributor to hypertension for many years (Henry & Cassel, 1969). Stress can cause hypertension through repeated blood pressure elevations as well as by stimulations of the nervous system to produce large amount of vasoconstricting hormones that increases blood pressure (Carroll et al., 2001). Laboratory studies that exposed people to stress reliably show increased blood pressure responses (Girdler et al., 1996). In a path breaking study, Benshop et al., (1995) reported effects of psychosocial stress and immunological activities and cardiovascular reactivity viz blood pressure and heart rate. Some other studies also reported stress to induce increase in heart rate and blood pressure. In a study Mohan et al., (2000) found significant differences between hypertensive and cardiac group and health controls on life events stress and daily hassles. High blood pressure can result from exposure to chronic social, personal and financial conflict and from job strain, specifically when there is the combination of high demands with little control (Pickering et al., 1996). However, evidence is mixed concerning the effects of stress on the development of hypertension. -3- Men and women report different reactions to stress, both physically and mentally. They attempt to manage stress in very different ways and also perceive their ability to do and the things that stand in their way in markedly different ways. Matud (2004) examined gender differences in stress and coping in a sample of 2816 people (1566 women and 1250 men). They found that women scored significantly higher than the men in chronic stress and minor daily stressors. Although there was no difference in the number of live events experienced, women rated their life events as more negative and less controllable than men. Furthermore, they found women listed family and health related problems as more stressful than men, whereas men listed finance and work related events as more stressful. Women tend to be more involved in relationship than men and suffer more when they are disrupted. It has also been found that women are more likely than men to feel that having a good relationship with their families and friends is most important to them than their jobs. Kesslor & McLeod (1984) examined evidence from five epidemiologic studies of men’s and women’s exposure and vulnerability to life events. They found that loss of income was reported to be more stressful by men where as the death of loved ones and family related events were perceived more stressful by women. Most of the research on stress and illness has been conducted on the role of specific stressful life events in predicting ill health. One of the most widely used measures has been the Social Readjustment Rating Scale (SRRS) developed by Holmes and Rahe (1967). This scale consists of a list of 42 life events arranged in order, from most to least stressful. Each event carries an assigned value ranging from 100 points for death of a spouse to lesser points for minor violations of the law. Subjects are asked to check the items that they have experienced during a -4- recent period, usually the previous 6 to 24 months. The items values are added up for each person and total scores are correlated for future events such as incidence of illness. Holmes and Rahe developed their scale by assuming that change in life adjustment is a key ingredient in stress. The precise character of an event or situation is not a reliable indicator of the degree of stress an individual feels or of how that stress affects the individual’s physical and psychological health. As people vary in what they consider to be stressful, researchers feel that perceived stress is better measure of stress than are instruments that measure whether people have been exposed to particular events. Lobel, Dunkel- Schetter, & Scrimshaw (1992) suggested that perceived stress predicts a broad way of health outcome. The present study attempts to find the role of hypertension and gender on the perception of stress and coping difficulties using Social Readjustment Rating Scale. Method The primary purpose of the study is to examine the influence of the psychological factors like perception of stress and coping difficulties of hypertensives and normotensives as well as male and female participants. Participants Two hundred and forty participants (120 participants with chronic hypertension and 120 healthy participants without hypertension) were selected from Gurgaon, Delhi. The 120 participants without hypertension are absolutely healthy and not suffering from any other disease. Out of the 120 hypertensives, 60 were males and 60 were females. Hypertensives were suffering from hypertension for minimum 5 years. Similarly, in the case of 120 normotensives, -5- there were 60 males and 60 females. All the participants were educated and their minimum qualification was fixed at graduation. The age