Dialysis - North West Urology Registrar Group
advertisement

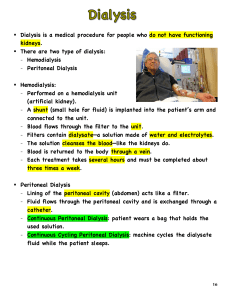
Haemodialysis Diffusion of solutes, ultrafiltration of fluid across a semi-permeable membrane. MCQ 1. Acidosis with pH<7 not responding to treatment is an indication for dialysis. 2. Gastritis, hypothermia, and fits are signs of uraemia. 3. CAPD involves one exchange of fluid a day. 4. Hypoglycaemia is a complication of peritoneal dialysis. 5. An abdominal wall stoma is not a contraindication to peritoneal dialysis. Indications for dialysis 1. ARF 2. CRF Indications in ARF • Absolute indications: – Uraemia » (e.g. pericarditis, gastritis, hypothermia, fits or encephalopathy) – Fluid overload » leading to pulmonary oedema not resolving with diuretics – Severe Hyperkalaemia » (potassium > 6.5mmol/L) unresponsive to medical management – Acidosis » (pH < 7.0) not responding to treatment (eg. sodium bicarbonate) • Relative indications: – Serum sodium > 155mmol/L or < 120 mmol/L – Severe renal failure (urea > 30 mmol/L, Creatinine > 500 micromol/L) – Toxicity with drugs that can be dialysed Indications in Chronic Renal Failure • When to start dialysis is controversial (if no urgent indication) • In general, GFR 10 mL/minute (15 mL/minute if diabetic) • Before <6 ml/min regardless • No evidence that starting dialysis earlier is of any benefit to patients • Mortality rate and low quality of life VS complications of CRF (malnutrition) IDEAL Study • NEJM. 2010;363(7):609-19 – RCT, 32 centres Australia / NZ, 828 adults – Early (eGFR 10-15ml/min) vs Late (eGFR 5-7 ml/min) – No significant difference in survival or clinical outcomes • No RCTs comparing HD with HF but Cochrane Review in 2006 showed equivalence (Rabindranath, CD006258) Principles of dialysis Principles of dialysis Components • Blood side – blood flows on one side • Dialysis side – dialysate flows on other side • The dialysate contains H2O,Na, K, Cl,HCO3, Mg, Ca, Dextrose • Dialyser unit with semi-permeable membranes. – Bundles of capillary-like hollow fibres in cylindrical shell – Blood flows through fibres, dialysate flows within surrounding shell Process • Vascular access - AV fistula (3-6 months before), AV graft or central venous catheter (CVC) • Extracorporeal circuit with heparin pump • Blood from vascular access delivered to dialyser at 200-400 ml/min – Entire blood volume through machine every 15 minutes • Blood flows in opposite direction to dialysate – counter-current – Maintains concentration gradient for maximum efficiency of diffusion • Diffusion of solutes across semi-permeable membrane • Ultrafiltration - to remove excess body water – Achieved by altering hydrostatic pressure of dialysate compartment • Patient is exposed to 120L of water each session • For CRF: three times each week for about 4 hours Peritoneal Dialysis – The semi permeable membrane: peritoneum – Dialysate infused into peritoneal cavity through a permanent tunnelled Tenckhoff catheter – Peritoneal capillaries are the source of blood – The dialysate is exchanged either • each night : automated peritoneal dialysis OR • Regular exchanges during the day (Continuous ambulatory peritoneal dialysis- CAPD) • Usually 4 exchanges/day (20 minutes) • 1.5-3 litres per exchange –Solute normally contains sodium, chloride, lactate or bicarbonate. –Ultrafiltration is controlled by altering the osmolality achieved with glucose or other large molecular weight solutes in the dialysate. Haemofiltration • Convection of water and solutes across semi-permeable membrane • Blood via double lumen CVC passes through anticoagulation port into dialyser at 100-200 ml/min • Solutes move from blood to filtrate compartment driven by positive hydrostatic pressure • Allows extraction of larger molecular weight molecules than HD • Similar filtration rate irrespective of solute size • Large quantity of water removed requiring replacement fluid to prevent hypovolaemia • Replacement fluid – isotonic • Haemofiltration rate of 1L/hr = 1L fluid removed and replaced • Anticoagulation important due to activation of clotting cascades (heparin/citrate) Haemodiafiltration Haemodiafiltration • Combination of diffusion and convection • Haemodialysis combined with haemofiltration • Better removal of small and large molecules (urea, B2 microglobulin,) •Less problematic hypotension as losses replaced by substitution fluid Complications of Haemodialysis Access related: – – – – local infection, endocarditis, osteomyelitis, creation of stenosis, – thrombosis or aneurysm. During haemodialysis: – – – – – – – – – – – Hypotension (common), cardiac arrhythmias, air embolism Nausea and vomiting, headache, Cramps Fever: infected central lines Dialyser reactions: anaphylaxis Heparin-induced thrombocytopenia Haemolysis Disequilibration syndrome: • • restlessness, headache, tremors, fits and coma Complications of Peritoneal Dialysis – Complications • Peritonitis (infective), also sclerosing peritonitis • Catheter problems: – – – – Infection Blockage, kinking Leaks Slow drainage • Dietary complications – – – – Hyperglycemia, poor diabetic control weight gain (due to dextrose- avoid fats) Malnutrition (need high protein diet) Constipation • Others – – – – Fluid retention/ hypovolaemia Intraperitoneal bleeding Hernias (incisional, inguinal, umbilical) Back pain – Amyloid CRRT Therapy (Continuous Renal Replacement Therapy) • Slow Continuous Ultrafiltration (SCUF) • Continuous Veno-Venous Haemofiltration (CVVH) • Continuous Veno-Venous Haemodialysis (CVVHD) • Continuous Veno-Venous Haemodiafiltration (CVVHDF) • Continuous Ambulatory Peritoneal Dialysis (CAPD) MCQ 1. Acidosis with pH<7 not responding to treatment is an indication for dialysis. TRUE 2. Gastritis, hypothermia, and fits are signs of uraemia. TRUE 3. CAPD involves one exchange of fluid a day. FALSE 4. Hypoglycaemia is a complication of peritoneal dialysis. FALSE 5. An abdominal wall stoma is not a contraindication to peritoneal dialysis. TRUE