Reflex - Bases
advertisement

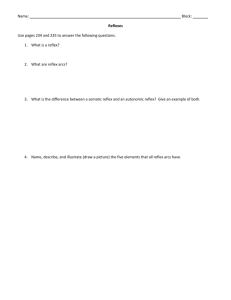
Reflexes and Surgical influences Daniel Robbins Definitions • Stimulation Internal (e.g. conscious decision), External (e.g. mechanical / electrical) • Orthodromic impulse An orthodromic impulse runs along an axon in its normal direction, away from the soma. • Antidromic impulse An antidromic impulse in an axon refers to conduction opposite to the normal • Reflex Automated response, different to that of a decisive reaction, E.g. does not follow hicks law, T = blog2(n + 1) T = time b = constant determined empirically by fitting a line to measured data n = number of equally probable choices Smaller/faster neural pathways etc. This diagram is not 100% accurate as the signal would actually be sent from the muscle not the tendon. However its still quite nice so I left it in. Types of Reflex Autonomic reflex The intrinsic visceral reflexes mediated by control centers in the brain, particularly in the hypothalamus and brain stem, and in the spinal cord, particularly in the lateral horns of thoracic and lumbar spinal cord segments; these reflexes are involved in the automatic adjustment or negative feedback control of internal environment = internal homeostasis. Somatic reflex Any reflex in which the effectors are skeletal muscles, e.g., the patellar reflex, the flexor or withdrawal reflex, the crossed extensor reflex, etc. Categorising reflexes and responses Stretch-reflex A stretch reflex is a muscle contraction in response to stretching within the muscle. It is a monosynaptic reflex which provides automatic regulation of skeletal muscle length. e.g. Ankle Clonus H-reflex The H-reflex is the electrical equivalent of the monosynaptic stretch reflex and is normally obtained in only a few muscles. It is elicited by selectively stimulating the sensory (Ia) fibres of the posterior tibial or median nerve. The stimulus travels along the Ia fibers, through the dorsal root ganglion, and is transmitted across the central synapse to the anterior horn cell which fires it down along the alpha motor axon to the muscle. Reflexes and responses cont. F-wave/F-response The second of two voltage changes observed after electrical stimulation is applied to the skin surface above the distal region of a nerve. F wave properties include: Amplitude (µV) - F wave height Duration (ms) - length of F wave Latency (ms) – period between F wave and initial stimulation Persistence - the number of measurable F waves divided by the number of stimuli. M-wave – – – – Evoked motor unit action potential Compound muscle action potential (CMAP) Massed action potential Direct muscle response – A maximum M-wave (Mmax) is elicited by a supramaximal stimulation of all motor units within the motor unit pool. The Mmax is the methodological control to ensure that the effective stimulus intensity to peripheral nerves is consistent across recording sessions. Anaesthetic effects on reflexes Isoflurane/Sevoflurane – No difference in incidence of ankle clonus or mean clonus score – Greater time to onset in clonus when Sevoflurane is used (1). – Both isoflurane alone and isoflurane plus nitrous oxide decrease H-reflex and F-wave amplitude and F-wave persistence (the number of measurable F waves divided by the number of stimuli). These effects suggest that isoflurane and nitrous oxide decrease motoneuronal excitability in the human spinal cord. This may play an important role in producing surgical immobility (2). – http://www.anesthesiology.org/pt/re/anes/popUpImage.htm;jsessionid=L82KDHLYl2L0TsJVqnCBpn2ZKbHW YvTvVrp80dQF6YJ0JmC8jHQ0!949623904!181195628!8091!-1!1224506890350?an=00000542-19970200000005&id=FF2&type=full – http://www.anesthesiology.org/pt/re/anes/popUpImage.htm;jsessionid=L82KDHLYl2L0TsJVqnCBpn2ZKbHWYvTvVrp80dQF6YJ0JmC8jHQ0!94 9623904!181195628!8091!