Matrix of Evidence Based Practices
advertisement

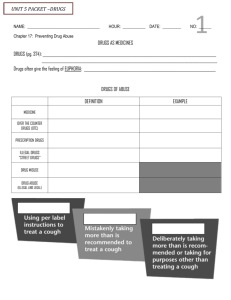
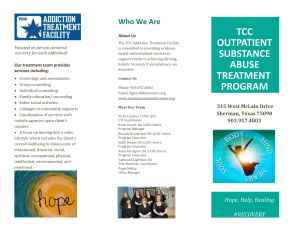
Matrix of Interventions Evidence-Based Practices for Treatment of Adults with Substance Use Disorder Adapted from University of Washington Alcohol and Drug Abuse Institute* Behavioral Couples $ Therapy 3. Behavioral SelfControl Training 4. N N No Brief Cognitive Behavioral Intervention for Amphetamine D 5. Brief Marijuana Dependence Counseling D N N 6. Cognitive Behavioral Coping Skills Therapy D 7. Community Reinforcement Approach (CRA) with Vouchers D Contingency Management without CRA No 9. (Lower Cost) Contingency Management No No 8. 10. Day Tx with Contingencies & Vouchers Opiate substitution clients Offenders Low income IV drug user Homeless Co-occurring patients N Housing, employment N Women and/or pregnant women Poly-substance Marijuana Heroin/opiates N Reduced depression Cocaine/crack N Meth/amphetamine N Adverse consequences from drinking (N) Fewer arrests and hospitalizations, improved relationships (N) Adverse consequences from drinking; reduced partner violence Mild/moderate problem drinking N Alcohol problems N Hispanic/Latino 2. D Other (e.g., legal, family, interpersonal, medical) Population African Americans Twelve-Step Facilitation Abstinence from substances 1. Reduced substance use Outcomes/substance: N=Listed in NREPP 1 Treatment completion **Manual availability: D= Free download $ = Purchase copy No = No manual Retention Manual availability** See Appendix 1 for references Not specific to one drug Problematic substance Positive outcomes Engagement Practice ASI drug use composite score (when used with #12) 12. Individual Drug Counseling for Cocaine Addiction: CCTS Model D ASI drug use composite score (when used with #11) 13. Matrix Intensive Outpatient Program for the Tx of Stimulant Abuse $/D N N N HIV risk 14. Motivational Enhancement Therapy (MET) D N N Motivation, social functioning N N Commitment to treatment, HIV risk, illegal activity N N N N Reduced PTSD symptoms N N Lower methadone dose, reduced depression N N Reduced mental health symptoms, HIV risk 15. Mapping Enhanced D Counseling N 16. Relapse Prevention D Therapy 17. Seeking Safety: A Psychotherapy for Trauma/PTSD and Substance Abuse $ 18. SupportiveExpressive Psychotherapy $ 19. Boston Consortium Model: TraumaD Informed SUD TX for Women N N N Marital adjustment (N) N N N N N N N N N N N N Opiate substitution clients IV drug user Homeless Co-occurring patients Women and/or pregnant women Hispanic/Latino African Americans Poly-substance N Marijuana Heroin/opiates Cocaine/crack Meth/amphetamine Offenders D Population Low income 11. Group Drug Counseling for Cocaine Addiction: CCTS Model Mild/moderate problem drinking Other (e.g., legal, family, interpersonal, medical) Alcohol problems Abstinence from substances Reduced substance use Outcomes/substance: N=Listed in NREPP 1 Treatment completion **Manual availability: D= Free download $ = Purchase copy No = No manual Retention Manual availability** See Appendix 1 for references Not specific to one drug Problematic substance Positive outcomes Engagement Practice N *Adapted from the University of Washington Alcohol and Drug Abuse Institute (ADAI). Evidence-Based Practices for Treating Substance Use Disorders: Matrix of Interventions, August 2006. URL: http://adai.washington.edu/ebp/matrix.pdf 1 NREPP= SAMHSA National Registry of Evidence-based Programs and Practices, http://nrepp.samhsa.gov/ APPENDIX I Information on Evidence-Based Practices The following list of evidence-based practices (EBPs) corresponding to the matrix (see previous page) describes each EBP, provides references that support the link between the practice and client outcomes, and, if available, research on fidelity to the practice. This list also includes links to downloadable manuals, if available. 1. Twelve-Step Facilitation Therapy (TSF). TSF is a strategy designed to increase the likelihood of a substance abuser becoming actively involved in 12-step self-help groups, thereby promoting abstinence. This EBP is a brief, structured, manual-driven approach to facilitate early recovery from alcohol abuse, alcoholism, and other drug abuse and addiction problems. Research from Project MATCH indicates that compared with participants who received treatment as usual, TSF participants had a higher percentage of days abstinent in the prior 3 months at 6 months and 12 months posttreatment (Project MATCH Research Group, 1998a). Kaskutas and colleagues (2009) developed a related approach, “Making AA Easier” (MAAEZ), a six-session manual-guided intervention designed to help clients connect with individuals encountered in AA. Fidelity Over 80 therapists from diverse backgrounds received careful training and supervision using Project MATCH structured manuals and were able to implement the TSF therapy successfully and with fidelity (Project MATCH Research Group, 1998b). In addition, Sholomskas and Carroll (2006) developed a feasible and effective computer-assisted training program to impart skills associated with the delivery of TSF. A study by Guydish and others (2013) found that higher competence and empathy in the delivery of TSF was associated with fewer days of drug use and better employment outcomes at 3 months post-baseline; greater adherence to the protocol was associated with better employment outcomes only (TSF was adapted for groups and stimulant users). References reporting improved client outcomes: Kaskutas LA, Subbaraman MS, Witbrodt J, & Zemore SE. (2009). Effectiveness of making Alcoholics Anonymous easier: A group format 12-step facilitation approach. Journal of Substance Abuse Treatment, 37, 228-239. Project MATCH Research Group. (1998a). Matching patients with alcohol disorders to treatments: Clinical implications from Project MATCH. Journal of Mental Health, 7, 589-602. Project MATCH Research Group. (1998b). Matching alcoholism treatments to client heterogeneity: Project MATCH three-year drinking outcomes. Alcoholism: Clinical and Experimental Research, 22, 1300-1311. Treatment manual: Nowinski J, Baker S, Carroll K. (1995). Twelve Step Facilitation Therapy Manual: A Clinical Research Guide for Therapists Treating Individuals with Alcohol Abuse and Dependence. National Institute on Alcohol Abuse and Alcoholism Project MATCH Monograph Series vol. 1. