Biologic Therapy in Crohn's

BIOLOGIC THERAPY
IN CROHN’S DISEASE
ATILLA ERTAN, M.D.
THERAPEUTIC GOALS IN IBD
Clinical improvement
Clinical remission
Corticosteroid weaning
Maintenance of remission
Maintained tissue healing
Decrease in hospitalization & surgical interventions
Prevention of complications
Change natural course of the disease
HISTORY OF CROHN’S DISEASE
TREATMENT
1979 Sulfasalazine, steroids
1980
1993
Antibiotics, Azathioprine, 6-MP
5-ASA
1994
1995
1998
2004
Budesonide
Mtx
Infliximab
Second generation biologics
TNF Biophysiology
Most TNF is produced by monocytes, macrophages and lymphocytes. TNF also produced by intestinal epithelial cell in response to bacterial invasion.
TNF increases secretion of chemokines, cytokines and activates adoptosis from the epithelial cells.
TNF activates adhesion molecules, such as
ICAM-I.
Key Actions Attributed to TNF
Synthesis and Actions of TNF
Mechanism for Antibody
Neutralization of TNF
van Deventer S. Gut . 1997; 40:443-48.
Scallon BJ. Cytokine . 1995; 7:251-59.
Feldman M, et al. Adv Immunol.
1997; 64:283-350.
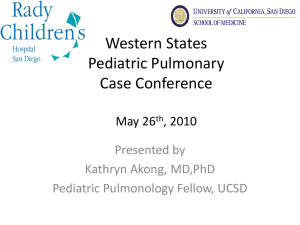
Monoclonal Antibodies, Fusion Proteins and Fab' fragments against TNF
Chimeric monoclonal antibody
Human monoclonal antibody
Human recombinant receptor/Fc fusion protein
Humanized
Fab' fragment
VL VH
Receptor
C
CH1
Fc
IgG1
Infliximab mAb
Adalimumab mAb
© UCB 2006. All rights reserved .
Constant 2
Fc
Constant 3
Etanercept
PEG PEG
Certolizumab pegol
Fab'
Adapted with permission from: Hanauer. Rev
Gastroenterol Disord 2004; 4 (supp 3): S18-24
Chimeric A2 (cA2) Monoclonal
Antibody
Infliximab
Mouse
(Binding Sites for TNF
)
Human (IgG
1
)
Chimeric (mouse/human)
IgG
1 monoclonal antibody
Binds to TNF
with high specificity, high affinity, and high avidity
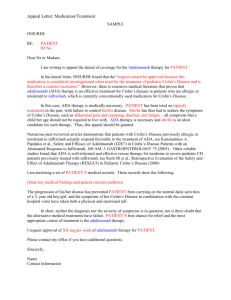
Infliximab in Patients with Crohn’s
Disease
Clinical Response defined as at least a 70-point reduction in CDAI.
Clinical Remission defined as a decline of the CDAI below 150.
Targan S, et al. New Engl J Med .
1997;337:1029-35.
Infliximab in Patients with Fistulizing Crohn’s Disease
Present D, et al. New Engl J Med . 1999; 340:1398-
405.
and 54
100
80
*p<0.001
**p=0.002
69
*
62 *
60
37
40
20
0
30
52 *
51 **
19.8
45.5
*
44.3
*
Week 8 Week 30 Week 54
Placebo 5 mg/kg Infliximab 10 mg/kg Infliximab
Rutgeerts P et al. NEJM . 2005;353(23):30-44.
Clinical Remission at Week 8, 30
ACT 1 and 54
100
80
*p<0.001
**p=0.002
† p=0.001
60
40
38.8
*
32
**
20
14.9
0
15.7
33.9
†
36.9
*
16.5
34.7
†
34.4
†
Week 8 Week 30 Week 54
Placebo 5 mg/kg Infliximab 10 mg/kg Infliximab
Rutgeerts P et al. NEJM . 2005;353(23):30-44.
Patients in Clinical Remission at
Week 2 Responders
Week 54
Clinical Remission with Steroid
Withdrawal at Week 54
Week 2 Responders Receiving Steroids at Baseline
082201.1 Lindenbaum (on screen) 15
Maintenance Therapy was
Associated with Greater
Mucosal Healing
Rutgeerts, et al. Gastroenterology 2004;126:402-413.
Number of Crohn’s-related
Hospitalizations per 100 Patients
All Randomized Patients
Rutgeerts, et al. Gastroenterology 2004;126:402-413.
