Lt Ge
advertisement

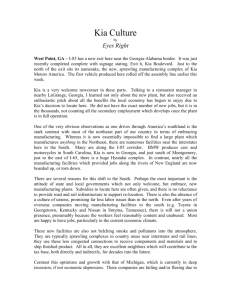
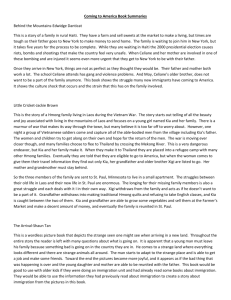
How Did We Get Where We Are in Combat Casualty Care Paul K. Carlton Jr., MD, FACS. LtGen, USAF, MC, Ret. Professor of Surgery, Texas A&M HSC, Ret. 29 May 2015 Begin with the end in mind FINISH Combat Casualty Statistics From Stansbury, Holcomb, Champion, Bellamy, 2005 Best survival we have ever had in the history of war! 25 20 15 WWII Vietnam OIF/OEF 10 5 0 %KIA %DOW WIA = Wounded in Action (WIA =RTD+ Evacuated+ DOW) RTD = Returned to Duty in 72 hrs Evacuated = Not RTD in 72 hrs DOW = Died of Wounds KIA = Killed in Action CFR = Case Fatality Rate %CFR • %KIA = KIA / KIA + (WIA - RTD) • %DOW = DOW / WIA – RTD • %CFR = KIA +DOW / KIA + WIA Press On Nothing in the World can take the place of persistence. Talent will not; nothing is more common than An Aviators perspective! unsuccessful men with talent. Genius will not; unrewarded genius is almost a proverb. Education will not; the world is full of educated derelicts. Persistence and determination alone are omnipotent! Calvin Coolidge 1929 Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Combat Casualty Care 1. No one would resist trying to improve the survival of our war wounded! 2. Everyone is trying to do that! 3. WRONG! 4. Any change upsets the status quo, so will be resisted tremendously! Why is Change So Hard Positives = Neutral = Negatives= Positives: Interest - excitement Pleasure - joy Two One Six Startle Negatives: Anger Fear Shame Because our brains are hard wired to resist change! Distress Disgust Dis-smell Source: Silvan Thompkins How did we get where we are today in combat casualty care? Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Historical Review of Casualty Care 1.This topic is basically the history of medicine as we know it today! 2.Medicine had no scientific basis until Pasteur made his observations on cowpox and smallpox in 1796! 3.Modern, scientific medicine follows the development of necessity during wartime activities! 4.Medical facilities did not really develop in this country until after WW2, when soldiers saw their value. Wounding Contrary to what we have all witnessed on countless TV and Movie shows, no one dies right away when struck with a projectile! They die or stop fighting when the brain no longer receives oxygen or the brain is dis-associated from the body! This can be very quickly, if the head is blown off, or take days to weeks, depending on where the projectile hits the body. This is a very difficult concept to get across to our law enforcement community, just because someone has a lethal wound does not mean they stop resisting! It is very important to you as warfighters if you have to protect your colleagues! Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Antiquity 1. Wounding was by low velocity missiles of many typesswords, spears, arrows, primitive rifles and bullets. 2. Medical care was typical of the times- poultices, bleedings, amputations. 3. No formal medical school, just an apprenticeship. 4. Mortality rates ran in the 60% or greater realm. 5. Questions from ancient India, who showed cross arm flaps to reconstruct noses in drawings from 500 BC. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Casualty Care -Prior to Larrey •Casualties lay in the field •If won – care given •If lost – executed or left to die on the battlefield and looted as spoils of war Dominique-Jean Larrey •1786 – Completed medical studies •1792 – War breaks out •1797 – designed first “flying ambulances” for evacuation - “flying ambulances” were horse drawn wagons to collect and carry wounded from battlefield to hospital - consisted of transport, medical supplies and support personnel •1815- spared by the Duke of Wellington because he took care of all casualties at Battle of Waterloo Napoleon's Surgeon “Flying Ambulance” Hence the name of the first modular team was “Flying Ambulance Surgical Trauma Team” 1984- USAFE Same concept Napoleon's Surgeon 1. Wounding was by low velocity missiles of many types, swords, spears, arrows, primitive rifles and bullets. 2. Medical care was typical of the times- poultices, bleedings, amputations. 3. Mortality rates ran in the 60% or greater realm. 4. For the first time, the casualty did not lay in the field to wait to see who won, they were moved to receive medical care. 5. This practice saved Larrey’s life after the Battle of Waterloocustom was to execute entire General Staff. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Civil War and anesthesia. The discovery of ether in 1846 was a landmark in the surgical field, now you could operate painlessly! First abdominal surgery in the USA was in 1846, an ovarian tumor was removed and the patient survived. The first survivor of a pelvic gunshot would was Col Joshua Chamberlain, of Gettysburg fame. He was from the 20th Maine and held the left flank of the Union lines at that battle. At the Battle of the Wilderness in 1864 he was shot in the pelvis and categorized as expectant. No one had ever survived such a wound. Civil War and anesthesia. The discovery of ether in 1846 was a landmark in the surgical field, now you could operate painlessly! First abdominal surgery in the USA was in 1846, an ovarian tumor was removed and the patient survived. The first survivor of a pelvic gunshot would was Col Joshua Chamberlain, of Gettysburg fame. He was from the 20th Maine and held the left flank of the Union lines at that battle. At the Battle of the Wilderness in 1864 he was shot in the pelvis and categorized as expectant. No one had ever survived such a wound. His brother pleaded his case and he underwent an operation to suture his bladder injury under ether anesthesia. The bladder always ruptured when it filled after suturing. His bladder was decompressed with a rigid catheter and he survived to go on and be a University President and Governor of Maine. Civil War and anesthesia. The discovery of ether in 1846 was a landmark in the surgical field, now you could operate painlessly! The first survivor of a pelvic gunshot would was Col Joshua Chamberlain, of Gettysburg fame. He was from the 20th Maine and held the left flank of the Union lines at that battle. At the Battle of the Wilderness in 1864 he was shot in the pelvis and categorized as expectant. No one had ever survived such a wound. His surgeon was willing to think differently than conventional wisdom His brother pleaded his case and he underwent an operation dictated! to suture his bladder injury under ether anesthesia. War leads to ruptured many innovations in suturing. medical The bladder always when it filled after His bladder with a rigid catheter and care, aswas it isdecompressed doing now! he survived to go on and be a University President and Governor of Maine. “In times of change the learners will inherit the world… while the learned will find themselves beautifully equipped to deal with a world that no longer exists” Eric Hoffer Civil War and anesthesia. 1. Wounding was still by low velocity missiles of many types, swords, spears, arrows, primitive rifles and bullets. 2. Grape shot by cannon began to move into high velocity wounding. 3. Medical care was typical of the times- poultices, bleedings, amputations, but anesthesia, when available, made it less painful! 4. Mortality rates came down to around 50% using hot cautery for amputations. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Boer War 1. South Africa between Dutch and British armies and their surrogates. 2. First high velocity wounds prompted the Dutch to charge the British with using “exploding bullets!” 3. The high velocity bullets imparted their energy into the tissue and created a large exit wound with a small entry wound. 4. Mortality rates remained at the 50% level despite this high velocity wound due to better medical care. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity World War One 1. High velocity wounds were the norm. 2. Artillery caused a large number of wounds. 3. Horror of trench warfare created a large number of gas gangrene cases. 4. Wounding to medical care was measured in hours. 5. Chemical warfare created a new type of casualty. 6. Mortality rates remained in the 50% range because medical care was more sophisticated despite more horrific wounding. World War One We sent the major medical facilities to war! Mayo Clinic, Harvard, Hopkins, Cincinnati, Yale, etc. all went to war as an integral team of University people! Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity World War Two We sent the major medical facilities to war! Mayo Clinic, Harvard, Hopkins, Cincinnati, Yale, etc. all went to war as an integral team of University people! They brought modern medical and surgical techniques to the war for the first time! This time they had antibiotics and more sophisticated surgical care. World War Two 1. 2. 3. 4. Modern surgical technique were used. Antibiotics were available. Medical planning was integral. Wounding to medical care was now 6-12 hours. 5. Vascular repairs became available instead of ligation. 6. Mortality rates came down to around 30% despite high velocity wounding! Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Korea 1. Rotary wing evacuation lowered time to surgery from wounding to hours. 