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism. http://lib.adai.washington.edu/pubs/match1/match1.pdf 2. Behavioral Couples Therapy for Alcoholism and Drug Abuse (BCT): In BCT, the therapist works with both the person who is abusing substances and his or her partner to build a relationship that supports abstinence. Program components include a recovery contract between the partners and therapist; activities and assignments designed to increase positive feelings, shared activities, and constructive communication; and relapse prevention planning. Partners generally attend 15–20 hour-long sessions over 5–6 months. During the 1-year posttreatment follow-up, participants who received BCT reported fewer days of drinking, fewer drinking-related negative consequences, higher dyadic adjustment, and reduced partner violence, compared with participants who received individual or educational support (FalsStewart et al., 2006). Fidelity In an effectiveness study of BCT by Fals-Stewart et al. (2006), all sessions were audiotaped, and three of the sessions for each participant were randomly selected and rated for adherence and compliance by an experienced clinical psychologist who had extensive knowledge of BCT. Adherence and competence scores for all rated sessions in all the conditions were acceptable. Fidelity requirement for improved outcomes not found (i.e., a literature search was conducted for information on the extent that BCT treatment fidelity might be associated with better outcomes; however, information could not be found. References reporting improved client outcomes: Fals-Stewart W, Birchler GR, & Kelley ML. (2006). Learning sobriety together: A randomized clinical trial examining behavioral couples therapy with alcoholic female patients. Journal of Consulting and Clinical Psychology, 74, 579-591. Schumm JA, O'Farrell TJ, & Andreas JB. (2012). Behavioral couples therapy when both partners have a current alcohol use disorder. Alcoholism Treatment Quarterly, 30, 407-421. Treatment manual: The following guidebook is available: O'Farrell TJ, & Fals-Stewart W. (2006). Behavioral couples therapy for alcoholism and drug abuse. New York: Guilford Press. Slides describing BCT and information to order the book are available at: http://uwf.edu/cap/DeploymentMentalHealth/materials/Dr.%20Timothy%20O'Farrell%20%20Behavioral%20Couples%20Therapy%20for%20Alcoholism%20and%20Drug%20Abuse.pd f 3. Behavioral Self-Control Training for Alcohol Use (BSCT): BSCT is an approach used with individuals who have a treatment goal of either controlled/non-problematic drinking or abstinence. BSCT includes six elements: specific goal-setting, self-monitoring of drinking or urges to drink, strategies to reduce or avoid consumption, self-reinforcement for achievement of goals, identification of high-risk situations, and alternatives to drinking as a coping response. A review of treatments for mild to moderate problem drinking indicates several studies demonstrate the robust efficacy of behavioral self-control strategies in reducing alcohol consumption among problem drinkers with low levels of physical dependence on alcohol (Walitzer & Connors, 1999). Fidelity: No formal treatment manual has been developed for BSCT. Walitzer and Connors (1999) reported that studies of the effectiveness of this approach found numerous variations in how BSCT was implemented. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Walters GD. (2001). Behavioral self-control training for problem drinkers: A meta-analysis of randomized control studies. Behavior Therapy, 31, 135-149. Walitzer KS, & Connors GJ. (1999). Treating problem drinking. Alcohol Research & Health, 23, 138-143. Treatment manual: Not applicable. Information about BSCT is available in: Miller WR, & Muñoz RF. (2013). Controlling Your Drinking, 2nd Edition, Tools to Make Moderation Work for You. New York: Guilford Press. Miller WR, & Muñoz RF. (1982). How to control your drinking. Albuquerque: University of New Mexico Press. 4. Brief Cognitive Behavioral Intervention for Amphetamine Users. This intervention consists of four weekly individual sessions lasting 45–60 minutes that are focused on developing skills to reduce amphetamine use. The sessions involve motivational interviewing, coping with cravings and lapses, controlling thoughts about amphetamine use, developing skills to refuse amphetamine use, and preparation for future high-risk situations. A pilot study (Baker et al., 2001) and a full-scale trial (Baker et al., 2005) were conducted in Australia; both studies showed an overall decrease in amphetamine use across the control and treatment groups and a significant increase in abstinence in the treatment groups compared to the control groups. Fidelity: Therapists received a week-long training session prior to delivering the manualized intervention that covered research procedures and role-plays of treatment sessions. Videotaped feedback was used to enhance training. Session checklists were employed to guide weekly supervision. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Baker A, Boggs TG, Lewin TJ. (2001). Randomized controlled trial of brief cognitive – behavioural interventions among regular users of amphetamine. Addiction, 96, 1279 – 87. Baker A, Lee NK, Claire M, Lewin TJ, Grant T, Pohlman S, et al. (2005). Brief cognitive behavioural interventions for regular amphetamine users: a step in the right direction. Addiction, 100, 367-378. Treatment manual: Baker A, Kay-Lambkin F, Lee N, Claire M & Jenner L. (2003) A Brief Cognitive-Behavioural Intervention for Regular Amphetamine Users. Canberra: Australian Government Department of Health and Aging. http://www.health.gov.au/internet/main/publishing.nsf/content/1DEA7F68576F8F16CA257BF00 01F3E5C/$File/cognitive-intervention.pdf 5. Brief Marijuana Dependence Counseling (BMDC). BMDC combines elements from motivational enhancement therapy (MET), cognitive behavioral therapy (CBT), and case management. It consists of an assessment session followed by nine weekly one-on-one sessions: Enhancing Motivation (sessions 1 and 2); and Changing Marijuana Use through Skill Building (sessions 3 through 9). Participants in nine sessions significantly reduced the percentage of days in which they used marijuana by an averaged of 58.8%, compared with a 35.7% reduction among participants in a two-session program and a 15.9% reduction among clients awaiting services (Marijuana Treatment Project [MTP] Research Group, 2004). Fidelity: Independent evaluators reviewed sample treatment sessions to assess therapists’ adherence to the manuals throughout treatment (MTP Research Group, 2004; Litt et al., 2005). In a subsequent study, BMDC was delivered as specified in the MTP (9 sessions, each lasting 60– minutes) and was based on the therapy manual developed for MTP (Kadden et al., 2007). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Kadden RM, Litt MD, Kabela-Cormier E, & Petry NM. (2007). Abstinence rates following behavioral treatments for marijuana dependence. Addictive Behaviors, 32, 1220-1236. Litt MD, Kadden RM, Stephens RS. (2005). Coping and self-efficacy in marijuana treatment: results from the Marijuana Treatment Project. Journal of Consulting and Clinical Psychology 73, 1015-25. Marijuana Treatment Project (MTP) Research Group. (2004). Brief treatments for cannabis dependence: findings from a randomized multisite trial. Journal of Consulting and Clinical Psychology, 72, 455-66. Treatment manual: Steinberg KL, Roffman, RA, Carroll, KM, McRee B, Babor, TF, Miller, M, Kadden, R, Duresky D, and Stephens, R. (2005). Brief Counseling for Marijuana Dependence: A Manual for Treating Adults. DHHS Publication No (SMA) 05-4022.Rockville, MD: Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration. http://www.integration.samhsa.gov/clinicalpractice/sbirt/brief_counseling_for_marijuana_dependence.pdf 6. Cognitive Behavioral Coping Skills Therapy (CBT) Cognitive behavioral approaches, such as relapse prevention, are grounded in social learning theories and principles of operant conditioning. The defining features of these approaches emphasize functional analysis of drug use and skills training (Carroll & Onken, 2005). A specific 12-session CBT individual intervention used in Project MATCH aimed to improve patients’ cognitive and behavioral skills for changing problematic alcohol behavior. Later, CBT was adapted for cocaine-addicted individuals and is listed in NIDA’s Principles of Drug Addiction Treatment (2012) as effective with individuals who use methamphetamine, marijuana, and nicotine, in addition to alcohol and cocaine. Participants in all Project MATCH conditions, including CBT, showed significant reductions in drinking in the first year after treatment, and these reductions were sustained over the 3-year follow-up period; almost 30% were totally abstinent in months 37 to 39 (Project MATCH Research Group, 1998). A meta-analysis suggests that CBT may be more effective for treating alcohol than cocaine problems (Irvin et al., 1999). However, among cocaine users, those who received CBT reduced their cocaine use significantly more than those who received interpersonal psychotherapy (Carroll et al., 2004). Fidelity: Over 80 therapists from diverse backgrounds received careful training and supervision using Project MATCH structured manuals and were able to implement the CBT therapy successfully and with fidelity (Project MATCH Research Group, 1998). A study of treatment providers assigned to either review the CBT manual only (manual only); review the manual and access the CBT training website (website); or review the manual and participate in a didactic seminar followed by supervised casework (supervision) found significant differences in protocol adherence and skill ratings favoring the seminar plus supervision over the manual-only condition, with intermediate scores for the website condition (Sholomskas et al., 2005). However, this study did not address the extent to which the type of training affected actual patient outcomes. A study by Hogue (2008) found that better adherence to a cognitive behavioral intervention targeting adolescent substance use and other problems predicted better drug use outcomes when the therapeutic alliance was controlled. Overall, cognitive behavioral approaches may be comparatively complex, and training clinicians to implement these approaches effectively can be challenging (Carroll & Onken, 2005). References reporting improved client outcomes: Carroll KM, Fenton LR, Ball SA, Nich C, Frankforter TL, Shi J, & Rounsaville BJ. (2004). Efficacy of Disulfiram and Cognitive Behavior Therapy in Cocaine-Dependent Outpatients: A Randomized Placebo-Controlled Trial. Archives of General Psychiatry, 61, 264-272. Carroll KM, and Onken LS. (2005). Behavioral therapies for drug abuse. The American Journal of Psychiatry, 168, 1452–1460. Carroll KM, Rounsaville BJ, Gawin FH. (1991). A comparative trial of psychotherapies for ambulatory cocaine abusers: Relapse prevention and interpersonal therapy. American Journal of Drug and Alcohol Dependence, 17, 229-247. Irvin JE, Bowers CA, Dunn ME, & Wang MC. (1999). Efficacy of relapse prevention, a metaanalytic review. Journal of Consulting and Clinical Psychology, 67, 563-570. National Institute on Drug Abuse (NIDA). (2012). Principles of Drug Addiction Treatment, 3rd edition. (NIH Publication No. 12-4180) NIDA, Bethesda, MD. Project MATCH Research Group. (1997). Matching alcoholism treatments to client heterogeneity: Project MATCH post treatment drinking outcomes. Journal of Studies on Alcohol and Drugs, 58, 7-29. Treatment manual: The CBT manual from Project MATCH (addressing alcohol problems) is: Kadden R, Carroll K, Donovan D, Cooney N, Monti P, Abrams D, Litt M, Hester R (1992). Cognitive-behavioral Coping Skills Therapy Manual, A Clinical Research Guide for Therapists Treating Individuals with Alcohol Abuse and Dependence. (NIAAA Project MATCH Monograph, Vol. 3, DHHS Publication No. ADM 92-1895). Washington, DC: U.S. Government Printing Office. http://pubs.niaaa.nih.gov/publications/MATCHSeries3/Project%20MATCH%20Vol_3.pdf The CBT manual for cocaine addiction is: Carroll KM. (2000). A Cognitive-behavioral Approach: Treating Cocaine Addiction. US Dept. of Health and Human Services, National Institutes of Health, National Institute on Drug Abuse. http://archives.drugabuse.gov/pdf/CBT.pdf 7. Community Reinforcement Approach (CRA) with Vouchers. CRA with Vouchers uses a range of recreational, familial, social, and vocational reinforcements, as well as material incentives to make a non-drug-using lifestyle more rewarding than substance use. The treatment goals among cocaine users are to maintain drug abstinence long enough to learn new life skills, and to reduce alcohol consumption among individuals whose drinking is associated with cocaine use. Individuals treated with CRA with vouchers were more likely to be retained in treatment, used cocaine at a lower frequency during treatment, and reported a lower frequency of drinking to intoxication during treatment and follow-up compared with patients treated with vouchers only. Those treated with CRA with vouchers also reported a higher frequency of days of paid employment during treatment and the initial 6-month follow-up, decreased depressive symptoms during treatment, and had fewer hospitalizations and legal problems during follow-up (Higgins et al., 2003). Fidelity No information could be found regarding fidelity, or if/how CRA with vouchers was delivered as intended. A study conducted in Spain reported CRA was implemented according to the manual but with one difference: instead of delivering all sessions individually, Secades-Villa et al. (2008) reported sessions were delivered both individually and in groups due to the need to adapt the program to the characteristics of the research site’s Institutional Review Board. