Urinary System Study Guide: Anatomy & Physiology
advertisement

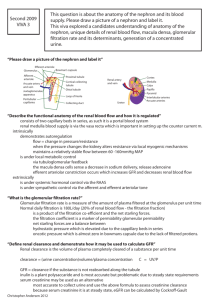
CHAPTER 20: URINARY SYSTEM OBJECTIVES: 1. Name the major function of the urinary system, and name and locate (on a diagram) the organs that compose the system. 2. Explain what the term renal refers to. 3. Define the term retroperitoneal. 4. Using a cross-section diagram of a kidney, locate the renal capsule, renal cortex, renal medulla, renal pyramids, minor calyces, major calyces, renal sinus, renal pelvis, and ureter. 5. Discuss the many ways in which the kidney maintains the blood. 6. Name the functional unit of the kidney. 7. Distinguish between a renal corpuscle and renal tubule, and identify each component on a microscopic section of the kidney. 8. Trace a drop of blood from the heart through a nephron and back to the heart. 9. Explain FULLY the structure and the significance of the juxtaglomerular apparatus. 10. List the three major steps involved in urine formation, name the portion of the nephron where each occurs, and discuss each process fully. 11. Explain why proteins are not filtered out of the blood in the glomerulus. 12. Name the force responsible for glomerular filtration. 13. FULLY discuss the negative feedback mechanisms involved in the regulation of the glomerular filtration rate (GFR). 14. Explain the process by which most reabsorption occurs in the PCT, and list the substances that are reabsorbed here. 15. Explain the significance of anti-diuretic hormone (ADH) and what it targets. 16. List the wastes excreted in urine, and explain the origin of the by-products. 17. Explain the structure, location, and function of the ureters and urinary bladder. 18. Define the term micturition. 19. Discuss the differences between male and female urethras. 20. Trace a drop of urine from its initial collection point as the "glomerular filtrate". I. INTRODUCTION The major function of the urinary system to remove metabolic wastes from blood, and direct them out of the body. The organs of the urinary system include the kidneys, ureters, urinary bladder, and urethra. See Fig. 20.1 and Fig 20.2, page 773. II. URINARY ORGANS A. Kidney (Renal) 1. Location: Fig 20.1, page 773 and Fig 20.3, page 774. a. b. c. 2. Structure: a. b. c. d. e. f. g. h. 3. high on posterior abdominal wall; retroperitoneal; right kidney lies just below left. Why? Fig 20.4a, page 775. renal capsule renal cortex renal medulla renal pyramids ureter renal pelvis = = = = = = tough fibrous shell around kidney; outer portion of kidney; inner portion of kidney; cone shaped masses of tissue in renal medulla; tube leading from kidney; superior end of ureter which is expanded to form a funnel shape; major calyces = divisions of renal pelvis (2-3 tubes); minor calyces = divisions of major calyces. Functions of Kidney: a. to remove metabolic wastes from blood & excrete them to outside (urine). b. Maintenance of blood: o regulation of RBC formation (hormone erythropoietin); o blood pressure (enzyme renin); o blood volume (hormone ADH); o blood composition; o blood pH. II. URINARY ORGANS A. Kidney (Renal) 4. Blood flow: Macroscopic = Fig 20.5, page 775 and Fig 20.6, page 777; Microscopic = Fig 20.10, page 779, and Fig 20.14, page 783; Summary Fig 20.15, page 783 Aorta Renal Artery (to each kidney) Interlobar arteries (between each pyramid) Arcuate arteries (between medulla & cortex) Interlobular arteries (within cortex) Afferent arteriole (leading to glomerulus) Glomerular capillaries (site of filtration) Efferent arteriole (leading away from glom) Peritubular capillaries/vasa recta (around renal tubule) Interlobular veins Arcuate veins Interlobar veins II. Renal vein IVC. URINARY ORGANS A. Kidney (Renal) 5. The functional unit of a kidney = the nephron. Fig 20.4c, page 775. a. o o Structure: A nephron is composed of a renal corpuscle and a renal tubule. Renal Corpuscle = glomerulus (filtration unit) within Bowman's capsule. Renal Tubule = 1. proximal convoluted tubule; 2. descending loop of Henle; 3. ascending loop of Henle; 4. distal convoluted