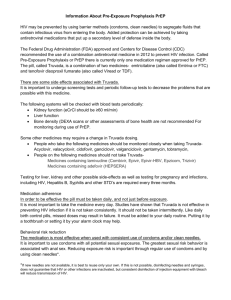
Global epidemiology
Over 7000 new infections a day in 2012
Western
Europe
900,000
North america
1,400,000
Eastern Europe
& Central Asia
1,400,000
InNorth
2012Africa &
Middle: East
New HIV infections
2.5 million
300,000
Deaths due to AIDS
: 1.7 million
East Asia
830,000
South-East Asia
4,000,000
Latin america
1,400,000
Sub-saharan
Africa
23,500,000
Oceania
53,000
Adults and children living with HIV
UNAIDS report on the global AIDS epidemic 2012
6
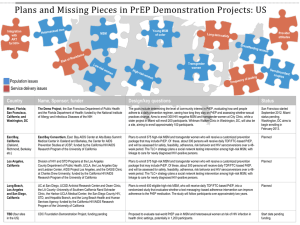
USA
Estimates of New HIV Infections in the United
States, 2011, for the Most-Affected Subpopulations
12,000
Fast Facts
11,200
1,148,200 persons living with
HIV infection , including 207,600
persons undiagnosed (18.1%)
10,600
Number of New HIV Infections
10,000
8,000
≈ 50,000 people newly
infected/year
+++ 20-24 years
6,700
6,000
5,300
4,000
2,700
2,000
0
1,300 1,200 1,100
White
MSM
Black
MSM
Hispanic/
Latino
MSM
Black
Hetero
sexual
Women
Black
Hetero
sexual
Men
White
Hispanic/ Black
Male
Hetero
Latino
sexual Heterosexual IDUs
Women
Women
850
Classification by transmission:
Male-to-male sexual contact :
28,782
Heterosexual contact : 12,875
Black
Female
IDUs
Centers for Disease Control and Prevention
EUROPE
HIV infections, per 100,000 population, reported for 2011 : All cases
≈54,000 HIV diagnoses
of which 28,000 in EU
and EEA
Rapport UNAIDS 2012
8
EUROPE
HIV infections, per 100,000 population, reported for 2011 : Heterosexual cases
Rapport UNAIDS 2012
9
EUROPE
HIV infections, per 100,000 population, reported for 2011 : MSM cases
Rapport UNAIDS 2012
10
EUROPE
• Trends of reported HIV diagnoses, by transmission mode and
year of diagnosis, adjusted for reporting delay, EU/EEA,
2004–2011
Heterosexual, excluding cases
originating from sub-Saharan Africa
Heterosexual cases originating from
sub-Saharan Africa
Men who have sex with men
Injecting drug users
Mother-to-child transmission
Other/undetermined
HIV/AIDS Surveillance in Europe 2011 by WhHO ECDC
11
FRANCE
HIV Seropositivity Discovery
6100 people newly infected in 2011
8000
7500
7670
7451
7555
7098
7000
6464
6500
6318
6297
6262
6088
6000
5500
5000
2003
2004
2005
2006 2007 2008
Year of Diagnosis
2009
2010
2011
InVS données DO VIH au 31/12/2011
12
FRANCE
Epidemiology of new infection by
transmission mode
Fast facts
2400 gay and
bisexual men
40% of all
new infections
Year of diagnosis
InVS données DO VIH au 31/12/2011
13
HIV prevention opportunities
Sexual
monogamy
Behavioral Interventions
Aim to lower of partner change, alter
risk taking behavior
Correct &
consitent
condom use
Education
Delayed
sexual
debut
PrEP
Sexual
abstinence
Treatment
of STIs
HIV Prevention toolbox
Treatment of
the infected
population
Biological Interventions
Aim: to reduce the efficiency of
transmission or to shorten the
duration of infectiousness
Male
circumcision
15
What is PrEP ?
• Pre-exposure prophylaxis (PrEP) is based on
the use of antiretroviral therapy in HIV
negative people at risk HIV to block
transmission of the virus.