range of the respondents varied from 45 to 50 years and their average age was 47.41 years (SD = 1.39). Almost all the participants had middle socio-economic status. Instrument Measure of Stress and Coping . The Social Readjustment Rating Scale developed by Holmes and Rahe (1967) was employed to evaluate the degree of coping necessary on the part of the participants while encountering various stressful situations of life. The Social Readjustment Rating Scale (SRRS) is one of the most widely used measures in the stress literature, frequently used by researchers and practitioners. The SRRS consists of forty two life events ranging in stressfulness from death of a spouse to losing some valuables. The life events are divided into three categories that is family, personal and finance related stressful encounters. Participants are asked to rate the items according to the degree of the adjustment required by them. The rating may vary from 1-100. Out of the total forty two stressful situations given in the questionnaire, sixteen stressful situations are related to family issues, twenty three to personal issues and three of them are related to financial issues. Participants are asked to indicate the units of adjustment required to deal with each event according to its intensity and length of time necessary to accommodate regardless of the desirability of the event. Marriage is arbitrarily assigned a stress value of fifty units. Using this as a reference point all other items are evaluated accordingly. For example, an event twice as stressful as marriage would be assigned a value of 100 and an event one fifth as stressful as marriage would be assigned a value of 10. However, rating ‘1’ indicates minimum adjustment necessary and rating ‘100’ indicates maximum -6- adjustment required. Total score was calculated by adding scores given to individual stressful situation. The scale is often used to measure in clinical as well as general adaptation literature. Rahe and Holmes (1967) in an unpublished report document the positive association between Life Change Unit (LCU) scores and disease susceptibility. Procedure The study involved a 2 (hypertensives versus normotensives) x 2 (males versus females) factorial design. The participants of these four quasi experimental groups were compared with respect to their perception stress and coping difficulties. Results The coping variables include the consideration of readjustment in three dimensions. Those are family, personal and financial dimensions. The analysis of variance computed on family readjustment scores of the participants shows significant main effect for status, F (1, 236) = 773.78, P < .01 (See Table 1). Table 2, indicates that hypertensives experienced higher personal readjustment difficulties compared to normotensives (M = 69.03 and 54.67, respectively). The result also shows significant effect for gender, F (1,236) = 278.95, P < .01. The examination of mean scores reveals that females experienced greater family readjustment difficulties compared to males (M = 66.16 and 57.54 respectively). However, the analysis shows a non-significant effect for status x gender, F (1, 236) = 0.23,n.s. -7- Table 1 Analysis of Variance Performed on Family Readjustment Scores of Participants. Sources df MS F Status 1 12378.00 773.78** Gender 1 4462.23 278.95** Statues x Gender 1 3.69 Error 236 0.23 15.99 Note : P<.01** Table 2 Mean Ratings on Family Readjustment Scores of Participants. Groups Males Females M SD Hypertensive 64.85 3.67 Normotensive 50.23 3.39 Combined 57.54 M SD M 73.22 3.41 69.03 59.11 5.22 54.67 66.16 -8- Combined The analysis of variance performed on personal readjustment scores of participants shows significant effect for status F (1,236) = 1196.98, P<.01 (See Table 3). As shown in Table 4, hypertensives experienced greater coping difficulties on personal dimensions of coping compared to normotensives (M=77.50 and 62.13, respectively). The result also shows significant effect for gender F(1,236)=353.36, P<.01. As depicted in Table 4, males report greater personal readjustment difficulties compared to females (M=73.99 and M=65.63 respectively). Further analysis shows nonsignificant effect for status x gender, F (1,236)=1.7,n.s. That shows status and gender together have no effect on personal readjustment scores of the participants. Table 3 Analysis of Variance Performed on Personal Readjustment Scores of Participants. Sources df MS F Status 1 14198.64 1196.98** Gender 1 4191.62 353.36** Statues x Gender 1 Error 236 21.01 11.862 Note : **P<.01 -9- 1.77 Table 4 Mean Ratings on Personal Readjustment Scores of Participants. Groups Males Females M SD M Hypertensive 81.99 4.21 Normotensive 66.00 4.06 Combined 73.99 Combined SD M 73.03 1.73 77.50 58.24 3.19 62.13 65.63 Table 5 Analysis of Variance Performed on Financial Readjustment Scores of Participants. Sources df MS F Status 1 17703.13 