Advancing the Vision of the Neurological Institute
Patient Experience 2014
Julie Fussner BSN, RN, CPHQ, SCRN
Advancing the Vision of the Neurological Institute
Patient Experience
• April 26, 2012
• 49 yo F Hx: HTN, Bipolar
• 10:20 L weakness, slurred speech, and collapsed at
Vet’s office
• Taken to OSH – arrived at 10:40
• VS: B/P 159/63 HR 120, R 20 BS 138
• NIHSS=10
• CT small right parietal hypodensity – did not explain
symptoms
• UH transfer center called and IV tPA recommended
• 11:20 IV tPA started (Door to drug = 40 mins)
2
Advancing the Vision of the Neurological Institute
Patient Experience
• 12:14 arrival to UH CMC by helicopter
• VS: B/P 145/86 HR 112 Pulse ox 96% on 2L NC
• Exam: Alert and oriented x3, responding to
questions, following commands, looking to the right,
visual field cut (Homonymous Hemianopia), no
movement on left side, dense sensory loss on left,
mild dysarthria, L neglect
• NIHSS = 20
• IV tPA infusion finishing
• Foley
• Menses
3
Advancing the Vision of the Neurological Institute
Patient Experience- NIHSS
•
•
•
•
•
•
•
•
•
•
•
•
•
1a. LOC - 0
1b. LOC Questions - 0
1c. LOC Commands - 0
2. Best Gaze - 2
3. Visual Fields -2
4. Facial Palsy - 1
5. Motor Arm - 4
6. Motor Leg - 4
7. Limb Ataxia - 0
8. Sensory - 2
9. Best Language - 0
10. Dysarthria - 1
11. Neglect - 2
4
Advancing the Vision of the Neurological Institute
Patient Experience
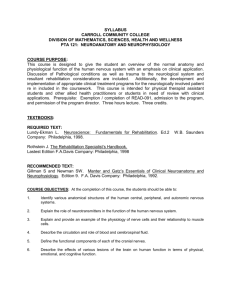
Endovascular Intervention
•
•
•
•
•
IV TPA 33% benefit
12:45 Taken for Neuro angio suite
13:05 Groin access (Door to groin = 51 mins)
R MCA Occlusion (R Middle cerebral artery)
MCA Branches
Anterior – occluded
Middle - occluded
Posterior - patent
5
Advancing the Vision of the Neurological Institute
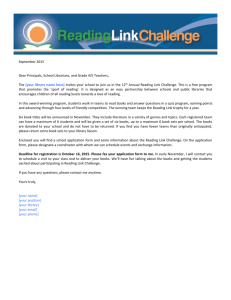
Patient Experience - MRI
6
Advancing the Vision of the Neurological Institute
Patient Experience
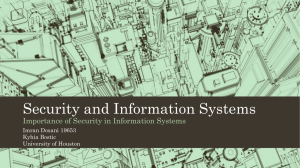
Endovascular devices
Solitaire
Penumbra
7
Advancing the Vision of the Neurological Institute
Patient Experience
Endovascular Intervention
•
•
•
•
•
•
•
•
Solitaire #1
Solitaire #2
Penumbra #1
Penumbra #2
TPA – 2 mg IA tPA
Penumbra # 3 – successful in the anterior branch
TPA – 2.5mg IA tPA
Solitaire #3 – Intermittent revascularization of middle
branch
• Post procedure NIHSS =18
8
Advancing the Vision of the Neurological Institute
Patient Experience
• Stroke Work up:
– Lipid panel: LDL = 99
– HbA1c = 5%
– Echocardiogram: EF >65%, No PFO, + atrial septal
aneurysm
– Troponin leak 0.13 but no EKG changes
• Hospital course:
– Anemia
• Hb = 5.2 due to uterine bleeding- Tx with 2U PRBC’s
– Diabetes Insipidus
9
Advancing the Vision of the Neurological Institute
Patient Experience
Diabetes Insipidus
• Kidneys are unable to conserve water as they
perform their function of filtering blood.
• Amount of water conserved is controlled by
antidiuretic hormone (ADH), also called vasopressin.
• ADH is a hormone
– Produced in the hypothalamus
– Stored and released from the pituitary gland, a small gland
at the base of the brain.
• DI caused by a lack of ADH is called central diabetes
insipidus. When DI is caused by a failure of the
kidneys to respond to ADH, the condition is called
nephrogenic diabetes insipidus
10
Advancing the Vision of the Neurological Institute
Patient Experience
Diabetes Insipidus (DI)
•
•
•
•
Hypernatremia - Na = 160’s
Urine output 200 - 300cc/ hr
TX: DDAVP, hypo osmotic fluids
Renal consult: Nephrogenic DI induced by
lithium therapy
• NSU for 6 days
11
Advancing the Vision of the Neurological Institute
Patient Experience
• Therapy (PT, OT, ST ) recommending acute
rehab
– Maximal assist to move in bed and sit up
– Able pivot
– Poor trunk control
• Modified Barium Swallow
– Passed for pureed with nectar thick liquids
– unable to take in enough calories
• PEG placed on May 3
12
Advancing the Vision of the Neurological Institute
Patient Experience
•
•
•
•
•
•
•
•
•
•
Discharged to Acute rehab on May 4, 2012
Alert Ox 2
R gaze but able to cross over to left side
L visual field cut
LUE – 0/5
LLE – 1/5
L neglect
L sensory
Dysarthria but no aphasia
NIHSS = 16
13
Advancing the Vision of the Neurological Institute
•
•
•
•
•
•
•
•
•
Patient Experience
Discharge Medications
ASA
Atorvastatin
HCTZ
Metoprolol
Ferrous Sulfate
Synthroid
Ranitidine
Heparin SQ
Ciprofloxacin for UTI
14
 0
0