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Brooks AC, Ryder D, Carise D, Kirby KC. (2010). Feasibility and effectiveness of computerbased therapy in community treatment. Journal of Substance Abuse Treatment, 39, 227235. Higgins ST, Sigmon SC, Wong CJ, Heil SH, BadgerM GJ, Donham R, et al. (2003). Community reinforcement therapy for cocaine-dependent outpatients. Archives of General Psychiatry, 60, 1043-1052. Roozen HG, Boulogne JJ, van Tulder MW, van den Brink W, De Jong CAJ, and Kerhof JFM. (2004). A systemic review of the effectiveness of the community reinforcement approach in alcohol, cocaine and opioid addiction. Drug and Alcohol Dependence 74, 1–13. Secades-Villa R, García-Rodríguez O, Higgins ST, Fernández-Hermida JR, & Carballo, JL. (2008). Community reinforcement approach plus vouchers for cocaine dependence in a community setting in Spain: Six-month outcomes. Journal of Substance Abuse Treatment, 34, 202-207. Treatment manual: Budney AJ, Higgins ST, Mercer DE, Carpenter G. (1998). A Community Reinforcement Plus Vouchers Approach: Treating Cocaine Addiction. NIDA Therapy Manuals for Drug Addiction No. 2; NIH publication no. 98-4309. Rockville: National Institute on Drug Abuse. http://archives.drugabuse.gov/pdf/CRA.pdf 8. Contingency Management (CM). CM is defined as procedures that aim to alter drug use by systematically arranging consequences that are designed to weaken drug use and strengthen abstinence. The time interval for monitoring for incidences of substance use should be short (e.g., three urine tests per week). Different types of incentives (e.g., cash, vouchers, prizes, or the privilege of taking home doses of methadone) are used in CM to prepare drug users for an abstinent lifestyle (Higgins et al., 2004). Silverman et al., (1996) reported that participants in an abstinent-contingent voucher group gave cocaine-positive urines approximately 40% less often than a random voucher group, suggesting this approach is efficacious for treating cocaine use in a methadone-maintained population. Fidelity Numerous variations in voucher schedules are possible, and some studies report individuals with negative urine tests are eligible to participate in drawings for prizes, rather than receive specific amounts in vouchers. The value of a voucher may escalate with each successive negative urine and can be reset to a lower value following a positive urine test, or a bonus is provided after a certain number of negative urine tests are produced (Prendergast et al., 2006). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Higgins ST, Heil SH, Lussier JP. (2004). Clinical implications of reinforcement as a determinant of substance use disorders. Annual Review of Psychology, 55, 431–61. Prendergast M, Podus D, Finney J, Greenwell L, & Roll J. (2006). Contingency management for treatment of substance use disorders: A meta‐ analysis. Addiction, 101, 1546-1560. Silverman K, Wong CJ, Higgins ST, Brooner RK, Montoya ID, Contoreggi C, et al. (1996). Increasing opiate abstinence through voucher-based reinforcement therapy. Drug and Alcohol Dependence, 41, 157-165. No manual available. 9. Lower-Cost Contingency Management (LCCM). LCCM approaches that use prizes with monetary values of $1–$100 appear to reduce drug use as indicated in studies by Petry et al. (2001; 2002; 2005). Cocaine- and heroin-dependent participants were randomly assigned to a group that was eligible to receive abstinent-contingent prizes or a standard care group (Petry et al., 2002). In the abstinent-contingent prize group, participants who submitted urine samples negative for cocaine and opioids were eligible to draw for prizes of various values. Patients in the prize group condition achieved longer durations of continuous abstinence than patients in the standard treatment condition, and these effects were maintained throughout a 6-month follow-up period. Conversely, LCCM approaches that use reinforcers without monetary value and/or reinforce behaviors other than provision of drug-free urine samples may be promising strategies, but there are no cost-effectiveness data that might persuade policy makers and third-party payers to support these approaches in clinical practice (Carroll & Onken 2005). Fidelity As stated above, numerous variations in voucher schedules and implementation of CM/LCCM are possible, depending on program resources. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Carroll KM, & Onken LS. (2005). Behavioral therapies for drug abuse. American Journal of Psychiatry, 162, 1452-1460. Petry NM, Peirce JM, Stitzer ML, Blaine J, Roll JM., Cohen A, et al. (2005). Effect of prizebased incentives on outcomes in stimulant abusers in outpatient psychosocial treatment programs. Archives of General Psychiatry, 62, 1148-1156. Petry NM, Martin B, Cooney JL, Kranzler HR. (2000). Give them prizes, and they will come: contingency management for treatment of alcohol dependence. Journal of Consulting and Clinical Psychology, 68, 250-257. Petry NM, Martin B. (2002). Low-cost contingency management for treating cocaine- and opioid-abusing methadone patients. Journal of Consulting and Clinical Psychology, 70, 398405. No manual available, for more info see: http://ctndisseminationlibrary.org/display/291.htm 10. Day Treatment with Abstinence Contingencies and Vouchers. This intervention was developed to treat homeless individuals dependent on crack/cocaine. Lunch and transportation were provided, as were individual and group counseling, and multiple psycho-educational and relapse prevention groups. After at least two weeks of abstinence, participants graduated to a 4-month work component that paid wages that could be used to rent inexpensive, drug-free housing. A voucher system also rewarded drug-free related social and recreational activities. Compared to usual care, intervention participants had 36% fewer positive tests for cocaine at 2 months and 18% fewer at 6 months; they were also more likely to be employed and had fewer days of homelessness at follow-up. Fidelity Each component of day treatment was described in a brief program guide, which provided structure for counselors. The guide described the goals of the activities, procedures, and groups. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Milby JB, Schumacher JE, Raczynski JM, Caldwell E, Engle M, Michael M, Carr J. (1996). Sufficient conditions for effective treatment of substance abusing homeless. Drug & Alcohol Dependence, 43, 39-47 Schumacher JE, Milby JB, Caldwell E, Raczynski J, Engle M, Michael M, & Carr J. (1995). Treatment outcome as a function of treatment attendance with homeless persons abusing cocaine. Journal of Addictive Diseases, 14, 73-85. No manual available. 