-1!1224506890350?an=00000542-199702000-00005&id=FF4&type=full – High concentrations of Sevoflurane have been shown to depress tetanic stimulus-induced withdrawal reflexes to a greater extent than that of Propofol. Isoflurane/sevoflurane and ankle clonus (1) Isoflurane & H-reflex (2) Isoflurane and F-wave (2) Nitrous oxide/Isoflurane & F-wave (2) • Propofol - Suppresses the H-reflex at concentrations far lower than those needed for surgical immobility(3). • Ketamine - Does not affect peripheral sensory or motor conduction (4). - Has been shown to effect polysynaptic reflexes but not monosynaptic reflexes when used in the absence of enhanced GABA-mediated inhibitions (5). • Pentobarbital - Does not affect peripheral sensory or motor conduction, but does increase latency of the initial positive component of the somatosensory cortical response and the attenuation of the following negative component. - No significant differences in M-Wave or H-reflex. - Effects are greater and longer in duration than that of Ketamine (4). Reflex Changes in response to SCI/SCT • Spinal Shock – Characterised by complete paralysis, loss of sensation, muscle hypotonia and absent reflexes caudal to the lesion. – In patients with acute SCI, H-reflex and F-wave responses are absent or markedly suppressed early after injury – Similar responses can be observed following perturbation/manipulation of the spine during surgery (6). • Interestingly this study reports that H-reflexes are not affected by depth of anaesthesia, an observation contrary to most literature… Four-phase model of Spinal Shock (7) Phase 1 (0-1 days) Phase 2 (1-3 days) Phase 3 (1-4 weeks) Phase 4 (1-12 months) Areflexia / hyporeflexia Initial reflex return Initial hyperreflexia Final hyperreflexia Loss of descending facilitation Denervation supersensitivity Axon-supported synapse growth Somasupported synapse growth Recovery of reflexes: four phases of spinal shock (7) Reflex 0-1 Day 1-3 Days 1-4 Days 1-12 Months Delayed Planter reflex (S1-2) +++ +++ +/0 +/0 Bulbocavernosus (S3-5) +/0 ++ ++ ++ Anal wink (S4) +/0 ++ ++ ++ Cremasteric (L1-2) +/0 ++ ++ ++ Babinski sign 0 + ++ ++ Flexor withdrawal reflex 0 +/0 ++ +++ Deep tendon reflex (Ankle L5-S2, Knee L3-4) 0 +/0 ++ +++ Tibial H-reflex 0 ++ + +++ Extensor spasm 0 0 0 +++ Interlimb reflexes 0 0 0 +++ Reflex neurogenic bladder (L4-S3) 0 0 0 +++ Autonomic hyper-reflexia 0 0 0 +++ Return of Reflexes (8) • • Plantar response Babinski Return of Reflexes (8) Return of Reflexes (8) References 1) 2) 3) 4) 5) 6) 7) 8) Ewen, A. Cox, R.G. Davies, S.A. Luntley, J.B. Rubin, Y. Fick, G.H. Bevin, B.B. (2005) The ankle clonus test is not a clinically useful measure of spinal cord integrity in children. Can J anesth 52,5,524-529 Zhou, Henry H. MD, PhD; Mehta, Mahesh MD; Leis, A. Arturo MD (1997) Spinal Cord Motoneuron Excitability during Isoflurane and Nitrous Oxide Anaesthesia. Anaesthesiology Volume 86(2) February pp 302-307 Baars,J.H. Dangel, C. Herold, K.F Hadzidiakos, D.A. Rehberg. (2006) Suppression of the human spinal H-reflex by propofol: a quantitative analysis. Acta anaesthesiol scand 50 193200. Goss-Sampson, M.A. Kriss, A. (1991) Effects of pentobarbital and Ketamine-xylazine anaesthesia on somatosensory, brainstem auditory and peripheral sensory-motor responses in the rat. Laboratory Animals 25, 360-366. Lodge, D. Anis, N.A. (1984). Effects of Ketamine and three other anaesthetics on the spinal reflexes in the cat. Br J Anaesth. 56, 1143-1151. Leiss, A.A. Zhou, H.H. Mehta,M. Harkey, H.L. Paske. (1996) Behaviour of the H-reflex in humans following mechanical injury to rostral spinal cord. Ditunno, J.F. Little, Tessler, J.W. Burns, A.S. (2004) Spinal shock revisited: a Four phase model. Spinal cord. 42. 383-395. Kyo, H-Y. Ditunno, JF. Graziani, V. Little, J.W. (1999) The pattern of reflex recovery during spinal shock. Spinal Cord 37, 402-409. Thanks for listening Questions ???