• This treatment could be taken systemically
(tablets) or topically (vaginal or rectal gels),
continuously, daily, or intermittent, framing
the risk of exposure.
16
New method ?
1994:
Prevention
of mother to
child
transmission
1997: PEP:
PostExposure
Prophylaxis
TASP:
Treatment
as
Prevention
Test and
treat
2012:
Truvada®
PrEP
17
Truvada®
• Molecules:
Emtricitabine 200mg (FTC) + tenofovir disoproxil fumarate 300mg (TDF)
Fixed–dose combination tablet of two nucleos(t)ide reverse transcriptase
inhibitors (NRTIs)
18
Truvada® : Mechanism of action
19
Truvada®
• Side effects
– Serious :
• Severe liver problems : hepatomegaly , steatosis Build-up of lactic
acidosis
• Kidney damage hypophosphataemia => Bone mineral density loss
• Worsening of pre-existent hepatitis B infection
– Common :
• Headache
• Dizziness
• Vomiting, nausea, diarrhea
• Raised blood levels of creatine kinase
20
HIV : where do we stand ?
Truvada® : with other
antiviral medicines, to
treat HIV1 in adults
NB: L’initiation d’abacavir ne peut être envisagée que chez
des patients ne présentant pas l’allèle HLA-B57*01.
http://www.sante.gouv.fr/IMG/pdf/05_Traitement_anti_retroviral.pdf
21
W
TDF&FTC: potent
inhibitors of HIV
Increases the number
of mutations required
for resistance
Penetrates well in
sites of HIV exposure
Why Truvada® ?
Greater activity than
TDF alone
No drug interaction
with ttm against
malaria, tuberculosis,
or oral
contraceptives
Long half-life 1
tablet a day
Good safety and
tolerability profile for
treatment
22
Regulatory history
Viread®
(TDF)
2001
2001
Emtriva®
(FTC)
2002
2003
Complera®
(FTC/TDF/RPV)
2011
Truvada®
(FTC/TDF)
2004
Atripla®
(FTC/TDF/EFV)
2008
2004
TDF : tenofovir disoproxil fumarate
FTC : emtricitabine
EFV : efavirenz
RPV : ripavirine
2006
2011
2012
2012
Truvada® PrEP
(FTC/TDF)
24
FDA approval
• July 2012
• Truvada® for pre-exposure prophylaxis indication :
With safer sex practices at all times to reduce the risk of getting HIV1 :
– in MSM who are at higher risk of getting infected with HIV1 through sex,
– in heterosexual couples where one partner has HIV1 and the other has not.
• Supplemental New Drug Application (sNDA)
• Priority Review: 6 months instead of 10
25
Clinical trials of oral PrEP
Trial
Location
Population
Intervention
Phase III/ IIb
iPrEx
Brazil, Ecuador, Peru,
South Africa, Thailand,
USA
Adult MSM at high risk
Daily oral FTC/TDF
Partners PrEP
Kenya, Uganda
Serodiscordant couples
Daily oral TDF or
FTC/TDF
CDC TDF2
Botswana
Adult heterosexual
men and women
Daily oral FTC/TDF
Fem-PrEP
Kenya, South Africa,
Tanzania
Adult women at high
risk
Daily oral FTC/TDF
VOICE
Uganda, South Africa,
Zimbabwe
Adult women
Daily oral FTC/TDF or
TDF or tenofovir
vaginal gel
Phase II
CDC 4323
USA
Adult MSM
Daily oral TDF
(immediate vs oral
treatment)
FHI PrEP
Ghana, Cameroon,
Nigeria
Adult women at high
risk
Daily oral TDF
28
Trial Designs
Trial
Population
Randomized (N)
Intervention
iPrEx
Adult MSM at high
risk
2499
Daily oral FTC/TDF
vs Placebo
Partners PrEP
Heterosexual
serodiscordant
couples
4747
Daily oral TDF