11. Group Drug Counseling (GDC) for Cocaine Addiction: The Collaborative Cocaine Treatment Study Model (CCTS). GDC involves 24 group therapy sessions during a 6-month period in two phases. Phase 1 is structured and psycho-educational in nature, and provides an overview of the key issues in early recovery related to addiction, the recovery process, and relapse prevention. In Phase II, a more “open” problem-solving approach is used to discuss current concerns and problems, and clients set the agenda for discussion during each group session. Although the CCTS study found that individual drug counseling (IDC), cognitive therapy, and other treatments helped patients improve, the combination of IDC and GDC produced the best results in terms of reductions in cocaine and other drug use (Crits-Christoph et al., 1999). Fidelity Extensive attention was paid to selection, training, and competence of each counselor delivering the intervention. Assessments of treatment fidelity and discrimination were obtained during the training phase and the main trial using independent audiotape ratings. Training phase data indicated that the treatments were implemented as intended and that the treatment conditions could be readily differentiated (Crits-Christoph et al., 1999). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Crits-Christoph P, Siqueland L, Blaine J, Frank A, Luborsky L, Onken LS, et al. (1999). Psychosocial treatments for cocaine dependence: Results from the NIDA collaborative cocaine treatment Study. Archives of General Psychiatry, 56, 493-502. Crits-Christoph P, Siqueland L, McCalmont E, Gastriend DR, Frank A, Moras K, et al. (2001). Impact of psychosocial treatments on associated problems of cocaine-dependent patients. Journal of Consulting and Clinical Psychology, 69, 825-830. Treatment manual: Daley DC, Mercer DE, & Carpenter G. (2002). Drug Counseling for Cocaine Addiction: The Collaborative Cocaine Treatment Study Model. US Department of Health and Human Services, National Institutes of Health, National Institute of Drug Abuse. http://archives.drugabuse.gov/pdf/Manual4.pdf 12. Individual Drug Counseling Approach to Treat Cocaine Addiction (IDC): The Collaborative Cocaine Treatment Study Model (CCTS). IDC is a drug counseling approach that focuses on the symptoms of drug addiction and related areas of impairment, and the content and structure of the patient's ongoing recovery program. It gives the patient coping strategies and tools for recovery and promotes 12-step ideology and participation. The goals are to assist patients in achieving and maintaining abstinence from addictive chemicals and behaviors, and to help them recover from the damage the addiction has caused in their life. IDC consists of 36 sessions over 6 months (approximately 45 minutes each) during the active treatment phase and then once-a-month follow-up sessions for 3 months. As noted with GDC, the researchers with the CCTS study reported IDC and other treatments helped patients significantly reduce cocaine and other drug use; however, the combination of IDC and GDC produced the best results (Crits-Christoph et al, 1999) Fidelity: Barber et al. (1996) developed a seven-point fidelity scale for IDC. Three raters assessed 43 items based on the main components described in the treatment manual. These measures were used to assess both adherence (i.e., extent to which intervention components are delivered as prescribed in the treatment manual), and competence (i.e., qualitative measure of the skillfulness in which intervention components are delivered). Rater training included a practice period during which raters met weekly to rate 72 tapes, followed by discussion about how they were using the scale. Raters then rated 62 new tapes in order to assess interrater reliability. Overall, intraclass correlation coefficients for adherence and competence ratings were acceptable. Adherence to IDC was associated with better drug use outcomes only when the therapeutic alliance was low (Barber et al., 2006). References reporting improved client outcomes: (See references under #11, GDC) Treatment manual: Mercer DE, & Woody GE. (1999). An Individual Drug Counseling Approach to Treat Cocaine Addiction: The Collaborative Cocaine Treatment Study Model. US Department of Health and Human Services, National Institutes of Health, National Institute of Drug Abuse. http://archives.drugabuse.gov/pdf/Manual3.pdf 13. Matrix Intensive Outpatient Program for Treatment of Stimulant Abuse The Matrix Model is a treatment approach for stimulant use disorders that was developed through 20 years of experience in real-world treatment settings. This approach consists of relapse-prevention groups, education groups, social-support groups, individual counseling, and urine and breath testing delivered over a 16-week period. Participants also become familiar with self-help programs. Matrix participants were 38% more likely to stay in treatment and 27% more likely to complete treatment compared with participants receiving treatment as usual; stimulant use in the past 30 days declined from an average of 11 days at the beginning of treatment to 4 days at treatment discharge (Rawson et al., 1995, 2004). Fidelity Staff trained to deliver the Matrix Model received an initial 40 hours of didactic and experiential training. Clinical supervisors conducted booster training sessions at each site, led mandatory weekly teleconferences with Matrix clinicians, monitored clinician performance via a weekly activity checklist, reviewed a sample of tape-recorded sessions and provided feedback regularly to ensure that the Matrix Model was implemented as designed. Two fidelity scales were developed to assess adherence to the treatment protocol. Data from Year 2 of the study found that sites adhered to the Matrix Model protocol in implementation of critical elements (Rawson et al., 2004). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Rawson RA, Marinelli-Casey P, Anglin MD, Dickow A, Frazier Y, Gallagher C, et al. (2004). A multi-site comparison of psychosocial approaches for the treatment of methamphetamine dependence. Addiction, 99, 708-717. Rawson RA, Shoptaw SJ, Obert JL, McCann MJ, Hasson AL, Marinelli-Casey PJ, et al. (1995). An intensive outpatient approach for cocaine abuse treatment: The Matrix model. Journal of Substance Abuse Treatment, 12, 117-127. Treatment manual: The Matrix Institute, Obert JL, Rawson, R, McCann MJ, Ling W. (2005). The Matrix Model Therapist's Manual, A 16-week Individualized Program. Center City, MN: Hazelden Publishing. Some manuals and materials are available free of charge; others may be purchased at www.hazelden.org. For more information about treatment manuals: http://www.matrixinstitute.org/training/manuals.html 14. Motivational Enhancement Therapy (MET). MET is an adaptation of motivational interviewing (MI) that includes normative assessment feedback to clients that is presented and discussed in a non-confrontational manner. This