tubule; 5. collecting duct. Each collecting duct empties into a minor calyx, which leads to a major calyx and into the renal pelvis. Refer to Fig 20.7 page 778 to see a scanning electron micrograph of glomeruli within the renal tubules, and Fig 20.11, page 780, illustrating light micrographs of the kidney, which you will observe in lab. 6. Juxtaglomerular Apparatus (JGA) = point of contact between the afferent arteriole and distal convoluted tubule (DCT). See Fig. 20.12, page 781. a. b. c. 7. Macula Densa = cells in DCT in contact with afferent arteriole. Juxtaglomerular cells = smooth muscle cells in afferent arteriole. The JGA is very important in the regulation of glomerular filtration (see below)! Cortical and Juxtamedullary Nephrons a. 80% of nephrons are found mostly in the cortex and are therefore termed Cortical Nephrons b. 20% of nephrons have a Loop of Henle the extends deep into the renal medulla and are therefore termed Juxtamedullary Nephrons o Very important in the production of dilute urine at times of dehydration as will be discussed later. o See Figure 20.13 page 782. II. URINARY ORGANS A. Kidney (Renal) 8. Urine Formation: The nephrons function to remove wastes from blood and regulate water & electrolyte concentrations. Urine is the end-product of these functions. Urine formation involves three major steps including glomerular filtration, tubular reabsorption, and tubular secretion. Urine excreted = Glomerular Filtration + Tubular Secretion – Tubular Reabsorption a. Glomerular Filtration Fig 20.16, page 784 and Fig 20.17, page 785. o o The fenestrated glomerular capillaries (See Fig 20.9, page 779) filter water & dissolved materials (remember plasma components) from blood. This "filtrate" is collected in Bowman's Capsule. Proteins are not filtered out of blood! b. Filtration Pressure See Figure 20.17 page 785. o Filtration is due to a force net filtration pressure 1. outward + 60 mmHg called glomerular hydrostatic pressure (GHSP) inside glomerular capillaries. 2. inward - 18 mmHg in Bowman’s capsule. 3. inward – 32 mmHg colloid osmotic pressure in glomerular capillaries. 4. Net Filtration Pressure = 10 mmHg outward c. Filtration Rate o Kidneys produce (glomerular filtration rate/GFR = ) 125 ml fluid per minute; 1. most of this is reabsorbed in tubule. 2. See Fig 20.18, page 786. d. Regulation of Glomerular Filtration Rate (GFR) Normal GFR is approximately 125ml/minute (70 kg adult male, both kidneys) primarily due to glomerular hydrostatic pressure (GHSP). GFR remains relatively constant through two mechanisms, which include: 1. Autoregulation by vasomotor center in medulla 2. Renin-angiotensin system. : II. URINARY ORGANS A. Kidney (Renal) 8. Urine Formation: d. Regulation of Glomerular Filtration Rate (GFR) Autoregulation (AR) by Vasomotor Center 1. The vasomotor center in the medulla regulates arteriole smooth muscle allowing for AR. 2. Under normal conditions, the parasympathetic autonomic nervous system (ANS) maintains AR through vasoconstriction of the afferent arteriole to decrease GFR when elevated or vasoconstriction of the efferent arteriole to increase GFR when low. 3. AR can be overridden by the sympathetic ANS during significant volume loss or gain. a. A large blood volume loss, which markedly decreases blood pressure causes vasoconstriction of afferent arterioles, decreasing GFR, which decreases urine output to conserve water. b. A large blood volume gain, which markedly increases blood pressure causes vasodilation of afferent arterioles, increasing GFR, which increases urine output to eliminate the excess water. II. URINARY ORGANS A. Kidney (Renal) 8. Urine Formation: d. Regulation of Glomerular Filtration Rate (GFR) II. URINARY ORGANS Renin-Angiotensin System See Fig 20.19, page 787. 