Maintenance Therapy Is
Associated with Fewer CD
Surgeries
Rutgeerts, et al. Gastroenterology 2004;126:402-413.
Conclusions
The ACCENT I trial proves that when
REMICADE
®
(infliximab) is dosed every
8 weeks, patients are more likely to
Maintain clinical remission
Discontinue steroids
Maintain clinical response
Achieve mucosal healing
REMICADE maintenance is safe
Results consistent with earlier experience
Rutgeerts, et al. Gastroenterology 2004;126:402-413.
Conclusions cont.
Regular maintenance treatment with 5 or
10 mg/kg REMICADE
®
(infliximab) substantially reduces the rate and duration of hospitalization in Crohn’s disease patients, compared with single infusion plus episodic retreatment with 5 mg/kg
Rutgeerts, et al. Gastroenterology 2004;126:402-413.
Conclusions cont.
Regular maintenance treatment with 5 or
10 mg/kg REMICADE may reduce the number of all surgeries/procedures in
Crohn’s disease patients, compared with single infusion plus episodic retreatment with 5 mg/kg
Infusion Reactions
Important Safety Information:
Hypersensitivity
Infliximab should not be administered to patients with hypersensitivity to murine proteins or other components of the product. Infliximab has been associated with hypersensitivity reactions that differ in their time of onset. Acute urticaria, dyspnea, and hypotension have occurred in association with Infliximab infusions. Serious infusion reactions including anaphylaxis were infrequent. Medications for the treatment of hypersensitivity reactions should be available.
TREAT Registry
Infusion Reactions
Infliximab infusions:
Infusions with reactions:
20,309
4.6%
Infusions with serious reactions: 0.12%
Lichtenstein GR, et al. Gastroenterology. 2005;128(4):A-580.
Infections
INFECTIONS DURING INFLIXIMAB THERAPY
(n=170.000)
INFECTION
Myobacterium tbc
Pneumocystis carinii
Listeria monocytogenes
Histoplasmosis
Candidiasis
Aspergillosis
Cryptococcosis
Coccidioidomycosis n
84
12
11
9
7
6
2
2
Tuberculosis: Context
Patient Screening
Every patient being considered for an anti-TNF agent requires screening
Thorough screening may reveal potential risks:
• Past exposure
• TB treatment
• Place of birth and travel history
Why is TB reactivation still occurring?
• Many cases occur in patients who were not adequately screened and prophylaxed
• Some cases occur in patients with false-negative screening tests
TB should always be considered in all immunosuppressed patients, even if their screening PPD was negative
Monitoring for potential infections is always required when treating patients with immunosuppressive drugs
JAMA. 2004;292(14):1676-1678.
Serious Infections: Context
Other IBD Immunosuppressive
Agents
Annual rate of serious infections in infliximab-treated patients 6.4%
There is also an increased risk of serious infections with other IBD immunosuppressive agents
Many conventional therapies for Crohn’s disease have not been well studied in clinical trials
Malignancy &
Lymphoma
Lymphoma in CD Patients
CD Publication
Greenstein, 1985
Mellemkjaer, 2000
Lewis, 2001
Bernstein, 2001
Relative incidence of lymphoma
4.7- fold increase
1.5- fold increase
1.4- fold increase
2.4- fold increase
Malignancies and Lymphomas:
Other Treatments
Treatment
AZA 1
6-MP 2
6-MP 3
Cancer
(% of patients)
4.1%
6.3%*
3.1%
*Including 0.7% with lymphoma
1 Connell WR et al., Lancet. 1994;343:1249 –52. 2 Warman JI.
J Clin Gastroenterology. 2003;37(3):220 –225. 3 Present D et al.,
Annals of Internal Medicine. 1989;111:641 –9.
Clinical Trials
Malignancies in Controlled Portions
32 of Clinical Trials Compared with
General Population
Expected #
From SEER
Patientyears of F/U
Database**
General U.S.
Population
Observed
Number in
Infliximab Trials
Placebo 892 5.65
1
Infliximab 4990 29.04
29
**Excludes non-melanoma skin cancers because also excluded in SEER database
Data on file, Centocor, Inc.