2. Antibiotics. 3. Forward Surgical hospitals. 4. Evacuation was rapid. 5. Mass casualty management. 6. Mortality rate came down to around 25%. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Vietnam 1. 2. 3. 4. 5. 6. Rotary wing evacuation. Antibiotics. Good surgical techniques. Echelons of care. Mortality remained high at 24%. Breakdown the mortality though showed us that we only had a 2.8% in hospital mortality rate in country, if the casualty got to us alive. 17% KIA group were those who never saw a physician before dying. Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Current Activity What changed in medical care from 1970-2000: 1. Modern Ventilator care. 2. Golden Hour in Trauma. 3. Platinum 10 minutes in trauma care. 4. Salvage surgery. 5. Transportation platforms. 6. Level One Trauma Centers. 7. Organized system of trauma care. 8. Designated Trauma Surgeon. Current Activity What changed in medical care from 1970-2000: 1. Modern Ventilator care. 2. Golden Hour in Trauma. 3. Platinum 10 minutes in trauma care. 4. Salvage surgery. 5. Transportation platforms. 6. Level One Trauma Centers. 7. Organized system of trauma care. 8. Designated Trauma Surgeon. We applied all of these activities to our military teams in the combat zone! Military Medicine Measure of Merit for Military Medicine Soldiers, sailors, airmen and marines at work doing their jobs- protected against environmental hazards and if injured, receiving the very best possible care! 1. Public Health 2. Casualty Management Public Health Best job we have ever done in the history of war Major improvement over GW I in water, food, sanitation, etc… Prior to WW 2, we always lost more to public health than to combat! Casualty Management in Global War on Terrorism 2001-2015 “Unprecedented” Survival Rates • Soldier survival rates in Iraq highest in U.S. war history – 1/9 soldiers injured died from wounds – Wounds critical as past wars • Several advances – Improved body armor technology (kevlar helmets and vests) – On-site treatment by mobile surgical units • “The average time from battlefield to arrival in the United States is now less than four days. In Vietnam, it was 45 days.” -- Dr. Atul Gawande Navy Times, Jan 05 Addressed All Areas as Joint Team 2004 Led to highest survival in history of war – WWII Vietnam/GWI OIF 70% 90% 76% Result of “Heretical” Thinking NEJM 9 Dec 04 What does 90% Mean? 11,000+ Injured in Iraq GW2 90% 9,900 Vietnam/GW1 76% 1,540 8,360 Extra alive because of new thinking! Source: New England Journal of Medicine 9 Dec 2004 What does 90% Mean? 11,000+ Injured in Iraqupdated Number is now to GW2 9,900because over 6,00090% extra alive we were willing to 8,360 think Vietnam/GW1 76% differently! 1,540 Extra alive because of new thinking! Source: New England Journal of Medicine 9 Dec 2004 “In times of change the learners will inherit the world… while the learned will find themselves beautifully equipped to deal with a world that no longer exists” Eric Hoffer Nomenclature is Important KIA= Killed in Action, means died before saw a physician. DOW= Died of Wounds, means died after saw a physician. CFR= Case Fatality Rate, means of the total injured, how many die. Combat Casualty Statistics From Stansbury, Holcomb, Champion, Bellamy, 2005 25 Best we have ever done! 20 15 WWII Vietnam OIF/OEF 10 5 0 %KIA %DOW %CFR WIA = Wounded in Action (WIA =RTD+ Evacuated+ DOW) RTD = Returned to Duty in 72 hrs • %KIA = KIA / KIA + (WIA - RTD) Evacuated = Not RTD in 72 hrs • %DOW = DOW / WIA – RTD DOW = Died of Wounds KIA = Killed in Action • %CFR = KIA +DOW / KIA + WIA CFR = Case Fatality Rate Nomenclature is Important Hospital died of wounds rate was 2.8% in Vietnam. Our current hospital died of wounds rate is 1% at a Level III facility. This is only a 1.8% improvement! The big advances were on out of hospital care and prevention- 5%! That is where we focused! Improvement Most of the improvement is out of the KIA group. Our DOW rates actually went up! We made a conscious decision to go after the KIA group from Vietnam by putting medical care much closer to the battle field, knowing that our DOW rate would actually go up! Our postulate was that it would improve the overall survival rates, the Combined Case Fatality Rate. Combat Casualty Statistics From Stansbury, Holcomb, Champion, Bellamy, 2005 25 Best we have ever done! 20 15 WWII Vietnam OIF/OEF 10 5 0 %KIA %DOW %CFR WIA = Wounded in Action (WIA =RTD+ Evacuated+ DOW) RTD = Returned to Duty in 72 hrs • %KIA = KIA / KIA + (WIA - RTD) Evacuated = Not RTD in 72 hrs • %DOW = DOW / WIA – RTD DOW = Died of Wounds KIA = Killed in Action • %CFR = KIA +DOW / KIA + WIA CFR = Case Fatality Rate Major Variables •Better body armor that protects vital area •Stabilization of injury with far forward surgery •Critical care in the air •Family support - No One “gives up!” Apples to Apples Comparison Data from ISR--Case Fatality Rates 8.8% IF/EF 16.5% VN/GWI 22.8% WWII Stansbury, Holcomb, Champion, Bellamy July 2005 This segment will focus on how we got where we are today and look to the future 1983- After Action report from Marine Barracks Bombing Examined how we dealt with injured globally: Vietnam •Comprehensive care in country •Close by referral to Japan or Philipines •45 days to reach USA 1983- After Action report from Marine Barracks Bombing Examined how we dealt with injured globally: Vietnam •Comprehensive care in country •Close by referral to Japan or Philipines •45 days to reach USA This was a young team- Dan Locker, Win Mabry, Craig Hinman, Dave Welling, Geoff Wiedeman, PK Carlton, John Lockett, and many others- mostly LtCols in rank. We were laughed at for our audacity for thinking we could change a big system like the Air Force! 1983- After Action report from Marine Barracks Bombing Examined how we dealt with injured globally: Vietnam •Comprehensive care in country •Close by referral to Japan or Philipines •45 days to reach USA This was a young team- Dan Locker, Win Mabry, Craig Hinman, Dave Welling, Geoff Wiedeman, PK Carlton, John Lockett, and many others- mostly LtCols in rank. We were laughed at for our audacity for thinking we could change a big system like the Air Force! Our response was to say it was “our Air Force” and we had an obligation to make it better! 1983- After Action report from Grenada •Grenada invasion •LtGen Jim Peake, Ret. did much the same thing after Grenada 1983 •Parallel development that intertwined repeatedly USAFUSA-USN-USMC •I know the Air Force side so will relate that, understand other services participated in this improvement as well! 1983- After Action report from Marine Barracks Bombing Is that correct? 1983- After Action report from Marine Barracks Bombing Is that correct? Is there a better way? 1983- After Action report from Marine Barracks Bombing Is that correct? Is there a better way? Is that what you want for your son or daughter? 1983- After Action report from Marine Barracks Bombing Is that correct? Is there a better way? Is that what you want for your son or daughter? Could you look a grieving parent or spouse in the eye and say “no one could have done better!” Post Injury Phases of Illness 1983 Salvageable Mortality From: Blood Loss Infection Respiratory Failure Injury Days Rehabilitation Recovery Weeks Months Post Injury Phases of Illness 1983 Salvageable Mortality From: Salvage Surgery in 1st hour Blood Loss Secondary Surgery Definitive Care Infection Respiratory Failure Rehabilitation Recovery Injury Days Critical Care in the Air Months Weeks Critical Care in the Air Truisms! Right is right, even if everyone is against it, and wrong is wrong, even if everyone is for it.” William Penn, British statesman and philosopher This thinking and planning paid dividends in 1st hour of deployment in October 2001 Recent Support of War Effort: Operation Enduring Freedom--Oct 2001 Injury Scenario: Military and Civilian Care Comparison Elapsed Time Post Injury 1 2 3 4 Care Received Emergency Surgery 25 min Damage Control Military Setting MFST personnel 6* hours Emergency Surgery CCATT enroute Further Stabilization /surgical team at AmSurg Center 24* hours CCATT enroute /surgical team in Military Hospital Setting 48*+ hours Definitive Surgical Care Definitive Surgical Care Military Medical Center Civilian Setting Level 1 Trauma Center Level 1 Trauma Center Level 1 Trauma Center Level 1 Trauma Center/ Tertiary Hospital *Times and locations are estimated This has now become the norm according to surgeons at Landstuhl, Germany. Team work has never been better! Warren Dorlac 5 August 2005 Advantage •Smaller footprints in theater •Address needs as a threat become apparent •“Meet Golden Hour” •Home quickly with full resources •Family present! Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! “In times of change the learners will inherit the world… while the learned will find themselves beautifully equipped to deal with a world that no longer exists” Eric Hoffer Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Critical Care in the Air CCATT “Their Story” Heretical Thinking! Critical Care in the Air CCATT Continuous En Route Care Historical Route From Injury to Definitive Care STRATEGIC EVAC - Evac Policy 15 Days TACTICAL EVAC - Evac Policy 7 Days Definitive Care “Level 4” CASUALTY EVAC - Evac Policy 1 Day In Theater Hospital “Level 3” Field Hospital “Level 2” Battalion Aid Station “Level 1” Out of “ME” and into “WE” JOINT TEAM Continuous En Route Care Current Route from Injury to Definitive Care CASEVAC 1 Hour TACTICAL EVAC 24 Hours BAS Level 1 STRATEGIC EVAC 48-72 Hours Forward Surgical teams Level 2 Combat Support Hospital, EMEDS, Fleet Hospital Level 3 Surgical Capability Definitive Care Level 4 CCATT History •Conceptualized 1983- rejected by AE- “Like trying to catheterize a running race horse! Sit down, shut up, and never bring this up again!” AF SG •Specifics in 1988 •1988 – 1999 developed concept, equipment, training •2001-2015 proven effective •2009-15 implemented for NDMS in USA. Against Heavy Opposition Evolution of Critical Care in the Air • Aeromedical Evacuation (AE) system • Stable casualties only - GW1 and prior- “They might die on our airplanes!” • Critically ill patients could be transferred but the team had to be assembled ad hoc • Mogadishu, Somalia 1993 • Concept of Critical Care Air Transport Team developed and tested • Lt Gen Paul K. Carlton (ret.), MD, FACS • Col Christopher Farmer (ret.), MD, FACP • Col Jay Johannigman MD, FACS • Col Bill Beninati (ret), MD, FACP • BGen Rick Hersack (ret.), MD, AFMC/SG Critical Care Air Transport Team (CCATT) • Teams provide critical care expertise to manage patients in transit • Augment normal AE crew • Personnel • Active Duty • Guard and Reserve • Goal of 210 teams • 12-15 teams in theater • 4 special operations teams Critical Care Air Transport Team (CCATT) • Teams are multidisciplinary • Physician • Nurse • Respiratory Therapist • CCATT Course • 2 weeks • 3 ventilated patients • 6 patients maximum AE AIRFRAMES Opportune-- not dedicated Maximizes flexibility Critical Care in the Air We have now moved over 12,000 patients on ventilators in this current conflict! Over 100,000 total patients! 3 deaths enroute! CCATT Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Expeditionary Packages • Prevention and Aerospace Medicine (PAM) Team • Designed to prevent disease and non-battle injuries • Mobile Field Surgical Team (MFST) • Rapidly deployable, easily transportable, small surgical team • Small Portable Expeditionary Aeromedical Rapid Response Team (SPEARR) • Deployable within two hours • Flexible, broad scope of care • Critical Care Air Transport Team (CCATT) • For rapid aeromedical evacuation (AE) worldwide • Expeditionary Medical Support (EMEDS) • New version of traditional Air Transportable Clinic / Hospital • Biological Augmentation Team (BAT) • Field identification of pathogens of operational concern Modular Units of Capability: Providing What’s needed, When needed • The Crisis Defines the Response • Optimizes Resources • Maximizes Options for Commanders Staging Aug +20 Bed Expanded Beds +10 and +25 SPEAR Staging/Crews Comm Surgical TEAMS CRITICAL CARE PAM Teams Modular Units of Capability: Providing What’s needed, When needed • The was Crisis Defines This simply force packaging, as the the Response • Optimizes Resources Air Force line does so well! • Maximizes Options Staging Aug +20 Bed for Commanders Expanded Beds +10 and +25 SPEAR Staging/Crews Comm Surgical TEAMS CRITICAL CARE PAM Teams Prevention and Aerospace Medicine Team (PAM) • Designed to prevent disease and non-battle injuries • Missions/Tasks • Health threat/risk assessment • Health hazard surveillance, control, and mitigation of effects • Primary/emergency care, flight medicine • Population at risk; 2-10,000 • 9 personnel in 3 modules • Module 1 (Advon) - Aerospace medicine physician, public health officer • Module 2 - Bioenvironmental engineer (BEE), independent duty medical technician • Module 3- 2 public health technicians, 2 BEE technicians, aerospace physiologist Critical Care Air Transport Team (CCATT) • For Aeromedical Evacuation Patients • Capability: Provides in-flight critical care transport of 3 ICU patients; with 2nd critical care nurse, 5 stabilized patients • Personnel: 3 - 1 Physician, 1 Nurse, • 1 Respiratory Tech • Equipment: Light weight, compact, advanced and sophisticated patient management equipment and supplies • Operating Conditions: Work with 5 member AE crews to care for stabilized casualties; for tactical and strategic evacuation Mobile Field Surgical Team (MFST) Rapidly deployable, easily transportable, small surgical team Provide lifesaving trauma care within one hour of injury Personnel: 1-General Surgeon, 1-Orthopedic Surgeon, 1-Emergency Physician, 1-Anesthesiologist, 