2014 Tax Letter
advertisement

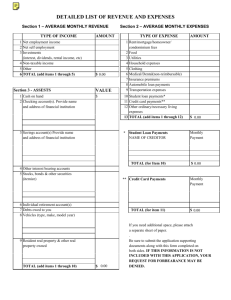
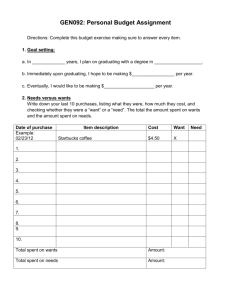
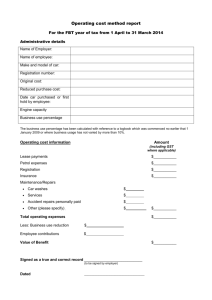
DONALD C. TAYLOR JASON C. TAYLOR LAURA R. CLASE GEORGE W. TAYLOR To All Tax Clients of Taylor’s Accounting & Tax Service Attached are income tax information sheets to be completed by you, covering your business and personal income and deductions. This checklist should be completed, signed and either mailed or brought in at the time of your appointment. Please call as soon as possible after you receive this letter to schedule an appointment that is convenient for you. Starting January 1, 2014 the Affordable Care Act (Obamacare) went into effect. The reporting of this coverage will be included on your 2014 return. We are required to determine if your health care coverage is sufficient to avoid being charged a penalty. Please answer all the questions related to Health Care Coverage on Page 2 of this checklist. All returns will be e-filed again this year. We must have a signed Form 8879 in our office before we can transmit any return. Please complete the attached worksheet before your appointment. Taylor’s Accounting Home_______________ Taxpayer__________________________Spouse________________________Phone # Work_______________ Cell _______________ Address________________________________City____________________County__________Zip_________ Taxpayers Social Security #_________________________Birthdate________________Occupation_________________ Spouse’s Social Security #_________________________Birthdate________________Occupation__________________ Bank Information - (for direct deposit of refund checks) Routing Number______________________ Savings _____________ Account Number______________________ Checking ____________ Dependents Name _________________ _________________ _________________ Relationship __________ __________ __________ Employer ________________ ________________ ________________ ________________ ________________ Box 1 _____ _____ _____ _____ _____ Birthdate ______ ______ ______ Box 2 _____ _____ _____ _____ _____ W-2 Wages Box 4 _____ _____ _____ _____ _____ Social Security # _____________________ _____________________ _____________________ # of Months in your home in 2014 __________ __________ __________ Box 6 _____ _____ _____ _____ _____ Box 19 _____ _____ _____ _____ _____ Box 17 _____ _____ _____ _____ _____ Interest and Dividend Income Amount – Please bring in your Dividend 1099’s Interest Income Amount Dividend Income Total Qualified Payer Payer ____________ ______________ ______________ _______________ _____________ _____________ ______________ ______________ _______________ _____________ _____________ ______________ ______________ _______________ _____________ Do you have a foreign bank account? Yes_______ No_________ Please bring in last statement Have you been a victim of Identity Theft? If yes – what is your PIN Number?_______________________ Mutual Fund Dividends – Please bring in your 1099’s Payer Dividends Qualified Dividends Capital Gain ________________ ________________ _____________________ ____________________ ________________ ________________ _____________________ ____________________ ________________ ________________ _____________________ ____________________ Other Income 2013 State Refund Received in 2014 _______________________________ Unemployment Income _______________________________ Partnership Income-Attach K-1 _______________________________ Prizes, Awards, Lottery _______________________________ Social Security Income _______________________________ Payer Amount Pension Income ______________ ____________________ ______________ ____________________ Do you have Health Insurance _________________ ____________________ Yes No If no, were you issued an exemption from paying Health Insurance _____________________ If yes, did you purchase from: _____________ _______________ _________________ Exchange Employer Other If purchased through the exchange, did you receive Form 1095-A? ________________ How many months did you have coverage? ______________________ Medical Expenses These expenses must exceed 10 % of your Gross Income. 1. 2. 3. 4. 5. 6. Hospitalization Insurance Premiums Prescription Transportation, Miles for Medical Medical Equipment, Eye Glasses, etc. Doctors, Dentists, and Hospital payments Long Term Care Insurance ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ _______________# of Policies__________ Taxes 1. 2. 3. 4. Real Estate Taxes on Home State Income Tax Withheld Ownership Tax on Cars Sales Tax paid on Auto Purchase ___________________________ ___________________________ ___________________________ ___________________________ Interest 1. Home Mortgage Interest st 1 Mortgage 2nd Mortgage Bank Name _____________ _____________ Additional Home Loan Information : Purchase Price of House Original Loan Amount Current Loan Amount 2. Deductible Points 3. Did you refinance this year? Length of new loan? 4. If yes, please bring a copy of the settlement sheet! 