or FTC/TDF
vs Placebo
• Randomized, prospective, placebo-controlled
• Monthly HIV-testing
• Powered to show at least 30% efficacy (standard threshold in HIV
vaccine and microbicide trials)
• Risk-reduction counseling, contraception counseling and referral
for circumcision (for Partners PrEP), condoms, treatment of
symptomatic STIs and HIV-1 testing provided at every visit
29
Trial Designs
Primary outcome: Anti-HIV seroconversion and safety endpoints
30
Inclusion criteria
• iPrEx :
– Male (18 years and older)
– HIV uninfected
– High risk for HIV infection: any of the followings in the past 6 months:
• no condom use during anal intercourse with male partner who is HIV+ or HIV status is
unknown
• anal intercourse with more than 3 male sex partners
• prostitution
• STI at screening or in the 6 months prior to study entry
• inconsistent condom use with HIV+ partner
• Partners PrEP :
– Male and female
– HIV-1 seropositive partner not yet eligible for ART treatment
31
iPrEx
64 infections
44%
fewer
• 44% efficacy overall (CI 95%: 15-63%)
• P-value: 0,005
• 92% efficacy when the drug was
detected in blood
• Drug detection correlated with
seronegative status
36 infections
Placebo
Truvada
33
IPrEx
Cumulative HIV Incidence by Treatment Time
34
iPrEx
• Adherence by intracellular TFV-DP levels: efficacy
Non-Measurable
Measurable
100%
87.5%
4.2%
4%
3.6%
3%
2%
1%
0.5%
0%
Placebo
Non-Measurable
Measurable
Relative risk reduction
HIV conversion per PY (%)
5%
80%
60%
40%
20%
14.5%
0%
Non-Measurable
Measurable
35
Primary efficacy
outcome
mITT analysis
Tenofovir
Tenofovir/emtricita
bine
Placebo
HIV acquisitions, n
17
13
52
HIV incidence/100
patient-years
0,65
0,50
1,99
Efficacy vs placebo
(%)
(95% CI)
67
75
(44-81)
(55-87)
P value
<0,001
<0,001
mITT: modified intention to treat
• If drug detected in the blood: TDF=86%; Truvada® : 90%
• On july 2011, Data and Safety Monitoring Board recommanded
discontinuation of placebo arm
36
Primary efficacy results
37
Efficacy
(95% CI)
P-value
Interaction
P-value
TDF
Women
71%
(N=595)
(37-87%)
p=0,002
p=0,65
Men
63%
(N=984)
(20-83%)
p=0,01
FTC/TDF
Women
66%
(N=566)
(28-84%)
p=0,005
p=0,24
Men
84%
(N=1010)
(54-94%)
p<0,001
38
• Adherence by plasma TFV levels: efficacy
2.5
Hiv conversion per PY (%)
2
52/2607
2%
5/235
2,1%
1.5
Placebo
6/733
1
Never measurable
0,8%
0.5
Sometimes measurable
2/1648
Always measurable
0,1%
0
Placebo
Never
measurable
Sometimes
measurable
Always
measurable
39
IPrEx
– Side effects:
• Nausea and abdominal pain in <10%, mainly in the first 4
weeks
• Loss of weight, mainly in the first 12 weeks
• Average 1% Bone Mineral Density loss
• Mild-moderate serum creatinine elevation (2,4%
Truvada® vs 2,2% placebo)
41
IPrEx
Safety : Severe and Serious Adverse Events (AE)
42
IPrEx
Safety : Clinical Adverse Events Grade 2 and Above
43
– Side Effects:
No significant differences with placebo
Number (%) of
participants
TDF
Death
8
SAE
(<1%)
118
(7%)
P-value vs
placebo
0,80
1,00
FTC/TDF
8
(<1%)
115
(7%)
P-value vs
placebo
0,80
0,89
Placebo
9
(<1%)
118
(7%)
45