1-OR Nurse/Tech Equipment: Manportable 300 lbs of medical equipment and supplies in 5 backpacks, 60lb generator, 1 folding litter Capability: Care for up to 20 patients in 48 hrs; perform up to 10 life or limb saving/stabilization procedures Operating conditions: Intended for specialized surgery tasks as stand alone for short periods or as medical augmentation unit; transportable by any means; uses shelter of opportunity; no patient holding capability Similar Thinking Service Name Number Time USA FFST 50 1943 USAF FAST 20 1984 USA FST 24 1985 USAF MFST 5 1994 USN FSRT 8 2000 All interchangeable as needed Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Team Training Until 1999 our medical readiness focus was on the small tactical hospital to deploy with their fighter wings. The problem was that our small hospitals never took care of people who were sick, trauma patients! In 1999 we moved into our new world of Expeditionary Medical Support, EMEDS, which was focused on the Medical Centers as the primary responders. This lowered the training requirements but did not eliminate them! 1998 Push hard to establish “Ft. Ben Taub” in Houston Did in 1999 with joint team of 13 1 Army CC, 3 Navy enlisted, 9 AF 2000 - 2015 Training Spread •USAF Center for Sustainment Training and Readiness Skills (CSTARS) 1. Baltimore Shock Trauma 2. Cincinnati for CCATT 3. St. Louis for National Guard and reserves •USA – Miami •USN - LA Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Lacking to Achieve Vision - 1983 Standards Established RSVP Readiness Skills Verification Program RSVP-Dance Card •What are requirements to go to war? •Consultants answered those program questions. •RSVP criteria established for each deployable person For Example General surgery -50 open laps every 2 years -50 ventilated patient days -etc… If not met then go to CSTARS for 4 week update prior to deployment Certified for deployment! For Example CCATT Nurses • 50 ventilator patient days • Readiness training • Etc… If not met then go to CSTARS for 2 week update prior to deployment Certified for Deployment Result •Military teams better prepared for conflicts that started after 11 September 2001 •Patients more challenging in war, but principles are real and applicable •Learning never stopped– 1. First year in Balad, Iraq, we had an 80% wound infection rate, dropped to less than 1% with use of wound vac. 2. Compartment syndromes rose, we countered with aggressive decompressive surgery and changing timing for AE. History is Important 1995- on call one night at Wilford Hall we were discussing how to speed up our ability to put blood vessels back together over a difficult case. One item that came up was how to shorten the time to put blood vessels back together again once damaged from trauma. A bright young resident, Todd Rasmussen, and his staff, David Dawson, brought up the idea of using a shunt to bypass the vessel until you had time to repair it. History is Important They asked me to buy them 10 pigs to prove the point that an extremity could survive for 24 hours without damage using such a shunt. I did and they proved the point, published the paper, and we added the shunt to our surgical back packs. Fast forward to Feb 2010: Todd Rasmussen is now at the Bagram Hospital in Afghanistan on call. He has just received a young Marine woman who stepped on an IED on patrol. History is Important Her right leg was blown off below the knee. Her left groin took shrapnel and divided both artery and vein to her leg. Her battle buddy got two tourniquets on for her. She was resuscitated at a forward surgical station, using two shunts for the dual vascular injury, and shipped to him in about four hours. He reconstructed the artery and vein after removing the shunt- saving her remaining leg. He then took this picture, telling me that it was the best investment I had ever made, buying those 10 pigs, for the war wounded! 22 Year Old Marine 22 Year Old Marine Dr Rasmussen has now done over 1300 such cases in the current conflicts! Combat Casualty Statistics From Stansbury, Holcomb, Champion, Bellamy, 2005 25 Best we have ever done! 20 15 WWII Vietnam OIF/OEF 10 5 0 %KIA %DOW WIA = Wounded in Action (WIA =RTD+ Evacuated+ DOW) RTD = Returned to Duty in 72 hrs Evacuated = Not RTD in 72 hrs DOW = Died of Wounds KIA = Killed in Action CFR = Case Fatality Rate %CFR • %KIA = KIA / KIA + (WIA - RTD) • %DOW = DOW / WIA – RTD • %CFR = KIA +DOW / KIA + WIA Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Joint Cooperation •Casualty does not care who takes care of them – Army, Navy, Air Force, Marine Corp •They care that