The Thoracic Spine
advertisement

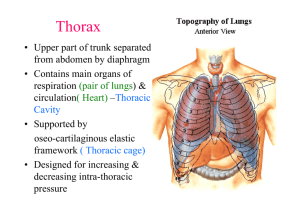
Chapter 26 The Thoracic Spine Overview In the thoracic region, protection and function of the thoracic viscera take precedence over segmental spinal mobility The thoracic complex can be a significant source of local and referred pain Anatomy The thoracic spine forms a kyphotic curve between the lordotic curves of the cervical and lumbar spines The curve begins at T 1-2 and extends down to T 12 with the T 6-7 disc space as the apex The thoracic kyphosis is a structural curve, which is present from birth Unlike the lumbar and cervical regions, which derive their curves from the corresponding differences in intervertebral disc heights, the thoracic curve is maintained by the wedge-shaped vertebral bodies, which are about 2 mm higher posteriorly than anteriorly Anatomy The thoracic vertebrae consist of the usual elements: the vertebral body (centrum), transverse processes, neural arch, and spinous process As elsewhere in the spine, the thoracic vertebrae are designed to endure and distribute the compressive forces produced by weight bearing, most of which is borne by the vertebral bodies Anatomy The thoracic vertebral body is roughly as wide as it is long so that its anterior-posterior and medial-lateral dimensions are of equal length Anatomy The height, end-plate cross-sectional area, and bone mass of the vertebral bodies increases cranial to caudal, particularly in the lower levels Progressive wedging of the thoracic vertebral bodies occurs with increasing age in the majority of individuals, with disc space narrowing at multiple levels occurring from the third decade of life Anatomy The transverse processes of the thoracic vertebrae differ from those of the cervical and lumbar spines due to the presence of a costal articular facet on the transverse process The costotransverse joint is formed by an oval facet on the lateral aspects of all of the transverse processes to which the rib attaches, except for T 11 and T 12 to which no ribs are attached Anatomy The thoracic vertebrae are classified as typical or atypical with reference to their morphology – The typical thoracic vertebrae are found at T 2-9, although T 9 may be atypical in that its inferior costal facet is frequently absent – The atypical thoracic vertebrae are the first, tenth, eleventh and twelfth Anatomy The common spinal ligaments are present at the thoracic vertebrae, and they perform much the same function as they do elsewhere in the spine The anterior longitudinal ligament in this region is narrower but thicker compared to the rest of the spine The posterior longitudinal ligament, is wider here at the intervertebral disc level, but narrower at the vertebral body than in the lumbar region Anatomy The zygapophyseal joints of the thoracic spine function to restrain the amount of flexion and anterior translation of the vertebral segment, and to facilitate rotation They appear to have little influence on the range of side bending Anatomy The bony thoracic cage is formed by twelve pairs of ribs, the sternum, the clavicle and the thoracic spine vertebrae All of the ribs are different from each other in size, width, and curvature, although they share some common characteristics Anatomy The ribs are divided into two classifications: (1) true/false and (2) typical/atypical – Ribs 1 through 7 are named true ribs because their cartilage attaches directly to the sternum – Ribs 3 through 9 are typical ribs. The typical rib is characterized by a posterior end, which is comprised of a head, neck and tubercle Anatomy The costovertebral articulation also forms an intimate relationship between the head of the rib and the lateral side of the vertebral body The radiate ligament connects the anterior aspect of the rib head to the bodies of two adjacent vertebrae and their intervening disc, in a fan-like arrangement Anatomy The costotransverse joint is a synovial joint between an articular facet on the posterior aspect of the rib tubercle and an articular facet on the anterior aspect of the transverse process, which is supported by a thin fibrous capsule Anatomy The sternum consists of three parts: the manubrium, the body, and the xiphoid process. The manubrium is broad and thick superiorly, and narrower and thinner inferiorly, where it articulates with the body Anatomy The first, sixth and seventh costal cartilages are each linked to the sternum by a synchondrosis The second to fifth ribs are each connected to the sternum through a synovial joint, whereby the cartilage of the corresponding rib articulates with a socket-like cavity in the sternum Anatomy A large number of muscles arise from and insert on the thoracic spine and ribs The muscles of this region can be divided into those that are involved in spinal or extremity motion, and those that are involved in respiration Anatomy The blood supply to this region is mainly provided by the dorsal branches of the posterior intercostal arteries, while the venous drainage occurs through the anterior and posterior venous plexuses The spinal cord region between T 4 and T 9 is poorly vascularized Anatomy In the thoracic region there is great variability in the topography of the nerves, and the structures that they serve Typically, the spinal root arises from the lateral end of the spinal nerve but, in 25% of cases, the spinal root is made up of two parts that arise from the superior border of the spinal nerve The thoracic spinal nerves are segmented into dorsal primary and ventral primary divisions Biomechanics The thoracic spinal segments possess the potential for a unique array of movements However, there is very little agreement in the literature with regards to the biomechanics of the thoracic spine and most of the understanding is based largely on the ex vivo studies and