Globalization and Health
advertisement

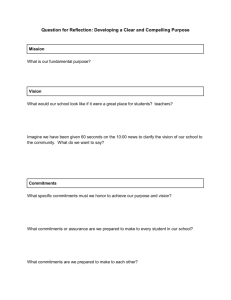
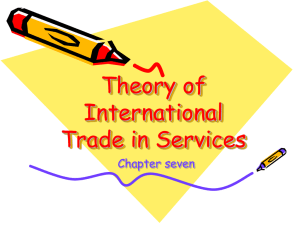
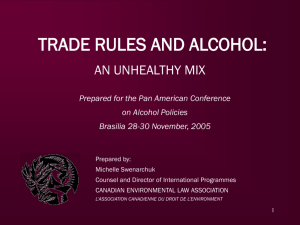
Lecture 18: Globalization and Health Richard Smith Reader in Health Economics School of Medicine, Health Policy & Practice Health Economics – SOCE3B11 – Autumn 04/05 Overview of lecture • • • • What is globalization? Relationship between globalization and health Aspects of globalization that may effect health Health, international trade and WTO – Trade in health services and GATS What is ‘Globalization’? • Easier travel & communication • Mixing of customs & cultures • Integration of national economies (removal of barriers to international trade & finance) – ‘liberalization’ or ‘openness’ • Means cannot view national health, interventions and policies in isolation from: – other countries – other sectors (e.g. travel, finance) Globalization economic opening goods, services, capital, people, ideas, information cross-border flows international rules and institutions national economy and health-related sectors risk factors household economy HEALTH health services Aspects of Globalization that may effect Health • General effect on health from changes in national economic growth – link between ‘health and wealth’ • Environmental degradation (e.g. air, water pollution) • Improved access to knowledge and technology • Marketing of harmful products & unhealthy behaviours • Conflict & security • Cross-border transmission of disease Emerging/re-emerging infectious diseases 1996 to 2003 Legionnaire’s Disease Multidrug resistant Salmonella Cryptosporidiosis E.coli O157 SARS BSE E.coli non-O157 Typhoid Malaria E.coli O157 nvCJD Lyme Borreliosis Venezuelan Equine Encephalitis Dengue haemhorrhagic fever West Nile Virus Reston virus Lassa fever Yellow fever Diphtheria West Nile SARS Influenza (H5N1) Fever Echinococcosis W135 Nipah Virus Buruli ulcer Ebola haemorrhagic fever Cholera Cholera 0139 RVF/VHF O’nyongnyong fever Reston Virus Dengue haemhorrhagic fever Human Monkeypox Cholera Equine morbillivirus Ross River virus Hendra virus Economic impact, selected infectious disease outbreaks, 1990–1999 USA—E. coli 0157 Food recall/ destruction Periodic UK—BSE US$ > 9 billion 1990-1998 HONG KONG SAR Influenza A (H5N1) Poultry destruction, 1997 INDIA—Plague US$ 1.7 billion, 1995 PERU—Cholera Seafood Export Barriers 1991 UR TANZANIA Cholera US$ 36 million 1998 MALAYSIA—Nipah Pig destruction, 1999 World Health Organization Health and International Trade • Context: Effects of trade liberalisation on public health • Trade liberalisation: removal of impediments to trade in goods and services (especially via WTO) • Public health: organised measures (public &/or private) to prevent disease, promote health or prolong life of the population as a whole Specific Public Health Issues • • • • • • • • Infectious disease control Food safety Tobacco Environment Access to drugs Food security Emerging issues (biotechnology….) Health services WTO Agreements • • • • Goods: GATT Technical barriers to trade: SPS, TBT Intellectual property and trade : TRIPS Services: GATS Specific Health Issues and most relevant WTO Agreements WTO AGREEMENTS HEALTH ISSUES Infectious Disease Control Food Safety Tobacco Control Environment Access to Drugs Health Services Food Security Emerging Issues Biotechnology Information Technology Traditional Knowledge SPS TBT * * * * * * TRIPS GATS * * * * * * * * * * Trade in Health Services/GATS: Background • International trade growing, & trade in services is increasing percentage of this overall growth • Of this trade, health sector is already affected by liberalization in other areas (e.g. finance) • Many countries see health as a sector where they may have a comparative trade advantage • More countries seeking to ascend to WTO and therefore make commitments under GATS General Agreement on Trade in Services (GATS) • GATS emerged from 1994 Uruguay Round of negotiations that created the WTO (Members agree to progressive liberalization) Subject services trade to ‘same’ treatment as goods (GATT) Basis = liberalization increases global efficiency (comparative advantage – lower cost, higher quality, innovation) Provides multilateral legal framework for liberalizing international services trade (based on existing int. trade law) • Debate is polarized - “Tale of Two Treaties” GATS is worst of treaties – undermines national sovereignty GATS is best of treaties – increase health (sovereignty) The House that GATS Built Trade Liberalization Preservation of the Right to Regulate Services Multilateral Framework Side Wall: Market Access Commitments Back Wall: Exceptions GATS (Services) Front Wall: General Obligations and Disciplines Side Wall: National Treatment Commitments GATS Council Floor: Dispute Settlement GATS Timetable • 1994 ‘Uruguay Round’ of WTO negotiations saw initial commitments in health services