Malignancy: Context
At the present time, it is not possible to be certain whether the use of anti-TNF agents increases a patient’s chance of developing a malignancy
There is also concern conventional immunomodulators may increase the risk of malignancy
Risks must always be weighed against the risks of inadequate treatment of the underlying disease
Caution should be exercised when treating any patient with a current or past history of malignancy
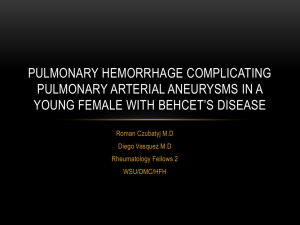
Certolizumab pegol
Molecular structure of certolizumab pegol
The chains of the Fab' fragment are shown in green and blue and the PEG is shown in yellow
Humanized PEGylated Fab' fragment of an anti-TNFα monoclonal antibody
Single Fab' fragment
engineered for production in E.coli
no need for glycosylation of Fc portion
2 x 20 kD PEG
to extend half life (ca. 2 weeks) to a value compared with a whole antibody product
compatible with sc administration
Site specific PEGylation
to hinge thiol
using proprietary linkage technology
In vitro no monocytes and lymphocytes apoptosis, no complement activation, no ADCC
© UCB 2006. All rights reserved .
Chapman A et al., Nature Biotech 1999; 17: 780-3
Fossati G and Nesbitt AM. Am J Gastroenterol 2005;100 (Suppl 9):S299
Monoclonal Antibodies, Fusion Proteins and Fab' fragments against TNF
Chimeric monoclonal antibody
Human monoclonal antibody
Human recombinant receptor/Fc fusion protein
Humanized
Fab' fragment
VL VH
Receptor
C
CH1
Fc
IgG1
Infliximab mAb
Adalimumab mAb
© UCB 2006. All rights reserved .
Constant 2
Fc
Constant 3
Etanercept
PEG PEG
Certolizumab pegol
Fab'
Adapted with permission from: Hanauer. Rev
Gastroenterol Disord 2004; 4 (supp 3): S18-24
100
80
60
40
20
0
0
Phase II: Clinical Response in Patients (ITT)
Placebo (N=73) Certolizumab pegol 400 mg (N=72) p=0.010 p=0.010
2 4 6
Weeks p=0.005
p=0.006
8 10 12
© UCB 2006. All rights reserved .
Adapted from: Schreiber et al. Gastroenterology. 2005;29(3):807-18
Phase II: Clinical Response in Patients
(Baseline CRP
10 mg/L)
100
80
60
40
20
0
0
Placebo (N=28) Certolizumab pegol 400 mg (N=32) p=0.002
p<0.001
p=0.004
p<0.001
p<0.001
p=0.005
2 4 6
Weeks
8 10 12
© UCB 2006. All rights reserved .
Adapted from: Schreiber et al. Gastroenterology. 2005;29(3):807-18
100
80
60
40
20
0
PRECiSE 2: Clinical Response at Week 26 (ITT)
3 inj. Certolizumab pegol + Placebo
Certolizumab pegol 400 mg sc p<0.001
62.8
p<0.001
61.6
36.2
33.7
All
(n=210) (n=215)
CRP
10 mg/L
(n=101) (n=112)
Schreiber, et al. Gut 2005; 54 (Suppl VII) A82
PRECiSE 2: Clinical Response at
Week 26 by Prior Anti-TNF Use
100
Certolizumab pegol 400 mg
3 inj. Certolizumab pegol
+ Placebo
80 p<0.001
68.7
60
40
39.6
P=0.018
44.2
25.5
20
0
No prior Anti-TNF
(n=159) (n=163)
Prior Anti-TNF (IFX)
(n=51) (n=52)
UCB, Inc. Data on File
© UCB 2006. All rights reserved
PRECiSE 2: Conclusions
PRECiSE 2 demonstrated that in the clinical trial certolizumab pegol induced clinical response and maintained clinical response and remission in patients with active
Crohn’s disease, regardless of baseline CRP level.
PRECISE 2: Conclusions cont.
Certolizumab d emonstrated efficacy across a broad patient population and well tolerated safety profile.
Certolizumab 400 mg q 4wk with an additional induction dose at wk 2, will be a valuable addition to the Crohn’s disease treatment armamentarium, when approved.