1. Moving Expenses Amount _______________ _______________ _______________ _______________ _______________ _______________ _______________ Other Deductions _________________________ 2. Alimony/Maintenance List recipients SS#___________________ _________________________ 3. Adoption Expenses _________________________ 4. Child Care Expense _________________________ Federal ID # or SS # ___________ ___________ ___________ ___________ ___________ Paid To __________________ __________________ __________________ __________________ __________________ Address _____________________ _____________________ _____________________ _____________________ _____________________ Amount _________ _________ _________ _________ _________ Phone # _________ _________ _________ _________ _________ College Education Expenses-Please Bring Form 1098-T Student Name ____________________ ____________________ ____________________ Year in College ____________________ ____________________ ____________________ Education Related Interest Payments to 529 Plans Did your employer offer a retirement plan? Payment to IRA Payments to SEP Payments to Roth IRA School Name _______________ _______________ _______________ Tuition Expense _________________ _________________ _________________ _____________________ _____________________ Taxpayer Spouse _____ ______ Yes No ____________ ____________ ____________ _______ _______ Yes No _______________ _______________ _______________ Expenses incurred in connection with your employment not reimbursed by your employer. Does not include commuting to and from work. Car 1 _____________ _____________ _____________ Car 2 _______________ _______________ _______________ 5. Travel, Airfare Expenses 6. Expenses for Meals 7. Expenses for Lodging ______ _______ Yes No ______________ ______________ ______________ ______ _________ Yes No ________________ ________________ ________________ 8. Other Business Expenses: Description _____________________ Description _____________________ Description _____________________ Description _____________________ Amount____________________ Amount____________________ Amount____________________ Amount____________________ 1. 2. 3. 4. Auto expenses; Gas, Ins., Repairs, Lease Total Miles Driven – 2014 Business Miles Do you have written evidence to support car mileage? Estimated Tax Payments in 2014 Federal ________________ ________________ ________________ ________________ 4/15/14 6/15/14 9/15/14 1/15/15 State _______________ _______________ _______________ _______________ Contributions 1. Cash Contributions, for which you have receipts, cancelled checks. Please list each organization separately. A receipt from the organization is needed for all donations. Organization ___________________ ___________________ ___________________ ___________________ Amount _____________ _____________ _____________ _____________ Do you have a Receipt? ___________________ ___________________ ___________________ ___________________ 2. Non-Cash Contributions – If over $500 – Itemized list needed. Amount _____________ _____________ _____________ _____________ _____________ Date ______ ______ ______ ______ ______ To Whom __________ __________ __________ __________ __________ Description of items __________________ __________________ __________________ __________________ __________________ How was value determined? ________________ ________________ ________________ ________________ ________________ 3. How many miles did you travel during the year in connection with church and other charitable work a s a volunteer fireman, scout master, PTA, etc. ___________________________ Miscellaneous Items The total of these items must exceed 2% of gross income before they become deductible. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Small tools used for work Tax preparation fee Special clothing for work Trade Books and Publications Union Dues Safe Deposit Box Rental Employment agency fees, resumes Investment Expenses Employment related education Teaching Supplies Other miscellaneous deductions ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ ___________________________ The answers to all questions are complete and accurate. If I become aware of any oversight or missing information before the return is prepared I will notify you immediately. __________________________________ Signature Date Rental Income & Expenses- (List each property separately) Property Address___________________________ Rents Received ____________________________ Date Purchased________________ Date Rented___________________ Expenses Rent Income and Expenses Advertising_____________________________ Auto & Travel___________________________ Maintenance____________________________ Commissions____________________________ Insurance_______________________________ Interest_________________________________ Legal_________________________ Repairs_______________________ Supplies_______________________ Taxes_________________________ Utilities_______________________ Misc._________________________ Appliances, Major Improvements, Etc. Description _________________________ Description__________________________ Amount_______________________ Amount_______________________ Small Business Income & Expenses If you use a portion of your home for business use, please provide: Square footage of office_____________ Square footage of home_________________________ Home Insurance________________Home Utilities______________Home Repairs_________________ Business Income_____________________________ Expenses Advertising__________________________ Bank Charges________________________ Car Expenses/Miles___________________ Commissions________________________ Dues_______________________________ Freight_____________________________ Insurance___________________________ Interest_____________________________ Laundry____________________________ Office Supplies_______________________ Professional Fees______________________ Rent________________________________ Repairs______________________________ Supplies_____________________________ Taxes_______________________________ Utilities_____________________________ Misc._______________________________ Travel & Entertainment_________________ Major Purchases (Description)__________________________________________________________ Sales of stock of property Description Date Acquired Date Sold Selling Price Cost 1.______________ 2.______________ 3.______________ 4.______________ ____________ ____________ ____________ ____________ ____________ ____________ ____________ ____________ ______________ ______________ ______________ ______________ ____________ ____________ ____________ ____________