they get taken care of •Has required many years to get into “WE” mindset of Jointness! Team Military US Army US Air Force US Navy US Marine Corp All now closely integrated team members Focus Areas Historical Route From Injury to Definitive Care STRATEGIC EVAC TACTICAL EVAC CASUALTY EVAC - Evac Policy 15 Days - Evac Policy 7 Days - Evac Policy 1 Day Definitive Care “Level 4” In Theater Hospital “Level 3” Field Hospital “Level 2” Battalion Aid Station “Level 1” Out of “ME” and into “WE” JOINT TEAM Lacking to Achieve Vision - 1983 •Critical care in the air •Modular teams •Team training •Joint cooperation •Trauma Surgeon Mired in 60’s MIND SET ISSUE! Trauma Surgeon It had become clear that we needed a constantly prepared cadre of surgeons who had dedicated themselves to the care of the traumatically wounded in our military to really optimize our surgical care in the military. The Vietnam cadre had departed and we seemed to have a significant gap of skills between what we trained for peacetime healthcare and what we needed for wartime surgery. As we worked on these concepts in the military the private sector had come to the same conclusion and were developing the whole concept of a “trauma surgeon”. Trauma Surgeon This “trauma surgeon” would be taught in a fellowship program, post general surgery or orthopedic surgery residencies, the intricacies of ICU care, management of the trauma patient, mass casualties, system thinking for trauma care, and how to integrate all of the pieces of the puzzle into a cohesive team! Our military invested in several of these training programs with our best residents. The results have been remarkable! People like Ty Putnam, Don Jenkins, Jay Johanigman, David Kissinger, Warren Dorlac, Ken Kaylor, Mark Richardson, Jeff Bailey, etc. carried this focus on wartime medicine to the best outcomes in the history of war! Trauma Surgeon The current wartime strategy is the first ever designed by and for surgeons using modern techniques! The results speak for themselves! Give Me Examples! 1.Index case #1- first Nova Lung use. 2.Index case #2- first survivor of a traumatic pneumonectomy in wartime. 3.Index case #3- first survivor using ECMO in wartime. Give Me Examples! 1.Index case #1- first Nova Lung use. 2.Index case #2- first survivor of a traumatic pneumonectomy in wartime. 3.Index case #3- first survivor using ECMO in wartime. Index Case #1 1. 21 year old male, blown up in IED explosion in Iraq, 2006. 2. Severe lung injury resulting in an inability to oxygenate him on the ventilator, despite all the tricks known. 3. Dying quickly from this injury! Index Case #1 4. Call to Landstuhl Trauma Team- is there nothing we can do? 5. Landstuhl launched the new NovaLung Team to Baghdad, hooked the man up to the Nova Lung, flew him back to Germany, took him to a German hospital on the Nova Lung, where he spent two weeks on this device. EVOLUTIONARY ADVANCES: NOVALUNG Index Case #1 21 year old male, blown up in IED explosion in Iraq, 2006. Severe lung injury resulting in an inability to oxygenate him on the ventilator, despite all the tricks known. Dying quickly from this injury! Call to Landstuhl Trauma Team- is there nothing we can do? Landstuhl launched the new NovaLung Team to Baghdad, hooked the man up to the NovaLung, flew him back to Germany, took him to a German hospital on the NovaLung, where he spent two weeks on this device. He graduated to a conventional ventilator, was sent back to Landstuhl, and is now home with his family- stone cold normal in his physiology! The Army tried to Court Martial the AF physician who gave this man a chance at life! Give Me Examples! 1.Index case #1- first Nova Lung use. 2.Index case #2- first survivor of a traumatic pneumonectomy in wartime. 3.Index case #3- first survivor using ECMO in wartime. Index Case #2 1. 19 yo Male, shot at close range with AK-47. 2. Bullet entered his right side, went through the hilum of the right lung, and left him in shock! 3. This is the type of person who coughed blood up once or twice and died in any previous conflict! 4. Brought to a forward operating location where he was addressed surgically in minutes. 5. When the surgeon saw the extent of his injury he knew he was in trouble. 6. He had to remove the entire right lung, a traumatic pneumonectomy. Index Case #2 7. There had never been a survivor of this in war! 8. The surgeon called the Trauma Czar and asked for help! 9. The Trauma Czar mobilized the Nova Lung team from Germany, met them in Bagram, flew to the forward operating location, hooked the man up to the Nova Lung, and transported him back to Germany. EVOLUTIONARY ADVANCES: NOVALUNG Index Case #2 1. 