– Side Effects:
Birth outcomes were similar
TOTAL
TDF
FTC/TDF
Placebo
Number of pregnancies
288
112
80
96
Number of pregnancies
With outcomes available
262
103
74
85
167
73
40
54
(64%)
(71%)
(54%)
(64%)
95
30
34
31
(36%)
(29%)
(46%)
(36%)
0,35
0,26
Data through 30 January 2012
Pregnancy outcome
Live birth
Pregnancy loss
P-value, vs placebo
46
Safety Summary
Overall Safety
Renal safety
Bone safety
iPrEx
Partners PrEP
Similar to placebo with
more gastro-intestinal
events through week 4
Similar safey profile to
placebo
Mild-moderate serum
ceratinine elevation: 2,4%
FTC/TDF vs 2,2% placebo
No increase in fracture,
small decrease in BMD at
the spine and hip, which
returned toward baseline
Infrequent serum
creatinine abnormalities
(<2%), similar across all
arms
No increase in fracture,
Evaluation of BMD not
performed
47
Resistance
NRTI resistance/ infections
Trial
iPrEx
Drug
On treatment
Baseline
FTC/TDF
0/48
2/2
FTC/TDF
0/12
1/3
TDF
0/15
2/5
Partners PrEP
49
Risk Compensation
51
Other clinical trials:
Population
Design
FEMPrEP
African
women
Oral
Truvada
daily vs
placebo
TDF2
African
heterosexual
men and
women
Oral
Truvada
daily vs
placebo
African
women
Tenofovir
gel 1% vs
placebo
CAPRISA
004
VOICE
African
women
Oral:
Truvada vs
TDF vs
placebo
Vaginal gel:
TDF vs
placebo
Efficacy
Sexual
behavior
Compliance
Resistance
No (stopped
futility)
<26% (plasma level)
On 68 infections, 1
resistant with
placebo, 4 with
Truvada
62% (strongly
related to
adherence)
>80% in both
groups (pill counts,
results in blood not
available)
1 person infected at
enrollment
developped
resistance
Number of
partners
declined in
both arms
no
slight
increase of
condom use
in both arms
39%
Tenofovir gel
and pills arms
stopped due to
inefficacy.
Truvada arm
continues.
60% (count of gel
bottles)
53
Conditions of approval
– collect viral isolates :
• from individuals infected by HIV during PrEP
– collect data on pregnancy outcomes :
• for women who become pregnant during PrEP
– conduct a trial for evaluation of drug adherence :
• relationship to adverse events
• risk of seroconversion
• Development of resistance in seroconverters.
– REMS
56
REMS
Risk Evaluation & Mitigation Strategy
= Risk Management Plan
• Advised by FDA Antiviral Products Advisory Committee
• Initial REMS approval : 07/16/2012
• Annual assessment
• Central component :
– Training and educational program
58
REMS
Risks
Description
HIV-1 Acquisition
Truvada PrEP may not always prevent HIV-1 acquisition,
even when there is adherence to the dosing regimen and
other prevention strategies are used.
Poor adherence to Truvada and other prevention
strategies further increases the risk of HIV-1 acquisition.
Development of
Resistance
Resistant HIV-1 variants may emerge in subjects with
unrecognized HIV-1 infection who continue to take
Truvada to reduce the risk of acquiring HIV-1.
Post-treatment
exacerbations of HBV
Acute exacerbations of HBV may occur upon
discontinuation of Truvada in individuals treated with
Truvada for HIV-1 pre-exposure prophylaxis who are
infected with HBV.
