Bladder
advertisement

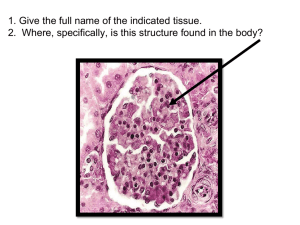
Evaluation of the Urologic Patient Maryam Taheri, Urologist Shohada-e Tajrish Hospital Urology Nephrology Research Center Shaheed Beheshti University of Medical Sciences • Urinary System – Kidneys – Ureters – Bladder – Urethra kidneys - Typically each kidney weighs 150 g in the male and 135 g in the female. - The kidneys generally measure 10 to 12 cm vertically, 5 to 7 cm transversely, and 3 cm in the anteroposterior dimension. - Because of compression by the liver, the right kidney tends to be somewhat shorter and wider. Also the right kidney sits 1 to 2 cm lower than the left. - Generally, the right kidney resides in the space between the top of the first lumbar vertebra to the bottom of the third lumbar vertebra. The left kidney occupies a more superior space from the body of the 12th thoracic vertebral body to the 3rd lumbar vertebra. • Internal anatomy of the Kidneys – – – – – – – Renal arteries Renal capsule Hilum Cortex Medulla(Pyramid) Calyces Collecting tubules Ureters - Urine, which is formed within the nephrons, flow into the ureter, a long narrow muscular tube which starts at the lower portion of the renal pelvis and extends down to the bladder. - Each ureter has 3 narrowed areas along its length. - These junctions cause an angling of the ureter that prevents reflux (backwards movement)t of urine up toward the kidney. - Also these three sites of ureteral narrowing are clinically significant because they are common locations for urinary calculi to lodge during passage. Bladder - The urinary bladder is a mascular, hollow sac located just behind the symphysis pubis. - Normal bladder capacity if 300-600 ml of urine. But an overdistended bladder can hold in excess of 1500ml of urine. When we insert a Foley, it is important to take note of the amount of urine that is drained as the distended bladder is emptied. Note: When a patient loses too much fluid too rapidly, his/her hemodynamics can’t tolerate the rapid change (release of pressure on abdominal vessels) and he/she may develop hypovolemic shock. This can be prevented by temporarily clamping the Foley drainage tubing after 750 ml of urine has entered the drainage bag. - In the neck of the bladder is an area of smooth muscle that makes up the internal urinary sphincter which is under involuntary control. Urethra -The urethra carries the urine from the bladder and expels it from the body. -On average, the female urethra traverses 4 cm from the bladder neck to the vaginal vestibule. -The male urethra extends from the internal urethral orifice in the urinary bladder to the external urethral orifice at the end of the penis. Its length varies from 17.5 to 20 cm.; and it is divided into four portions: prostatic, membranous, bulbar and penile urethra. - Within the urethra is the external urinary sphincter, which is the only structure within the urinary system that is under voluntary control. Physical Exam General Observations The visual inspection of the patient provides a general overview. - The skin should be inspected for evidence of jaundice or pallor. - The nutritional status of the patient should be noted. Cachexia is a frequent sign of malignancy, and obesity may be a sign of underlying endocrinologic abnormalities. In this instance, one should search for the presence of truncal obesity, a “buffalo hump,” and abdominal skin striae, which are stigmata of hyperadrenocorticism. In contrast, debility and hyperpigmentation may be signs of hypoadrenocorticism. - Gynecomastia may be a sign of endocrinologic disease and a possible indicator of alcoholism or previous hormonal therapy for prostate cancer. -Edema of the genitalia and lower extremities may be associated with cardiac decompensation, renal failure, nephrotic syndrome, or pelvic and/or retroperitoneal lymphatic obstruction. - Supraclavicular lymphadenopathy may be seen with any GU neoplasm, most commonly prostate and testis cancer; inguinal lymphadenopathy may occur secondary to carcinoma of the penis or urethra. Physical exam of urinary system • • A complete and thorough physical examination is an essential component of the evaluation of patients who present with urologic disease. When performing a physical assessment of a patient, urological problems may be detected by examination of the abdomen, suprapubic region, genitalia and lower back, as well as the lower extremities. Landmarks for physical assessment of the urinary system on abdomen and suprapubic: - Rectus Abdominis Muscles - Longitudinal muscles extending from the Pubis to the ribs on either side of the midline, guides the location kidney palpation. - Symphysis Pubis - Joint formed by the union of two pubic bones at the midline which bladder is cradled under this structure. The kidneys are fist-sized organs located high in the retroperitoneum bilaterally. In the adult, the kidneys are normally difficult to palpate because of their position under the diaphragm and ribs with abundant musculature both anteriorly and posteriorly. In children and thin women, it may be possible to palpate the lower pole of the right kidney with deep inspiration. However, it is usually not possible to palpate either kidney in men, and the left kidney is almost always impalpable unless it is abnormally enlarged. Auscultation of the right and left renal arteries: Subcostal bruit suggests renal artery stenosis. Fig. Palpating the left kidney. Costovertebral Angle - Area on the lower back formed by the vertebral column and downward curve of the last posterior rib. Fig. Blunt percussion over the left costovertebral angle Fig. Palpating the bladder. * A normal bladder in the adult cannot be palpated or percussed until there is at least 150 mL of urine in it. At a volume of about 500 mL, the distended bladder becomes visible in thin patients as a lower midline abdominal mass. Percussion is better