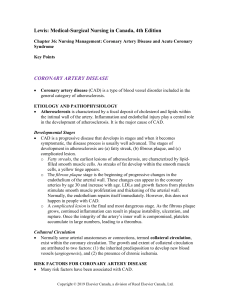
Perfusion & Coronary Artery Disease
advertisement

Coronary Artery Disease, High Cholesterol, Stable Angina, Unstable Angina (ACS) Brunner, ch 27, pp. 729-741 Coronary Artery Disease AKA: CAD Ischemic Heart Disease Coronary Heart Disease (CHD) Arteriosclerotic Heart Disease (AHD) Arteriosclerotic Cardiovascular Disease (ASCVD) Pathophysiology of CAD Abnormal accumulation of lipids and fibrous tissues causes an atheroma (plaque). Progresses from fatty streak to fibrous plaque, to ulcerated lesion with thrombus formation. Vessel wall becomes inflamed and damaged, attracting platelets and WBCs, becoming a complicated lesion. Pathophysiology cont’d Atheroma protrudes into lumen of vessel, obstructing blood flow (Figure 27-1, p. 730) Obstruction of blood flow causes lack of oxygen (ischemia) to the area perfused by the affected artery causing pain (angina). If collateral circulation does not develop, permanent damage can occur. Development of Collateral Circulation Non-modifiable Risk Factors for CAD Chart 27-1, 731: Age: (M > 45; F > 55) Gender: (M > F until menopause) Family hx: esp first degree relative Race: higher in African Americans Leading cause of death in both genders and in all races and ethnic groups. Modifiable Risk Factors for CAD— Metabolic Syndrome Dyslipidemia—high LDL;low HDL (F<50; M<40); triglycerides>150 Proinflammatory state—C-reactive protein (CRP) 1 mg/L; 3 is hi-risk Hypertension >130/85 Prothrombotic state (high fibrinogen) Insulin resistance (FBS > 100) Central obesity (waist: F: w>35; M: w>40) *Diagnosis = 3/6 Modifiable Risk Factors cont’d Elevated homocysteine >2.3 mg/L damages endothelial lining Tobacco use; twice as bad in women. Damages endothelial lining, increases catecholamines, carbon monoxide replaces O2 in blood Physical inactivity Hyperlipidemia; Atherogenic diet HTN: 120/80 prehypertensive; 140/90 Stage I Diabetes Obesity Metabolic syndrome Pathophysiology of High Cholesterol Metabolism of fats is important contributor to development of HD Fats are encased in lipoproteins that allow them to circulate Lipoproteins are categorized by their protein content: more protein = more dense High fat meal broken down into chylomicrons processed into lipoproteins LDL portion adheres to intimal wall See Figure 27-4, p. 733 Cholesterol Norms Total cholesterol <200 HDL >60—good cholesterol LDL <100 (<70 in hi-risk pts)—bad cholesterol Triglycerides <150 (high sugar intake can affect results) LDL is targeted for therapy Angina: Chronic, Stable Predictable and manageable Caused from CAD, but also anything that could increase the heart’s oxygen demand: Exertion Emotion Eating big meal Tobacco use Stimulants (cocaine, thyrotoxicosis) Irregular, fast heart rhythms Anemia Manifestations of Chronic Stable Angina Caused by partial occlusion with atheroma Squeezing, tightness, heaviness Epigastric, midsternal, or retrosternal pain May radiate to neck, jaw, arm, back May have nausea, diaphoresis, dizziness Chronic Stable Angina cont’d Usually lasts 3-5 minutes Responds to rest and nitrate therapy Same each time Usually has pattern of activity-pain/rest-relief T-wave inversion with episodes Women and individuals with diabetes are frequently atypical with GI sx, fatigue, and back pain Angina: Unstable (Preinfarction angina) Blood flow is reduced, but not fully occluded. Ischemia with or without significant injury to myocardial tissue. Coronary vessel is damaged and inflamed. Coronary artery spasms may occur (Prinzmetal’s or Variant angina). Pain is unpredictable. Reversible ST elevation Although if not treated can lead to an MI, it is not an MI—that is death to the myocardial tissue (covered in NUR 213) Silent Angina ECG changes with stress test show ischemia but no pain is felt Can have atypical symptoms such as nausea, diaphoresis, dizziness, indigestion which are usually ignored or blamed on something else More common in people with diabetes, women, and elderly Manifestations of Angina Substernal, retrosternal, or epigastric pain and /or choking sensation caused from partial occlusion and/or coronary artery spasm. exacerbated by cold, exertion, heavy meal, stress. Relieved by NTG Can radiate to neck, jaw, shoulders, inner left arm, epigastric area Apprehension, fear of impending doom, weakness, dizziness, N/V With unstable, pain is more severe and prolonged, increasing in frequency and severity, and may occur at rest. Unrelieved by NTG Manifestations cont’d May last 10-20 minutes Dyspnea, tachycardia, pulsus alternans, pulse deficit Gallop rhythm, murmur Hyper or hypotension Cool, pale skin ECG changes—arrhythmias, ST depression, T wave inversion ECG Changes with Angina Manifestations cont’d Negative serum cardiac markers Positive stress test and thallium scans (creates chest pain) CXR may show cardiac enlargement or pulmonary congestion Echo may show abnormal wall motion Positive coronary angiography (shows occlusion) Medical Management Goal is to improve oxygen to the myocardium by decreasing demand and providing supplementation Medication therapy (Table 27-3, p. 737) and morphine Changing modifiable risk factors In some instances, interventional therapies are needed (PCI, stents, arthrectomy, CABG) Nursing Diagnoses for CAD Acute Pain Ineffective tissue perfusion (cardiac/peripheral) Risk for imbalanced fluid volume Fear/Anxiety Imbalanced nutrition Ineffective health maintenance Ineffective therapeutic regimen mgmt Ineffective coping Deficient knowledge Nursing Management of CAD: Health Promotion Diet—low sodium, low fat. Mediterranean diet is promoted. Vegetarian diets are good. High fiber is helpful. Lose weight Exercise—150” of moderate activity/wk; 75” of intense Stop tobacco products Monitor and control blood sugar Monitor BP and lipid levels Reduce stress Nursing Management cont’d Monitor effects of and provide education for med therapy if indicated: Antilipidemics Antiplatelets Antidiabetics Antihypertensives Antianginals Percutaneous Revascularization Revascularization cont’d Patient Education S&S of CP Avoid activities that cause CP Avoid OTC meds that raise P and BP If pain occurs, stop activity and take NTG If no relief, BP gets too low, or weakness, dizziness, or syncopy occurs, call 911 Med therapy (self adm, storage, etc.) Preventative NTG tx Control modifiable risk factors