Identified risks
Potential risk
59
REMS
• Goals :
– Inform and educate :
• Prescribers, other healthcare professionals and individuals
(taking or considering Truvada for PrEP)
– About :
• Importance of strict adherence
• Importance of regular monitoring of HIV-1 status
To reduce the risk of development of resistant HIV-1
variants
• Truvada for PrEP which is only part of a comprehensive
prevention strategy with other preventive measures
60
REMS
• REMS Elements :
– Timetable for submission of assessment
– Medication guide
– Elements to assure safe use :
• Training & education program :
– Safety inforamtion fact sheet
– Important information for prescribers
• Materials for healthcare providers
– Dear Healthcare Providers Letter
– Important Safety information :
All these documents and information are :
» For healthcare providers
» For uninfected individuals
appended and part of the
REMS
– Agreement form
– Checklist for prescribers
– Other supports for training and education :
» Full prescribing information
» Prescriber Educational Slide Deck
» Training Guide for Healthcare Providers
• Website
• Additional actions to ensure safe use
61
Medication guide :
• Dispensed with each Truvada® prescription
• In paper hard copy
• Give the most important informations for the patient :
– Serious side effects & side effects
– Negative status to begin and test every 3 months
– Reminders (safer practises, does not always prevent HIV, does not cure HIV
infection or AIDS)
– indication
– Contraindications (positive or unknown status, drugs)
– Informations about :
• Risks
• Pregnancy (registry)
• The drug (taking, storage, ingredients)
62
Elements to assure safe use :
• Training & Education Program :
–
–
–
–
Safety information fact sheet
Important informations for prescribers
Online
Avaible as hard copy upon request
– Targets :
•
•
•
•
Primary Care physicians
Infectious diseases specialists
Obstetrician-gynecologists
Addiction specialists
63
Safety Information Fact Sheet :
• Dissemination bi-annually for 3 years
• Sent to :
– 12 associations of prescribers
e.g. : HIV Medicine Association, Infectious Diseases Society
of America
– Medwatch
64
Safety Information Fact Sheet :
•
Indication
•
Boxed Warning
o
o
•
3 key safety informations
o
o
o
•
Negative status
No sign/symptom of infection
Drug resistant HIV-1 risk
Comprehensive prevention strategy
Recommended dosing regimen
For more information
65
Important Informations for Prescribers :
• Target healthcare providers through select
professional scientific journals
• Published quaterly for 3 years
• In 5 professional society journals :
–
–
–
–
–
Journal of the American Medical Association
Journal of the Academy of Family Physicians
Obstetricians and Gynecologists
Clinical Infectious Diseases
New England Journal of Medicine
66
Important Informations for Prescribers :
Indication
Boxed Warning
Negative status
No sign/symptom of infection
3 key safety informations
Drug resistant HIV-1 risk
Comprehensive prevention strategy
Recommended dosing regimen
For more information
67
Elements to assure safe use :
• Materials for Healthcare Providers :
– Agreement form
– Checklist for Prescribers
68
Agreement Form :
• 3 parts :
o Indication and factors to
identify high risks
o Prescriber Agreement
and the list he has to do
o Uninfected Individual
Agreement and the list of
understandings and
explanations
69
Checklist for Prescribers :
•
Checklist :
• Have to be done
• At each visit
• 17 points :
o High risk evaluation
o Negative status
o Discussion about :
o Risks, Screenings,
adherence, prevention,
STIs
o HBV
o Creatinine Clearance
o Antiviral drugs
o Access to information
o Side effects
o Medication Guide
o Pregnancy
70
Elements to assure safe use :
• Website :
– www.TRUVADApreprems.com
– Access to :
• Specific information about Truvada® PrEP
• Educational and training materials
– Remain for 3 years
71
Elements to assure safe use :
• Additional actions to ensure safe use :
– Additional languages :
• To the Boxed Warnings :
–
–
–
–
“Negative HIV test must be confirmed”
“HIV test every 3 months”