than palpation for diagnosing a distended bladder. The examiner begins by percussing immediately above the symphysis pubis and continuing cephalad until there is a change in pitch from dull to resonant. Alternatively, it may be possible in thin patients and in children to palpate the bladder by lifting the lumbar spine with one hand and pressing the other hand into the midline of the lower abdomen. A careful bimanual examination, best done with the patient under anesthesia, is invaluable in assessing the regional extent of a bladder tumor or other pelvic mass. The bladder is palpated between the abdomen and the vagina in the female or the rectum in the male. In addition to defining areas of induration, the bimanual examination allows the examiner to assess the mobility of the bladder; such information cannot be obtained by radiologic techniques such as CT and MRI, which convey static images. Bimanual examination of the bladder in the female. Bimanual examination of the bladder in the male. Digital rectal examination (DRE) - DRE should be performed in every male after age 40 years and in men of any age who present for urologic evaluation. -Prostate cancer is the second most common cause of male cancer deaths after age 55 years and the most common cause of cancer deaths in men older than 70 years. Many prostate cancers can be detected in an early curable stage by DRE, and about 25% of colorectal cancers can be detected by DRE in combination with a stool guaiac test. -DRE should be performed at the end of the physical examination. It is done best with the patient standing and bent over the examining table or with the patient in the knee-chest position. -The gloved, lubricated index finger is then inserted gently into the anus. Only one phalanx should be inserted initially to give the anus time to relax and to easily accommodate the finger. Estimation of anal sphincter tone is of great importance; a flaccid or spastic anal sphincter suggests similar changes in the urinary sphincter and may be a clue to the diagnosis of neurogenic disease. If the physician waits only a few seconds, the anal sphincter will normally relax to the degree that the finger can be advanced to the knuckle without causing pain. The index finger then sweeps over the prostate; the entire posterior surface of the gland can usually be examined if the patient is in the proper position. Normally, the prostate is about the size of a chestnut and has a consistency similar to that of the contracted thenar eminence of the thumb (with the thumb opposed to the little finger). The index finger is extended as far as possible into the rectum, and the entire circumference is examined to detect an early rectal carcinoma. Vaginal Exam Pelvic organ prolapse is a downward descent of female pelvic organs, including the bladder, uterus and the small or large bowel, resulting in protrusion of the vagina, uterus, or both. Prolapse development can be attributed to several factors, including; vaginal delivery, hysterectomy, chronic straining, obesity, normal aging and abnormalities of connective tissue . -Four main types of pelvic organ prolapse can occur: * When the protrusion involves the front (anterior wall) of the vagina and bladder, the condition is called a cystocele or "dropped bladder." * When the back (posterior wall) of the vagina and rectum are involved, the condition is called a rectocele. * When the upper portion of the vaginal wall (the peritoneum cul-de-sac) and small bowel are involved the condition is called an enterocele. *When the uterus descends downward, the presentation is called uterine prolapse. History( Common urologic problems) The medical history is the cornerstone of the evaluation of the urologic patient, and a well-taken history will frequently elucidate the probable diagnosis. Fever and Chills Fever and chills may occur with infection anywhere in the GU tract but are most commonly observed in patients with pyelonephritis, prostatitis, or epididymitis. When associated with urinary obstruction, fever and chills may portend septicemia and necessitate emergency treatment to relieve obstruction. Pain Pain arising from the GU tract may be quite severe and is usually associated with either urinary tract obstruction or inflammation. Urinary calculi cause severe pain when they obstruct the upper urinary tract. Conversely, large, nonobstructing stones may be totally asymptomatic. Hematuria Hematuria is the presence of blood in the urine; greater than three red blood cells per high-power microscopic field (HPF) is significant. Patients with gross hematuria are usually frightened by the sudden onset of blood in the urine and frequently present to the emergency department for evaluation, fearing that they may be bleeding excessively. Hematuria of any degree should never be ignored and, in adults, should be regarded as a symptom of urologic malignancy until proved otherwise. Irritative urinary Symptoms; 1. Frequency: is one of the most common urologic symptoms. The normal adult voids five or six times per day, with a volume of approximately 300 mL with each void. Urinary frequency is due to either increased urinary output (polyuria) or decreased bladder capacity. If voiding is noted to occur in large amounts frequently, the patient has polyuria and should be evaluated for diabetes mellitus, diabetes insipidus, or excessive fluid ingestion. Causes of decreased bladder capacity include bladder outlet obstruction with decreased compliance, increased residual urine, and/or decreased functional capacity due to irritation, neurogenic bladder with increased sensitivity and decreased compliance, pressure from extrinsic sources, or anxiety. 