made by a handful of countries • Current negotiations began following WTO meeting in February 2000: – initial requests for specific commitments made by end June 2002 – initial offers due by end of March 2003 – finalised agreement by end of January 2005 The GATS Process • Countries (via MoT) select service sector(s) they wish to open to foreign suppliers • A ‘commitment’ is then made within this sector – within each mode individually or combined – stating limitations to how much access foreign providers are allowed • Commitments are multilateral – no ‘favourites’ Key Aspects of GATS • Creates ‘binary’ system – either solely public provided (hence not covered by GATS) or not • Commitments potentially irreversible – changes possible (> 3 years) but entail ‘compensation’ (offering new commitments in other sectors with a view to restoring the balance of commitments which existed prior to the modification) • GATS excludes “services supplied in the exercise of governmental authority” – debate on coverage • MFN principle • Structure – four ‘modes of supply’ S T A R T Threshold Question: Does GATS Apply? Is the health-related service supplied by the government? No Yes Yes Is the health-related service supplied on a commercial basis? Yes No Is the health-related service supplied in competition with one or more service providers? No GATS does not apply Is the health-related service supplied by a private actor pursuant to delegated governmental authority? Yes No GATS applies to measures of WTO members that affect trade in health-related services Structure of GATS: Four ‘Modes of Supply’ 1. 2. 3. 4. Cross border delivery (e-health) Consumption abroad (movt. of patients) Commercial presence (FDI hospitals) Movement of personnel (doctors abroad) Mode 1: Cross border delivery of services • Shipment of laboratory samples, diagnosis and clinical consultations by mail • E-health – – – – – Telediagnostic Telesurveillance Teleconsultation Teletreatment Teleproducts (especially phamaceuticals) Mode 1 Opportunities • Enable health care delivery to remote and underserviced areas – promoting equity • Alleviate (some) human resource constraints • Enable more cost-effective disease surveillance • Improve quality of diagnosis and treatment • Upgrade skills, disseminate knowledge through interactive electronic means Mode 1 Risks • Relies on telecommunications and power sector infrastructure • Capital intensive, possible diversion of resources from basic preventive and curative services • Equity issue if it caters to a small segment of the population - urban affluent Mode 2: Consumption abroad • Movement of patients from home country to the country providing the diagnosis/treatment • Movement of health professionals from home to another country to receive medical education and training Mode 2 Opportunities For exporting countries • Generate foreign exchange earnings to increase resources for health • Upgrade health infrastructure, knowledge, standards and quality For importing countries • Overcome shortages of physical and human resources in speciality areas • Receive more affordable treatment Mode 2 Risks • Create dual market structure • May crowd out local population – unless these services are made available to local population • Diversion of resources from the public health system • Outflow of foreign exchange for importing countries Mode 3: Commercial presence • Establishment of hospitals, clinics, diagnostic and treatment centres and nursing homes and training facilities through foreign direct investment – cross border mergers/acquisitions, joint venture/alliance • Opportunities for foreign commercial presence also in management of health facilities and allied services, medical and paramedical education, IT and health care Mode 3 Opportunities • Generate additional resources for investment in upgrading of infrastructure and technologies • Reduce the burden on public resources • Create employment opportunities • Raise standards, improve management, quality , improve availability, improve education (foreign commercial presence in medical education sector) Mode 3 Risks • Large initial public investments to attract FDI • If public funds/subsidies used - potential diversion of resources from the public health sector • Two tier structure of health care establishments • Internal brain drain from public to private sector • Crowding out of poorer patients, cream skimming phenomena Mode 4: Movement of Health Professionals • Includes doctors, nurses, paramedics, midwives, consultants, trainers, management personnel • Factors driving cross border movements wage differentials between countries search for better working conditions/standards of living search for greater exposure/training/qualifications demand and supply imbalances between countries • Approach towards mode 4 trade in health services by exporting and receiving countries varies - some countries encourage outflow, others