“Drug resistant HIV-1 variant”
“Lactic acidosis, hepatomegaly, HBV”
• To the Warnings & Precautions :
– “How Truvada® should be used”
– “Strict adherence to the dosing regimen”
– New contraindication for use as PrEP
– start.truvada.com
72
Targeted populations : MSM in the US
• MSM = 2% of the US
population = 6.3 million
12,000
10,000
8,000
• But 61% of the new HIV
infections in 2011
28,500 new cases in
MSM every year in the US
6,000
4,000
2,000
0
• 30% of MSM are considered
at « very-high risk »
≈ 2 million
Centers for Disease Control and Prevention
74
Costs in the USA
• Medicine cost
$11,000/year
• Initial consult: HIV-testing, physical
exam, HBV testing, creatinine
clairance…
• Quarterly HIV-testing,
medical
$12,000/year
consult
$1,300/1st year,
$1,020 after
• Adherence promotion
• Condoms
Provided by Gilead for
PrEP users
Free coupons from
Gilead
75
Number needed to treat
• Mathematical model (Desai et al. Study)
– Takes into account infections prevented in people NOT
taking PrEP
– Hypothesis: 50% efficacy and 50% adherence
– For very-high risk MSM (5year treatment):
9 taking PrEP
1
infection averted
Desai, AIDS 2008, 22:1829-1839
76
Number needed to treat
• The iPrEx Trial = Without taking into account infections
prevented in people NOT taking PrEP, during 2.5 years
– 44% efficacy overall = closer to “real life conditions”:
Number Needed to Treat : 36 persons to avoid 1 infection
– 92% efficacy when the drug was detected in blood:
Number Needed to Treat : 19 persons to avoid 1 infection
77
Costs per infection averted
• From:
– NNT = 9 $540,000
• To:
Closer to
« real-life »
– NNT = 36 $1,080,000
– NNT = 19 $570,000
• Compared to:
– Lifetime HIV-treatment : $379,668
78
QALY gained
• Life expectancy
– HIV+ : 32.1 years post diagnostic
Loss of 11.5 years of life
– HIV- : 43.6 years post testing
• QALY values :
– HIV : 0.87, lasting 28 years
– AIDS : 0.62, lasting 4 years
mean QALY value : 0.84
• QALY gained by HIV- :
– HIV+ life expectancy : 26.7 QALY
16.9 QALY gained if HIV79
Cost-effectiveness
• According to our data:
– ICER = ($1,080,000 - $379,668) / 16.9
= 41,400 $/QALY
Cost-effective
According to US standards ($50,000 to
$100,000)
• BUT : Based on the iPrEx study
Only high-risk MSM
80
Dynamic model : Cost-effectiveness of PrEP
in men in the USA
250
ICER, $/QALY
200
216.48
172.091
188.421
150
All MSM
Cost-effective
H-R MSM
100
50
40.279
44.556
52.443
20%
50%
% of MSM taking PrEP
100%
0
Ann Intern Med. 2012 Apr 17;156(8):541-50. Juusola JL, Brandeau ML, Owens DK, Bendavid E. The CostEffectiveness of Preexposure Prophylaxis for HIV Prevention in the United States
81
Reimbursment
• Private insurance and Medicare positions :
– Reimburse by main private insurances
– Can be part of Medicare part D and Medicaid
• Truvada® Medication Assistance Program :
– For PrEP
– For low income people
– For people without Medicaid or any other public
or private coverage for prescription drugs.
82
Truvada® US sales by trimester
FDA approval
500
Sales in millions
400
$373,6
$373,3
Q4 2011
Q1 2012
$393
$414,5
$431,7
300
200
100
0
Q2 2012
Q3 2012
Q4 2012
83
Gilead Global pricing policy : 4 levels
« Developed » countries : High prices
USA :
$11,000
France :
$8,500
Japan:
$17,000
Australia :
$13,500
84
Gilead Global pricing policy : 4 levels
Upper middle income: -70% compared to 1st level
$3,000/yr
Part of Gilead Access Program
85
Gilead Global pricing policy : 4 levels
Lower-Middle Income
$550/yr
Part of Gilead Access Program
86
Gilead Global pricing policy : 4 levels
Low Income : No-profit price
$300/yr
Part of Gilead Access Program
87
Gilead Access Program
Growth of the Gilead Access Program
• More than 130 countries
• 3.1 million patients
• Licensing partnerships with
14 Indian companies and
one South African
company
Generic products
• Branded Truvada® : $45
(LMI) to $26.25/mth (LI)
Generic Truvada® : $7/mth
88
EUROPE
CNS: Report in response to
the referral of Mr Director
General of Health
February , 2012
EMA :Reflection paper on
the non-clinical and clinical
development for oral and
topical HIV pre-exposure
prophylaxis (PrEP)
EMA Submission?