(Pegylated antibody fRagment
Evaluation
in C rohn’s disease Safety and
Efficacy)
PRECiSE 1 and 2 are large international, Phase III, placebocontrolled studies designed to demonstrate the safety and efficacy of certolizumab pegol in inducing and maintaining response and remission in patients with moderate to severe
Crohn’s disease
BIOLOGICS (TNF-Abs) In CROHN'S DISEASE
Name Route
Humanized antibody % Efficacy Immunogenicity
INFLIXIMAB/REMICADE IV 75 Yes High
CERTOLIZUMAB/CIMZIA SC
ADALIMUMAB/HUMIRA
ETANERCEPT
ONERCEPT
CD571
SC
100
100
Yes
Yes
No
No
No
Low
Low
Infliximab Benefit:Risk in IBD:
Summary
The natural history of inflammatory bowel disease results in a poor quality of life for many patients
Infliximab has been a major advance in treating IBD
Infliximab therapy is associated with risks, but these risks must be placed in context:
Benefits patients derive from infliximab
Risks of under-treating IBD
Risks of surgeries, other immunosuppressive
Clinical Trials
Infections in All Completed Clinical Trials
Placebo Infliximab
Patients treated
Average wks follow-up
# infections per 100 pt-yrs
# infections requiring treatment per 100 pt-yrs
1600
29.0
115.6
54.8
# serious infections per 100 pt-yrs 5.6
Pneumonia
Abscess
Cellulitis
Sepsis
Tuberculosis
0.11
0.45
0.45
0.22
0.11
5706
45.5
132.3
61.2
6.4
1.08
0.84
0.32
0.32
0.38
Data on file, Centocor, Inc.
Important Safety Information:
Risk of Infection
Tuberculosis (tb) (frequently disseminated or extrapulmonary at clinical presentation), invasive fungal infections, and other opportunistic infections, have been observed in patients receiving infliximab. Some of these infections have been fatal. Patients should be evaluated for latent tb infection with a skin test.
1 treatment of latent tb infection should be initiated prior to therapy with infliximab. Active tb has developed in patients receiving infliximab who were tuberculin skin test –negative prior to receiving infliximab. Monitor patients receiving infliximab for signs and symptoms of active tb, including those who are tuberculin skin test –negative.
1 American Thoracic Society, Centers for Disease Control and Prevention. Targeted tuberculin testing and treatment of latent tuberculosis infection.
Am J Respir Crit Care Med . 2000;161:S221 –S247.
Lymphomas Observed
During Infliximab Clinical Trials
Pt Yrs followup
Observed
Lymphomas
Expected
Lymphomas in
Non-RA
Population*
All
Studies
4996 5 1.10
47
RA
Studies
2428 2 0.62
Data on file, Centocor, Inc.
Important Safety Information:
Contraindications
Infliximab is contraindicated in patients with moderate to severe (NYHA Class III/IV) congestive heart failure
(CHF) at doses greater than 5 mg/kg. Higher mortality rates at the 10 mg/kg dose and higher rates of cardiovascular events at the 5 mg/kg dose have been observed in these patients. Infliximab should be used with caution and only after consideration of other treatment options. Patients should be monitored closely. Discontinue infliximab if new or worsening CHF symptoms appear. Infliximab should not be administered to patients with hypersensitivity to murine proteins or other components of the product.
Important Safety Information:
Hepatotoxicity
Severe hepatic reactions, including acute liver failure, jaundice, hepatitis, and cholestasis have been reported rarely in patients receiving infliximab postmarketing. Some cases were fatal or required liver transplant.
Aminotransferase elevations were not noted prior to discovery of liver injury in many cases. Patients with symptoms or signs of liver dysfunction should be evaluated for evidence of liver injury. If jaundice and/or marked liver enzyme elevations (e.g.,
5 times the upper limit of normal) develop, infliximab should be discontinued, and a thorough investigation of the abnormality should be undertaken.
Infliximab has been associated with reactivation of hepatitis
B. Chronic carriers of hepatitis B should be evaluated and monitored prior to and during treatment.
Important Safety Information:
Neurologic Events
TNF inhibitors, including infliximab, have been associated with rare cases of new or exacerbated symptoms of demyelinating disorders including multiple sclerosis, and optic neuritis, seizure, and CNS manifestations of systemic vasculitis.
Exercise caution when considering infliximab in all patients with these disorders. Consider discontinuation for significant CNS adverse reactions.
Rationale for Protocol C87042
Infliximab (IFX), a chimeric monoclonal antibody against TNF-alpha, is the only approved biological therapy for treatment of
Crohn’s disease.
IFX contains substantial murine protein sequences in the variable region. Thus, it is immunogenic and intermittent administration results in antibodies to IFX (ATIs).
Humanized monoclonal antibodies are relatively less immunogenic than chimeric
Hanauer S, et al. Gastroenterology 1999; 116: A731; Breedveld FC, Lancet 2000; 355:735-740.
antibodies.