2. 3. 4. 5. 6. 7. 8. 9. 19 yo Male, shot at close range with AK-47. Bullet entered his right side, went through the hilum of the right lung, and left him in shock! This is the type of person who coughed blood up once or twice and died in any previous conflict! Brought to a forward operating location where he was addressed surgically. When the surgeon saw the extent of his injury he knew he was in trouble. He had to remove the entire right lung, a traumatic pneumonectory. There had never been a survivor of this in war! He called the Trauma Czar and asked for help! The Trauma Czar mobilized the NovaLung team from Germany, met them in Bagram, flew to the forward operating location, hooked the man up to the NovaLung, and transported him back to Germany. 10.This gentleman spent several weeks on the Nova Lung and then went home. 11.He is doing well at home now with no complications. Give Me Examples! 1.Index case #1- first NovaLung use. 2.Index case #2- first survivor of a traumatic pneumonectomy in wartime. 3.Index case #3- first survivor using ECMO, a heart lung machine, in wartime. Index Case #3 1. 19 yo Male, shot at close range with AK-47. 2. Bullet entered his right side, went through the hilum of the right lung, proceeded across the mediasteinum, took off the top of his left lung, and left him in shock! 3. This is the type of person who had no chance for survival in any previous conflict! Index Case #3 4. His buddies got him to a Far Forward Surgical team in Afghanistan very quickly. 5. The surgeon addressed him surgically, had to remove his right lung and a portion of his left lung. 6. The surgeon called the “Trauma Czar” as he started, asking for help! 7. The “Trauma Czar” was well experienced, had taken care of the first survivor of a traumatic pneumonectomy in history and knew what would happen to the patient- his right heart would fail within 24 hours. Index Case #3 8. The “Trauma Czar” called for the ECMO team to come from Germany to pick this young man up, giving them a very short window to arrive. 9. They arrived at the 16 hour mark, traveled with the Trauma Czar to the forward location, and hooked up the patient to the heart lung machine at the 20 hour mark as he was entering florid right heart failure. EVOLUTIONARY ADVANCES: EXTRACORPOREAL MEMBRANE OXYGENATION We had to work this one for our people on Okinawa in the NICU from 1985 to present! This was certified for AE use on 1 Oct 2010. It was used on this patient for the first time two weeks later. Index Case #3 10. They then flew this young man back to Germany, kept him on the machine for two weeks to allow his heart to accommodate his new circulation, and he is home now with his family! 11. He has a normal life expectancy! Index Case #3 10. They then flew this young man back to Germany, kept him on the machine for two weeks to allow his heart to accommodate his new circulation, and he is home now with his family! 11. He has a normal life expectancy! That is what we mean by “nothing is too good for those in uniform!” “In times of change the learners will inherit the world… while the learned will find themselves beautifully equipped to deal with a world that no longer exists” Eric Hoffer A Little Humor Don’t accept your dog’s admiration as conclusive evidence that you are wonderful! How to Dissent Begin with the end in mind FINISH Combat Casualty Statistics From Stansbury, Holcomb, Champion, Bellamy, 2005 Best survival we have ever had in the history of war! 25 20 15 WWII Vietnam OIF/OEF 10 5 0 %KIA %DOW WIA = Wounded in Action (WIA =RTD+ Evacuated+ DOW) RTD = Returned to Duty in 72 hrs Evacuated = Not RTD in 72 hrs DOW = Died of Wounds KIA = Killed in Action CFR = Case Fatality Rate %CFR • %KIA = KIA / KIA + (WIA - RTD) • %DOW = DOW / WIA – RTD • %CFR = KIA +DOW / KIA + WIA Press On Nothing in the World can take the place of persistence. Talent will not; nothing is more common than An Aviators perspective! unsuccessful men with talent. Genius will not; unrewarded genius is almost a proverb. Education will not; the world is full of educated derelicts. Persistence and determination alone are omnipotent! Calvin Coolidge 1929 Historical Review of Casualty Care 1.Antiquity 2.Napoleon's Surgeon 3.Civil War and anesthesia. 4.Boer War. 5.WWI 6.WWII 7.Korea 8.Vietnam 9.Current Activity Questions? Medical Initiatives in Current Wars Medical Initiatives Updated 22March12 Sum total: NavyArmyAir ForceShared A/AF/NCOALITION- 0. 2. 25. 10. 2. FOR THE NEXT CONFLICT, CAN WE AFFORD TO LOSE THE AIR FORCE CONTRIBUTION? CLEARLY, THE ANSWER IS NO!