March 2012
91
Raised issues
•
•
•
•
•
Resistance
Reimbursement by French health authority
Long term toxicity in healthy people
Increase of high-risk sexual behaviour
Change in prevention strategy
92
French experts
Favourable impact of PrEP only if :
• Population at high risk of infection (incidence rate > 1%)
• Efficacy > 50% ( adherence)
• No increase of high-risk sexual behaviour
Decrease of 5 to 25 % of incidence in these populations
In France, only possible for MSM
93
French Market access
CNS* recommendation :
• Include PrEP in a global approach linking prevention, treatment
and HIV screening/testing.
• Ensure permanent and adequate access to therapeutic
education and information.
• Monitor the impact of PrEP on risk taking and ensure an
effective pharmacovigilance system.
• Use a different brand name for PrEP and a packaging with
condoms.
Conseil National du Sida
94
European Trial
• Need of European data for EU approval
• Beginning: February 2012
• France and Canada, 1900 MSM (anal sex, without systematic
use of condoms, at least 2 sexual partners in the last 6
months)
• Oral Truvada® vs placebo, occasional intake (2 tablets a day
before sexual intercourse, then once a day until 24h after the
last intercourse)
95
Ipergay
• Interests of an intermittent PrEP (on-demand):
• Acceptability, compliance, closer to the MSM
sexual activity
• Long-term safety, reduce side effects
• Less expensive
96
Clinical Trials : Recruitment
• Proving efficacy : need to recruit people who recognize taking
risk and not using condoms.
Contrary to the aim of prevention
• Informed consent : Providing full information about the risk and
prevention methods to patients (iPrex, Ipergay)
Cases of non-compliance of recruitment conditions
in Thailand (coercive recruitment), Cameroun,
France (TROD)…
99
Placebo arm
• Is the placebo arm (Ipergay study) still ethical after the FDA
approval ?
☞ maintain placebo arm
☞ change Ipergay design : replace placebo arm by continuous
Truvada®
☞ stop Ipergay & evaluate PrEP on available data : RTU ?
100
Placebo arm
☞ maintain placebo arm
Double-blind placebo-controlled randomized study :
• Decreases the unsafe sex : use protection measures.
• Effective assessment of PrEP efficacy (combined with condoms)
☞ change Ipergay design
• Intermittent PrEP vs continuous PrEP not feasible (> 10,000 patients)
AIDES and WARNING request the provision of a RTU as a « condition »
101
Placebo arm
☞ stop Ipergay & evaluate PrEP on available data : RTU ?
AIDES arguments:
• The benefit / risk ratio is favourable in a preventive indication.
• The indication extension was recently granted by the FDA.
• The risk of the development of an alternative Truvada market:
Deprive patients of appropriate supervision.
102
Side Effects
• Potential long-term side effects :
• Truvada® for Healthy people and Prevention use: renal
function, loss of bone mineral density…
• For a mild effectiveness when poor adherence.
104
Behavior and Effectiveness
• Unsafe Sex :
• Substantial increase in unsafe sex offset the benefits of
PrEP on a population level in real life.
≠
• The optimal conditions in the clinical study lead to decrease
the unsafe sex.
• Ensure an effective and clear communication /access to
information.
105
Market access
• Cost–effectiveness :
• $12,000 per year
• Is high-priced interventions cost-effective?
• Exacerbation of healthcare inequalities :
• Ensure Truvada® for PrEP when a lot of people still don’t have access to
HIV treatment ?
• If PrEP not reimbursed: taken only by people who can afford to pay.
• If PrEP reimbursed: Justified for an intentional risk taking?
• Displacement of funds : conventional prevention
PrEP.
106
Drug resistance
• Truvada® will be used for both treatment and PrEP
• In case of seroconversion under PrEP: need to stop immediately.
If not : possible drug resistance.
• Could infect someone with a strain of HIV resistant-virus.
potential public health benefits of PrEP
VS potential public health risk of drug resistance
107
Conclusion
108
Discussion: What do you think?
Any questions?
Thanks
• Dr Yves Poinsignon, CHBA
• Pr André Tartar, Université Lille 2
111