2. Nocturia: is nocturnal frequency. Normally, adults arise no more than twice at night to void. As with frequency, nocturia may be secondary to increased urine output or decreased bladder capacity. * Frequency during the day without nocturia is usually of psychogenic origin and related to anxiety. Nocturia without frequency may occur in the patient with congestive heart failure and peripheral edema in whom the intravascular volume and urine output increase when the patient is supine. 3. Dysuria: is painful urination that is usually caused by inflammation. This pain is usually not felt over the bladder but is commonly referred to the urethral meatus. Pain occurring at the start of urination may indicate urethral pathology, whereas pain occurring at the end of micturition (strangury) is usually of bladder origin. Dysuria is frequently accompanied by frequency and urgency. Obstructive Urinary Symptoms; 1. Decreased force of urination: is usually secondary to bladder outlet obstruction and commonly results from benign prostatic hyperplasia (BPH) or a urethral stricture. In fact, except for severe degrees of obstruction, most patients are unaware of a change in the force and caliber of their urinary stream. These changes usually occur gradually and go generally unrecognized by most patients. 2. Urinary hesitancy: refers to a delay in the start of micturition. Normally, urination begins within a second after relaxing the urinary sphincter, but it may be delayed in men with bladder outlet obstruction. 3. Intermittency: refers to involuntary start-stopping of the urinary stream. It most commonly results from prostatic obstruction with intermittent occlusion of the urinary stream by the lateral prostatic lobes. 4. Postvoid dribbling: refers to the terminal release of drops of urine at the end of micturition. This is secondary to a small amount of residual urine in either the bulbar or the prostatic urethra that is normally “milked back” into the bladder at the end of micturition. In men with bladder outlet obstruction, this urine escapes into the bulbar urethra and leaks out at the end of micturition. 5. Straining: refers to the use of abdominal musculature to urinate. Normally, it is unnecessary for a man to perform a Valsalva maneuver except at the end of urination. Increased straining during micturition is a symptom of bladder outlet obstruction. Urinary Incontinence Urinary incontinence is the involuntary loss of urine. A careful history of the incontinent patient will often determine the etiology. Urinary incontinence can be subdivided into four categories. 1. Continuous Incontinence: Continuous incontinence is most commonly due to a urinary tract fistula that bypasses the urethral sphincter. 2. Stress Incontinence: Stress incontinence refers to the sudden leakage of urine with coughing, sneezing, exercise, or other activities that increase intra-abdominal pressure. During these activities, intra-abdominal pressure rises transiently above urethral resistance, resulting in a sudden, usually small amount of urinary leakage. Stress incontinence is most common in women after childbearing or menopause and is related to a loss of anterior vaginal support and weakening of pelvic tissues. Stress incontinence is also observed in men after prostatic surgery, most commonly radical prostatectomy, in which there may be injury to the external urethral sphincter. 3. Urgency Incontinence. Urgency incontinence is the precipitous loss of urine preceded by a strong urge to void. This symptom is commonly observed in patients with cystitis, neurogenic bladder, and advanced bladder outlet obstruction with secondary loss of bladder compliance. 4. Overflow Urinary Incontinence. Overflow urinary incontinence, often called paradoxical incontinence, is secondary to advanced urinary retention and high residual urine volumes. In these patients, the bladder is chronically distended and never empties completely. Urine may dribble out in small amounts as the bladder overflows. Enuresis Enuresis refers to urinary incontinence that occurs during sleep. It occurs normally in children up to 3 years of age but persists in about 15% of children at age 5 and about 1% of children at age 15. Enuresis must be distinguished from continuous incontinence, which occurs in the day and night and which, in a young girl, usually indicates the presence of an ectopic ureter. All children older than age 6 years with enuresis should undergo a urologic evaluation, although the vast majority will be found to have no significant urologic abnormality. Neurogenic Bladder Neurogenic bladder is a dysfunction that results from interference with the normal nerve pathways associated with urination. Normal bladder function is dependent on the nerves that sense the fullness of the bladder (sensory nerves) and on those that trigger the muscle movements that either empty it or retain urine (motor nerves). The reflex to urinate is triggered when the bladder fills to 300-500 ml. The bladder is then emptied when the contraction of the bladder wall muscles forces urine out through the urethra. The bladder, internal sphincters, and external sphincters may all be affected by nerve disorders that create abnormalities in bladder function. There are two categories of neurogenic bladder dysfunction: overactive (spastic or hyper-reflexive) and underactive (flaccid or hypotonic) An overactive neurogenic bladder is characterized by uncontrolled, frequent expulsion of urine from the bladder. There is reduced bladder capacity and incomplete emptying of urine. An underactive neurogenic bladder has a capacity that is extremely large (up to 2000 ml). Due to a loss of the sensation of bladder filling, the bladder does not contract forcefully, and small amounts of urine dribble from the urethra as the bladder pressure reaches a breakthrough point. There are numerous causes for neurogenic bladder dysfunction such as: stroke, Parkinson's disease, surgery on the spinal cord, sacral spinal tumors, congenital defects or a complication of various diseases, such as syphilis, diabetes mellitus, or polio.