1895.08** Gender 1 3422.49 366.37** Statues x Gender 1 Error 236 22.21 9.34 Note : **P<.01 - 10 - 2.37 Table 6 Mean Ratings on Financial Readjustment Scores of Participants. Groups Males Females M SD Hypertensive 88.34 3.26 Normotensive 71.78 2.67 Combined 80.05 M Combined SD M 81.39 1.96 84.87 63.60 3.97 67.69 72.50 The analysis of variance performed on financial readjustment scores of participants reveals significant main effect for status, F(1,236) = 1895.08, P<0.01 (See Table 5). As shown by Table 6, hypertensives show more readjustment difficulties in financial matters compared to normotensives (M=84.87 and 67.69 respectively). The result also shows significant effect for gender, F(1,236)=366.37, P<0.01. The examination of mean scores reveals that males perceive more readjustment difficulties in financial matters compared to females (M=80.05 and 72.50, respectively). Further analysis shows a non significant effect for status x gender, F (1,236)=2.37,n.s. That shows status and gender together have no effect on financial readjustment scores of the participants. - 11 - Table 7 Analysis of Variance on Overall Readjustment Scores of Participants. Sources df MS F Status 1 211869.14 5251.76** Gender 1 860.482 21.33** Statues x Gender 1 Error 96.596 236 2.39 40.34 Note : P<.01** Table 8 Mean Ratings on Overall Readjustment Scores of Participants. Groups Males M Females Combined SD M SD M Hypertensive 240.18 6.78 237.66 4.85 238.92 Normotensive 182.01 6.30 176.97 7.22 179.49 Combined 211.09 207.31 - 12 - The analysis of variance performed on overall readjustment difficulties scores of participants reveals significant main effect for status, F (1,236)=5251.76, P<.01 (See Table 7). As shown by Table 8, hypertensives show more overall readjustment difficulties compared to normotensives (M=238.92 and 179.49 respectively). The result also shows significant effect for gender, F (1,236)=21.33, P<.01. The examination of mean scores reveals that males perceive more overall readjustment compared to females (M=211.09 and 207.31, respectively). Further analysis shows a non significant effect for status x gender, F (1,236)=2.39,n.s. That shows status and gender together have no effect on overall readjustment difficulties scores of the participants. Discussion The present finding clearly shows that people having hypertension experience greater amount of stress and they require more readjustments to deal with stressful life events compared to normotensives. They perceived more readjustment difficulties in personal, family and finance related stressful events and also in overall stressful encounters compared to normotensives. The present study also reveals that males perceived greater readjustment difficulties in personal and financial matters where as females perceived greater readjustment difficulties in family matters. Stress produces changes in the body system like increased heart rate and blood pressure. Repeated exposure to stressful events during which heightened blood pressure reactions occurrence may contribute over the long term to the development of chronically high blood pressure. Hypertension results from high - 13 - stress reactivity, possibly genetically based, in conjunction with high stress exposure ( al'Absi & Wittmers, 2003, Schwartz, Meisenhelder, Ma & Reed, 2003). People already diagnosed with hypertension show more readjustment difficulties to a wide range of stressors. The fact that diagnosed hypertensives show blood pressure responses to a wide array of stressors in consistent with the idea that excessive sympathetic nervous system activity - that is reactivity to response to stress - may be significant in the development of hypertension. It may be a fact that factors that usually help people cope successfully with stressful events may not do so with hypertensives. For example, people who feel they have personal control over stressful events usually show less sympathetic nervous system activity. This decrease does not appear to be true for people diagnosed with hypertension. Chronically hypertensive individuals appeared to be more stress sensitive (Fredriksson, Robson & Ljungdell, 1991). This may be a reason for hypertensives to perceive more stress and coping difficulties. Men and women psychologically define stressful events differently. They report different reactions to different types of stress, both physically and mentally. They attempt to manage stress in very different ways. The findings from the present study suggest that females perceive more stress and coping difficulties in family matters than that of males. Males experience greater stress and more readjustment difficulties in personal and financial issues. Many empirical studies have examined the gender difference in the vulnerability to stressful events that occurred to the subjects themselves versus stressful events that occurred to others. It has been found