approach is a goal-oriented, client-centered counseling style for facilitating behavior change by helping clients resolve ambivalence across a range of problematic behaviors. MET uses an empathic and strategic approach in which the therapist provides feedback that is intended to strengthen and consolidate the client's commitment to change and promote a sense of self-efficacy. As noted under TSF and CBT, participants in all Project MATCH conditions, including MET showed significant reductions in drinking (Project MATCH Research Group, 1998). Further study shows this approach is associated with reductions in alcohol and drug use during treatment and 12 weeks after treatment, as well as improvements in social functioning (Ball et al., 2007). Fidelity: Over 80 therapists from diverse backgrounds received careful training and supervision using Project MATCH structured manuals and were able to implement these treatments successfully and with fidelity (Project MATCH Research Group, 1998). However, more recently, Madsen et al. (2005) found variability in studies employing motivational interviewing (MI) approaches with regard to the training, supervision, and monitoring of therapists delivering the intervention. This finding is problematic given the concerns of some researchers that MI is sometimes implemented in a fashion that violates the spirit of the approach; consequently, instruments that assess adherence to MI approaches are being developed (Madsen et al., 2006). Martino et al. (2008) found that greater adherence to MET was associated with significant, although modest, client process and outcome variables, and a higher rate of negative drug screens during treatment was found for clients whose counselor demonstrated better adherence to the MET protocol. References reporting improved client outcomes: Ball SA, Martino S, Nich C, Frankforter TL, van Horn D, Crits-Christoph P, et al. (2007). Site matters: Multisite randomized trial of motivational enhancement therapy in community drug abuse clinics. Journal of Consulting and Clinical Psychology, 75, 556-567. Project MATCH Research Group. (1997). Matching alcoholism treatments to client heterogeneity: Project MATCH posttreatment drinking outcomes. Journal of Studies on Alcohol, 58, 7-29. Treatment manual: Miller WR, Zweben A, DiClemente CC, Rychtarik RG. (1994). Motivational Enhancement Therapy Manual: A Clinical Research Guide for Therapists Treating Individuals with Alcohol Abuse and Dependence. Project MATCH Monograph Series, Vol. 2; DHHS Publication No. 943723. Rockville, MD: NIAAA, 1994. http://lib.adai.washington.edu/pubs/match2/match2.pdf 15. Mapping-Enhanced Counseling (formerly “Node-Link Mapping”). This strategy involves the counselor and client developing visual representations, or maps, of issues that emerge in SUD treatment. Drawing a map or diagram can help clients see and understand relationships between their actions and consequences and can help them express complex relationships and parallel ideas that are difficult to verbalize. As a therapeutic tool, it helps address problems more clearly than when relying strictly on verbal skills. Clients who received this approach significantly decreased their opiate and cocaine use and had fewer positive urine samples overall than clients receiving standard counseling; they also were less likely to have used a dirty needle at 6-month follow-up (Dansereau et al., 1996). In addition, clients assigned to mapping-enhanced counseling missed fewer scheduled sessions than standard counseling clients in the first 6 months of treatment (Newbern et al., 2005). Fidelity: The training included a series of workshops during which counselors practiced using mapping and received training in the use of the manual. Mapping procedures were monitored and observed periodically by the training staff to assure that mapping was implemented adequately (Dansereau, et al., 1996). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Dansereau DF, Joe GW, Dees SM, & Simpson DD. (1996). Ethnicity and the effects of mapping-enhanced drug abuse counseling. Addictive Behaviors, 21(3), 363-376. Joe GW, Dansereau DF, Pitre U, & Simpson DD. (1997). Effectiveness of node-link mapping enhanced counseling for opiate addicts: A 12-month post treatment follow-up. Journal of Nervous and Mental Disease, 185, 306-313. Newbern D, Dansereau DF, Czuchry M, & Simpson DD. (2005). Node-link mapping in individual counseling: Treatment impact on clients with ADHD-related behaviors. Journal of Psychoactive Drugs, 37, 93-103. Treatment manual: Dansereau DF, Dees SM, Chatham LR, Boatler JF, & Simpson DD. (August 1993) Mapping New Roads to Recovery. Texas Institute of Behavioral Research at Texas Christian University (TCU). http://ibr.tcu.edu/wp-content/uploads/sites/2/2013/09/mappingall.pdf 16. Relapse Prevention Therapy (RPT). RPT is a behavioral self-control program that teaches individuals with substance addiction how to anticipate and cope with the potential for relapse. RPT can be used as a stand-alone SUD treatment or as an aftercare program to sustain gains achieved during initial SUD treatment. Coping skills training is the cornerstone of RPT. A metaanalysis found RPT was most effective when applied to alcohol or polysubstance use disorders, and combined with the adjunctive use of medication (Irvin et al., 1999). Overall, many basic tenets of the RPT model have received support, and findings regarding its clinical effectiveness have generally been supportive (Hendershot et al., 2011). Effectiveness of RPT in reducing the frequency of relapse episodes as well as the intensity of lapse and/or relapse episodes among people who resumed alcohol use after treatment has been reported (Larimer et al., 1999). Fidelity In a study of RTP for cocaine dependence, all therapists received extensive training in RTP that included a 2-day didactic seminar and successful completion of at least one closely supervised training case. To promote adherence to manual guidelines and prevent drift through the main phase of the study, therapists met weekly with study investigators to discuss case material and review session videotapes (Carroll et al., 1999). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Carroll KM, Rounsaville BJ, Nich C, Gordon LT, Wirtz PW, & Gawin F. (1994). One-year followup of psychotherapy and pharmacotherapy for cocaine dependence: delayed emergence of psychotherapy effects. Archives of General Psychiatry, 51, 989-997. Hendershot CS, Witkiewitz K, George WH, Marlatt GA. (2011). Relapse prevention for addictive behaviors. Substance Abuse Treatment Prevention and Policy, 6, 17. Larimer ME, Palmer RS, Marlatt GA. (1999). Relapse prevention: An overview of Marlatt’s cognitive-behavioral model. Alcohol Research and Health, 23, 151-160. Treatment manual: Marlatt GA, Parks GA, and Witkiewitz K. (December 2002). Clinical Guidelines for Implementing Relapse Prevention Therapy: A Guideline Developed for the Behavioral Health Recovery Management Project. Addictive Behaviors Research Center, University of Washington, Seattle. http://www.bhrm.org/guidelines/RPT%20guideline.pdf 17. Seeking Safety. Seeking Safety is a present-focused treatment for clients with a history of trauma and substance abuse for use in groups or individual treatment, with male and female clients, and in a variety of settings. This approach focuses on safety as the overarching goal (helping clients attain safety in their relationships, thinking, behavior, and emotions) and integrated SUD/PTSD treatment. Compared with women in a treatment-as-usual condition, women who participated in Seeking Safety significantly reduced their substance use at the end of treatment and at the 6-month follow-up (Hien et al., 2004). Another study found that substance use outcomes were improved but were not significantly different over time for women receiving the Seeking Safety intervention compared to those who received a treatmentas-usual intervention called "Women's Health Education" (Hien et al, 2009). Fidelity All counselors and supervisors attended a comparable centralized 3-day workshop, and supervisors received another half day of training focused on how to carry out supervision. An expert from the lead training team rated the videotaped certification sessions for adherence to the manual and competency in the delivery of the interventions. The supervisors used the certification sessions to obtain interrater reliability with the lead expert trainers on the adherence measures (Hien et al., 2009). Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Hien D, Wells EA, Jiang H, Suarez-Morales L, Campbell AN, Cohen LR, et al. (2009). Multisite Randomized Trial of Behavioral Interventions for Women with Co-Occurring PTSD and Substance Use Disorders. Journal of Consulting and Clinical Psychology, 77, 607-619. Hien DA, Cohen LR, Miele GM, Litt LC, & Capstick C. (2004). Promising treatments for women with comorbid PTSD and substance use disorders. American Journal of Psychiatry, 161, 1426-1432. Holdcraft LC, & Comtois KA. (2002). Description of and preliminary data from a women's dual diagnosis community mental health program. Canadian Journal of Community Mental Health, 21, 91-109. Treatment manual: Najavits LM. (2002). Seeking Safety: A treatment manual for PTSD and substance abuse. New York: Guilford Press. http://www.seekingsafety.org/ 18. Supportive-Expressive Psychotherapy (SE). SE is an analytically oriented, time-limited psychotherapy that has been adapted for use with individuals with heroin and cocaine addiction. Particular emphasis is given to themes related to drug dependence, the role of drugs in relation to problem feelings and behaviors, and alternative, drug-free means of resolving problems. Relative to individuals who received drug counseling, those who received SE reported fewer days of opiate and sedative use and were able to take a lower dose of methadone at follow-up (Luborsky et al., 1985). Fidelity The SE treatment manual was used in both the initial training and in the continuing supervision of all psychotherapists. The SE therapists were supervised weekly in a group by Dr. Luborsky for the first two thirds of the study and then biweekly. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Luborsky L, McLellan, AT, Woody GE, O'Brien CP, & Auerbach A. (1985). Therapist success and its determinants. Archives of General Psychiatry, 42, 602-611. Woody GE, Luborsky L, McLellan AT, O'Brien CP, Beck AT, Blaine J, et al. (1983). Psychotherapy for opiate addicts: Does it help? Archives of General Psychiatry, 40, 639645. Treatment manual: Luborsky L. (2000). Principles of Psychoanalytic Psychotherapy: A Manual for SupportiveExpressive (SE) Treatment. New York: Basic Books. 19. Boston Consortium Model (BCM): Trauma-Informed Substance Abuse Treatment for Women. This program provides a fully integrated set of substance abuse treatment and trauma-informed mental health services to low-income, minority women with co-occurring alcohol/drug addiction, mental disorders, and trauma histories. The treatment provider develops an integrated, trauma-informed treatment plan for the client, links her to the appropriate mental health services, and works collaboratively as the primary point of contact with the client's mental health and SUD treatment service teams. Additionally, BCM uses five manual-driven, skills-building group modules. Women in the BCM condition reported significantly lower illicit drug use, mental health symptoms, and HIV risk behaviors than a treatment-as-usual group (Amaro et al., 2007). Fidelity Staff who participated received in-depth staff training on trauma informed care, links between trauma, mental illness and SUDs, and trauma specific intervention. Fidelity requirement for improved outcomes not found. References reporting improved client outcomes: Amaro H, Dai J, Arevalo S, Acevedo A, Matsumoto A, Nieves R, et al. (2007). Effects of integrated trauma treatment on outcomes in a racially/ethnically diverse sample of women in urban community-based substance abuse treatment. Journal of Urban Health, 84, 508522. Amaro H, Larson MJ, Zhang A, Acevedo A, Dai J, & Matsumoto A. (2007). Effects of trauma intervention on HIV sexual risk behaviors among women with co-occurring disorders in substance abuse treatment. Journal of Community Psychology, 35, 895-908. Amaro H, Chernoff M, Brown V, Arévalo S, & Gatz M. (2007). Does integrated trauma-informed substance abuse treatment increase treatment retention? Journal of Community Psychology, 35, 845-862. Amaro H, McGraw S, Larson MJ, Lopez L, Nieves R, Marshall B. (2004). Boston Consortium of Services for Families in Recovery: a trauma-informed intervention model for women’s alcohol and drug addiction treatment. Alcoholism Treatment Quarterly, 22, 95–119. Treatment manual: Amaro, H, Melendez, MP, Melnick, S, and Nieves, RL. (2005). Integrated Substance Abuse, Mental Health and Trauma Treatment with Women: A case study workbook for staff training. Boston Consortium of Services for Families in Recovery, Public Health Commission, Boston, MA. http://www.bphc.org/whatwedo/AddictionServices/Documents/Curricula/Intergrated%20Substance%20Abuse%20EN.pdf APPENDIX II About the Evidence-Based Practice Matrix The matrix is a modified version of the Evidence-Based Practices for Treating Substance Use Disorders: Matrix of Interventions, which was developed as a joint project of the University of the Washington Alcohol & Drug Abuse Institute (ADAI) and the Northwest Frontier Addiction Technology Transfer Center. The ADAI matrix can be