create impediments Mode 4 Opportunities From sending country • Promote exchange of knowledge among professionals • Upgrade skills and standards (provided service providers return to the home country) • Gains from remittances and transfers From host country • Meet shortage of health care providers, improve access, quality and contain cost pressures Mode 4 Risks From sending country • Permanent outflows of skilled personnel ‘brain drain’ • Loss of subsidised training and financial capital invested • Adverse effects on equity, availability and quality of services Tourism/Courier Transportation Others Culture & sport Health & Social services Education Finance Construction Distribution Environment Telecommunication Business specific commitments Scope of analysis National treatment Market access Cross-industrial commitment 1-4 = modes 1 2 3 4 1 2 3 4 Status of GATS Commitments (No. WTO Members by Sector) 100 50 0 t l ism ancia siness ations sport ucti on ati on nmen alth bution cation r e u e n H i r c r u ro To Bu Fin uni Tra Const Ed istr Rec Envi D m m Co Commitments of WTO Members in Health Services Number of WTO Members number (~2004) with commitments in health (developed/developing): Medical/dental services 62 (18/44) (excl. USA) Nurses/midwives 34 (17/17) (excl.USA) Hospital services 52 (15/37) (incl. USA) Other human health 22 (2/20) (excl. USA & EC) No commitments at all 39 (e.g. Canada, Brazil) Commitments – Market Access Mode 1 Mode 2 Medical and Midwives, Hospital Other Human Dental Services Nurses, etc. Services Health Services Full 21 (4/17) 8 (2/6) 18 (0/18) 11 (0/11) Partial 12 (1/11) 6 (1/5) 1 (0/1) 1 (0/1) Unbound 29 (13/16) 20 (14/6) 35 (15/20) 10 (2/8) Full 35 (5/30) 12 (2/10) 44 (14/30) 15 (0/15) Partial 24 (13/11) 21 (15/6) 5 (1/4) 5 (2/3) 3 (0/3) 1 (0/1) 3 (0/3) 2 (0/2) Full 29 (13/16) 7 (2/5) 18 (0/18) 12 (0/12) Partial 26 (4/22) 25 (15/10) 31 (15/16) 9 (2/7) Unbound 7 (2/5) 2 (0/2) 3 (0/3) 1 (0/1) Full 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 56 (16/40) 32 (17/15) 48 (14/34) 21 (2/19) 6 (2/4) 2 (0/2) 4 (1/3) 1 (0/1) Unbound Mode 3 Mode 4 Partial Unbound Commitments – National Treatment Mode 1 Mode 2 Medical and Midwives, Hospital Other Human Dental Services Nurses, etc. Services Health Services Full 24 (4/20) 9 (2/7) 21 (0/21) 12 (0/12) Partial 10 (1/9) 6 (1/5) 1 (0/1) 1 (0/1) Unbound 28 (13/15) 19 (14/5) 30 (15/15) 9 (2/7) Full 34 (5/29) 12 (2/10) 44 (14/30) 15 (0/15) Partial 23 (13/10) 21 (15/6) 5 (1/4) 5 (2/3) 5 (0/5) 1 (0/1) 3 (0/3) 2 (0/2) Full 19 (1/18) 10 (2/8) 33 (13/20) 11 (0/11) Partial 37 (16/21) 22 (15/7) 15 (2/13) 9 (2/7) Unbound 6 (1/5) 2 (0/2) 4 (2/2) 2 (0/2) Full 3 (0/3) 1 (0/1) 3 (0/3) 1 (0/2) 54 (17/37) 31 (17/14) 44 (14/30) 19 (2/17) 5 (1/4) 2 (0/2) 5 (1/4) 2 (0/2) Unbound Mode 3 Mode 4 Partial Unbound Summary of GATS Commitments • Generally, number of sectors committed positively related to the level of economic development • But - pattern in health services less clear – Far more developing than developed country commitments • E.g Canada no commitments, USA/Japan only one whereas LDCs (Burundi, Gambia, Zambia etc) have 3 or 4 subsectors – Of 4 subsectors – medical/dental most heavily committed (62), followed by hospital (52). – Highest share of full market access recorded for mode 2 – Developed countries use limitations on modes 2 & 3 more than developing countries – No Member undertaken full commitments for mode 4 (highly restricted area) GATS – 3 Key Questions • Why are current levels of trade in health services low? – presence of government monopolies – likely to be rare – no ‘pace setters’ in health (c.f. telecommunications/financial services) – different ‘economic’ value (c.f. telecommunications/financial services) • How will GATS effect a country’s health sovereignty/system? – depends on interpretation of “commercial basis” and “in competition” – general obligations – MFN, pursuing increased liberalization, exception for measures ‘necessary’ to protect health’, dispute settlement – horizontal commitments made for other sectors • What effect might liberalization have on national health/wealth? – currently data free environment – even extent of ‘openness/liberalization’! – research required on impact of liberalization on: population health status, distribution of health services/status, economic factors (GDP, BoP etc) and how GATS compares with other agreements Further References • See references for Seminar 6 • Smith RD. Foreign direct investment and trade in health services: a review of the literature. Social Science and Medicine, 2004; 59: 2313-2323. • For future ref: – Blouin C, Drager N, Smith RD (eds). Trade in Health Services, developing countries and the GATS. Oxford University Press (in press). – Smith RD. Trade in Health Services: Current Challenges and Future Prospects of Globalisation. In: Jones AM (ed). Elgar Companion to Health Economics. Edward Elgar (in press).