that stressful events that occurred to self were equally associated with depression and anxiety in men and woman but stressful events that happened to others or close family members are associated - 14 - with depression and anxiety in woman. In woman, elevated blood pressure has been related to having extensive family responsibility (Brisson et. al., 1999), Rath and Alam (2012) found that males experienced greater coping difficulties in personal and financial matters and females experienced more coping difficulties in family related matters. Conger et al (1993) got similar findings. They found that women and men experience stressors differently in different domains. Women are more likely than men to report stressful events that involve interpersonal relationships and family, and men are likely to report greater distress in response to finance and work related stress. Males and females experienced stressful events of different domains differently. Since ages males are the bread winners of the family and responsible for financial resources whereas females are the home makers and responsible for family matters. So males give more importance to personal and financial events and perceived more readjustment difficulties in these domains whereas females give more importance to family related events and perceived more adjustment difficulty in this domain. - 15 - References Al’ Absi, M., & Wittmers, L. E., Jr. (2003). Enhanced adrenocortical response to stress in hypertension prone men and women. Annals of Behavioral Medicince, 25, 25-33. Benschop, R.J.m Godaert, G.L., Geenen, R., Brosschot, M., Smet, De, Heijnen, C.J. and Ballieux (1995), Relationship between Cardiovascular and Immunological changes in an experimental stress model, Psychological Medicine, 25, 323327 Brisson,C., LaFlamme,N., Moisan,J., Milot,A., Masse,B., & Vezina,M . (1999). Effect of family responsibilities and job strain of ambulatory blood pressure among white-collar women. Psychosomatic Medicine, 61, 205-213. Carroll, D., Smith, G.D., Shipley, M.J., Steptoe, A., Brunner,E.J., & Marrot, M.G.(2001). Blood pressure reactions to acute psychological stress and future blood pressure status : A 10 year follow-up of men in the Whitehall II study. Psychosomatic Medicine, 63, 737-743. Clark,V., Moore, C., & Adams, J. (1998). Cholesterol concentrations and Cardiovascular reactivity to stress in African American college volunteers. Journal of Behavivoral Medicine, 21, 505-515. Conger, R.D., Lorenz, F.O., Elder.G.Jr.Simons, R.L. & Ge, X, (1993). Husband and Wife differences in response to undesirable life events. Journal of Health and Social Behaviour, 34, 71-88. - 16 - Cooper, C. L, & Payne, R.(1991), Personality and Stress: Individual Differences in the Stress Process. Chichester; Wiley and Sons Fredrikson,M., Robson,A., & Ljungdell,T.(1991). Ambulatory and laboratory blood pressure in individuals with negative and positive family history of hypertension. Health Psychology, 10, 371-377. Girdler, S.S., Hinderliter, A.L., Brownley, K.A., Turner, J.R., Sherwood, A., & Light, K.C. (1996). The ability of active versus passive coping tasks to predict future blood pressure levels in normotensive men and women. International Journal of Behavioural Medicine, 3, 233-250. Henry, J.P., & Cassel, J.C. (1969). Psychological factors in essential hypertension : Recent epidemiologic and animal experimental evidence. American Journal of Epidemiology, 90,171-200. Holmes, T.H., & Rahe, R.H. (1967). The social readjustment rating scale. Journal of Psychosomatic Research, 11, 213-218. Kessler, R.C., & McLeod, J.D. (1984). Sex differences in vulnerable to undesirable life events. American Sociological Review, 49,620-631. Lobel,M., Dunkel-Schetles, C., & Scrimshaw, S.C.M (1992) Prenatal material stress and prematurity: A prospective study of socioeconomically disadvantaged - 17 - women. Health Psychology, 11, 32-40. Matud, M. P. (2004). Gender differences in stress and coping styles. Journal of Personality and Individual differences, 3, 1401-1415. Mohan, J. (1999), Keynote Address: Personality, Cognition and CAD. 3rd International Conference on Cognition, Mental Health and Education. Varanasi, India. Abstract Guide. Mohan, J. (2000), Stress and Coping: The Indian Perspective. Invited Symposium. 27th International Congress of Psychology, Sweden, (Abstract Guide) Pickering, T.G., Devereux, R.B., James, G.D., Gerin, W., Landsbergis, P., Schnall, P.L., et al. (1996). Environmental influences on blood pressure and the role of job strain. Journal of Hypertension, 14(suppl.), S 179 – S 185. Rath, S., & Alam,S. (2003). Perception of stress : Role of asthma and gender. Indian Journal of Health and Well being, 3(2), 552-556. Schwartz, C., Meisenhelder, J.B., Ma, Y., & Reed, G. (2003). Altruistic Social interest behaviors are associated with better mental health. Psychosomatic Medicine, 65, 778-785. - 18 -