a variety of clinical models Biomechanics Flexion of the thoracic spine in weight bearing is initiated by the abdominal muscles and, in the absence of resistance, is continued by gravity, with the spinal erector muscles eccentrically controlling the descent. Flexion may also occur during bilateral scapular protraction Biomechanics Extension of the thoracic spine is produced principally by the lumbar extensors, and results in an inferior glide of the superior facet of the zygapophyseal joint 1-2º of extension is available at each thoracic segment, giving an overall average of 15-20º of thoracic extension for the entire thoracic spine Biomechanics Side bending of the thoracic spine is initiated by the ipsilateral abdominals, and erector muscles, and then continued by gravity A total of 25-45º of side bending is available in the thoracic spine, at an average of about 3-4º to each side per segment, with the lower segments averaging slightly more, at 7º to 9º each Biomechanics Axial rotation is produced either by the abdominal muscles and other trunk rotators, or by unilateral elevation of the arm Pure axial rotation (twisting) can only occur at two points in the spine: at the thoracolumbar and cervicothoracic junctions Biomechanics Because the anterior end of the ribs is lower than the posterior, when the ribs elevate they rise upwards while the rib neck drops down In the upper ribs, this results in an anterior elevation (pump handle) which increases the anterior-posterior diameter of the thoracic cavity In the middle and lower ribs (excluding the free ribs), this results in a lateral elevation (bucket handle), which increases the transverse diameter of the thoracic cavity Examination Differential diagnosis of thoracic pain can be difficult. This is due to the complicated biomechanics and function of the region, the proximity to vital organs, and the many articulations Examination Pain arising from inflammation of the axial spine can mimic a variety of serious conditions, including cardiac/pulmonary pathology, renal colic, fracture, a tumor, or numerous visceral and retroperitoneal abnormalities, including abdominal aortic aneurysm Examination History – The clinician must determine if the pain is provoked or alleviated with movement or posture (musculoskeletal pain), respiration (rib dysfunction or pleuritic pain), eating or drinking (gastric pain), or exertion (rib dysfunction or cardiac pain) Examination Systems Review – Thoracic pain may originate from just about all of the viscera – Both visceral and somatic afferent nerves transmit pain messages from a peripheral stimulus and converge on the same projection neurons in the dorsal horn – The thoracolumbar outflow of the autonomic nervous system has its location here. Stimulation of this outflow can lead to the presence of facilitated segments, and trophic changes in the skin of the periphery Examination Observation – The clinician should observe: The relationship of the bony structures Smoothness of the thoracic curve The degree of thoracic kyphosis The amount of lateral curvature of the thoracic spine Chest wall shape Asymmetry in muscle bulk, prominence, or length Examination Palpation – The areas of spinous process obliquity may be divided into four regions by the so-called ‘rule of three’ 1st group of 3 spinous processes (T 1-3) are level with vertebral body of the same level 2nd group of 3 spinous processes (T 4-6) are level with the disk of the inferior level 3rd group of 3 spinous processes (T 7-9) are level with the vertebral body of the level below The 4th group of 3 spinous processes reverse the obliquity Examination Active Motion Testing – Active range of motion tests are used to determine the osteokinematic function of two adjacent thoracic vertebrae during active motions, to determine which joints are dysfunctional, and the specific direction of motion loss – Active range of motion is initially performed globally, looking for abnormalities, such as asymmetrical limitations of motion – A specific examination is then performed on any region that appeared to have either excessive or reduced motion Examination For those clinicians heavily influenced by the muscle energy techniques of the osteopaths, position testing is used to determine which segment to focus on Other clinicians omit the position tests and proceed to the combined motion and passive physiological tests Examination Costal examination – It is well worth postponing the costal, or rib, examination until after the thoracic spinal joints have been examined and treated, or the testing of which proved negative Examination A neurological deficit is very difficult to detect in the thoracic spine In this region, one dermatome may be absent with no loss of sensation Sensation should be tested over the abdomen; the area just below the xiphoid process is innervated by T 8, the umbilicus by T 10, and the lower abdominal region, level with the anterior superior iliac spines, by T 12 Too much overlap exists above T 8 to make sensation testing reliable Intervention Acute phase goals include: – – – – – – – – Decrease pain, inflammation, and muscle spasm Promote healing of tissues Increase pain-free range of vertebral and costal motion Regain soft tissue extensibility Regain neuromuscular control Initiate postural education Promote correct breathing Educate the patient about activities to avoid and positions of comfort. – Allow progression to the functional stage Intervention Functional phase goals – To significantly reduce or to completely resolve the patient’s pain – The restoration of full and pain-free vertebral and costal range of motion – Full integration the entire upper and lower kinetic chains – Complete restoration of respiratory function – The restoration of thoracic and upper quadrant strength and neuromuscular control