accessed from: Institute http://adai.washington.edu/ebp/matrix.pdf Links to the developers, summaries, intervention details, training/technical assistance, supporting references, and treatment manuals (when available) are embedded within this matrix. The following sources were used to determine which practices to include in the ADAI matrix. Knowledge Application Program (KAP) of the Center for Substance Abuse Treatment. This program produces, markets, and distributes knowledge about best treatment practices by putting it in the hands of providers who help individuals seeking substance abuse treatment. Miller WR, Wilbourne PL, Hettem JE. "What Works? A Summary of Alcohol Treatment Outcome Research." In: Hester, Reid K; Miller, William R (eds.) Handbook of Alcoholism Treatment Approaches: Effective Alternatives (3rd ed.). Boston : Allyn and Bacon, 2003. pp.13-63. National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A ResearchBased Guide (1999). This guide was developed after NIDA's National Conference on Drug Addiction Treatment: From Research to Practice in April 1998. It is designed to help foster more widespread use of scientifically based treatment components. Onken, Lisa. Effective Behavior Therapies for Treatment of Drug Abuse. (Unpublished document). Bethesda, MD: Behavioral Treatment Development Branch National Institute on Drug Abuse (NIDA). SAMHSA's National Registry of Evidence-based Programs and Practices (NREPP). A searchable database of interventions for the prevention and treatment of mental and substance use disorders. http://nrepp.samhsa.gov/ APPENDIX III Evidence-based practices as adjunctive treatments (for issues/concerns other than SUD) Although the following EBPs were not developed to treat SUD, these treatments address concerns relevant to many individuals with SUD. For more information about these treatments, go to http://adai.washington.edu/ebp/matrix.pdf and click on the specific treatment. Updated links to manuals are provided below. Time Out! for Me: An Assertiveness and Sexuality Workshop Designed for Women This intervention, which was developed for the TCU/DATAR project, was designed to help counselors work with sexually active women to improve their self-esteem, interpersonal communication skills, and comfort with sexuality. These are important issues for increasing women’s acceptance of safer sex choices and healthier sexual life-styles, and may help reduce their risk of HIV infection from sexual behaviors. Treatment manual: http://www.ibr.tcu.edu/pubs/trtmanual/tofm.html Time Out! for Men: A Communication Skills and Sexuality Workshop Designed for Men. This intervention provides guidelines for leading an 8-session workshop for men who are interested in improving their intimate relationships. Communication skills, self-esteem, sexual health, and conflict resolution skills are presented as a foundation for helping men find solutions to relationship difficulties. Treatment manual: http://www.ibr.tcu.edu/pubs/trtmanual/tofmen.html Anger Management for Substance Abuse and Mental Health Clients: Cognitive-Behavioral Therapy Anger Management is based on social learning theory; it may be useful for counselors who work with substance abuse and mental health clients with concurrent anger problems. Treatment manual: http://store.samhsa.gov/shin/content//SMA13-4213/SMA13-4213.pdf Moral Reconation Therapy [Reconation meaning “the conscious process of decision-making”] This is a systematic treatment strategy that seeks to decrease recidivism among criminal offenders by increasing moral reasoning. Its cognitive-behavioral approach combines elements from a variety of psychological traditions to progressively address ego, social, moral, and positive behavioral growth. Treatment manual: http://www.moral-reconation-therapy.com/ Holistic Health Recovery Program (HHRP, formerly Holistic Harm Reduction Program) HHRP is an HIV prevention and management intervention dedicated to harm reduction, health promotion, and improved quality of life for individuals addicted to illicit drugs. It utilizes cognitive remediation strategies (e.g., multimodal presentation of material) to facilitate acquisition and retention of new harm reduction skills. The group treatment manual, handouts, and client workbook are all available free of charge at the link below; slides are available for a fee. This program provides separate HHRP manuals for individuals of negative or unknown HIV serostatus and individuals who know their serostatus is HIV positive. Treatment manual: http://medicine.yale.edu/spiritualselfschema/training/hhrp/hhrpgroup.aspx APPENDIX IV Articles Reporting Fidelity Research on Evidence-Based Practices Barber JP, Gallop R, Crits-Christoph P, Frank A, Thase M, Weiss RD, et al. (2006). The role of therapist adherence, therapist competence, and alliance in predicting outcome of individual drug counseling: results from the National Institute on Drug Abuse Collaborative Cocaine Treatment Study. Psychotherapy Research, 16, 229–240. Barber JP, Mercer D, Krakauer I, Calvo N. (1996). Development of an adherence/competence rating scale for individual drug counseling. Drug and Alcohol Dependence, 43, 125–132. Barber JP, Sharpless BA, Klosterman S, McCarthy KS. (2007). Assessing intervention competence and its relation to therapy outcome: a selected review derived from the outcome literature. Professional Psychology: Research and Practice, 38, 493–500. Carroll KM, & Onken LS. (2005). Behavioral therapies for drug abuse. American Journal of Psychiatry, 162, 1452-1460. Guydish J, Campbell BK, Manuel JK, Delucchi KL, Le T, Peavy KM, & McCarty D. (2014). Does treatment fidelity predict client outcomes in 12-Step Facilitation for stimulant abuse? Drug and Alcohol Dependence, 134, 330-336. Hogue A, Henderson CE, Dauber S, Barajas PC, Fried A, Liddle HA. (2008). Treatment adherence, competence, and outcome in individual and family therapy for adolescent behavior problems. Journal of Consulting and Clinical Psychology, 76, 544–555. Madson MB, & Campbell TC. (2006). Measures of fidelity in motivational enhancement: A systematic review. Journal of Substance Abuse Treatment, 31, 67-73. Martino S, Ball SA, Nich C, Frankforter TL, Carroll KM, (2008). Community program therapist adherence and competence in motivational enhancement therapy. Drug and Alcohol Dependence, 97, 37–48. Sholomskas, DE, & Carroll, KM. (2006). One small step for manuals: Computer-assisted training in twelve-step facilitation. Journal of Studies on Alcohol, 67, 939-947. Sholomskas DE, Syracuse-Siewert G, Rounsaville BJ, Ball SA, Nuro KF, & Carroll KM. (2005). We don't train in vain: a dissemination trial of three strategies of training clinicians in cognitivebehavioral therapy. Journal of Consulting and Clinical Psychology, 73, 106-112.