1. A decrease in blood volume (BV) causes a decrease in blood pressure (BP), which in turn decreases the glomerular hydrostatic pressure (GHSP) and GFR. 2. Receptors in the Juxtaglomerular Apparatus (JGA) detect this decrease: a. Baroreceptors in the JG cells of the afferent arteriole (AA) detect a decrease in stretch and secrete the enzyme renin. b. The macula densa cells in the distal convoluted tubule (DCT) detect a decrease in the levels of sodium (Na+), potassium (K+), and chloride (Cl-), and further stimulate the JG cells of the AA to secrete the enzyme renin. c. In blood, renin converts the plasma protein, angiotensinogen to angiotensin I. d. Primarily in the lungs where endothelial capillaries produce angiotensin converting enzyme (ACE), ACE converts angiotensin I to Angiotensin II e. Angiotensin II targets four sites that work together to maintain sodium balance, water balance and blood pressure (which directly affects GFR). The efferent arterioles vasoconstrict, increasing GHSP, which directly increases GFR back to normal. The adrenal cortex secretes the hormone aldosterone, which targets the DCT, causing reabsorption of Na+ (and H20). This increases BV, which increases BP, which increases GHSP, and restores GFR back to normal. The posterior pituitary gland secretes the antidiuretic hormone (ADH), which targets the DCT, causing reabsorption H20. This increases BV, which increases BP, which increases GHSP, and restores GFR back to normal. The hypothalamus triggers thirst, which increases fluid intake. This increases BV, which increases BP, which increases GHSP, and restores GFR back to normal. A. Kidney (Renal) 8. Urine Formation: e. f. Tubular Reabsorption: o Definition = the process by which substances are transported from the glomerular filtrate (through the walls of the renal tubule) to blood in the peritubular caps. o Most occurs in the PCT through the process of active transport; Reabsorption of water = osmosis. See Fig 20.21, page 789. o Reabsorbed substances pass from the lumen of the renal tubule through the epithelial cells (PCT) and into the lumen of a peritubular capillary where they are returned to bloodstream. o Reabsorbed substances include: 1. glucose 2. amino acids 3. water 4. ions (sodium, chloride, phosphate, sulfate, potassium) 5. others (creatine, lactic acid. citric acid, urea, uric acid, ascorbic acid) o Substances that remain in filtrate become concentrated as water is reabsorbed. Tubular secretion: See Fig 20.20b, page 787. o o II. See Fig 20.20, page 787. URINARY ORGANS Definition = the process by which substances are transported from the blood in the peritubular caps into the DCT. Maintains ion concentrations in blood (i.e. if the blood is high in K+, K+ will be secreted into urine). A. Kidney (Renal) 8. Urine Formation: g. Regulation of urine concentration & volume o o o o o The hormone anti-diuretic hormone (ADH) promotes the reabsorption of water through the DCT and collecting ducts, preventing excessive amounts of water from being lost in the urine. This negative feedback mechanism prevents dehydration. Countercurrent Mechanism – juxtamedullary nephrons actively resorb NaCl in the ascending loop causing hypertonic medullary interstitial fluid Countercurrent Multiplier – descending loop loses water to hypertonic medulla, further increasing tonicity of medulla Vasa recta ensures NaCl stays in the medulla ADH opens water channels in DCT and CD that allows water to be resorbed by osmosis, due to the osmotic pressure set up by the juxtamedullary nephrons See Table 20.3, page 793. h. i. Excretion of wastes (Urea & Uric Acid) o Wastes are by-products of metabolism: urea from amino acid metabolism; uric acid from nucleotide metabolism. o Wastes are reabsorbed by tubules, but are then secreted back into urine & excreted. Urine Composition o o II. URINARY ORGANS A. Kidney (Renal) 95% water; other 5% includes: urea, uric acid, trace amino acids, electrolytes. 8. Urine Formation: j. Renal Clearance o Rate at which a particular chemical is removed from the plasma Inulin test Creatinine clearance test o Used to calculate GFR and efficiency by comparing blood and urine values k. Use Table 20.1, page 784 to compare the levels of various substances present in o plasma, o glomerular filtrate, and o urine. SUMMARY TABLE (Keyed at the end of this outline) Major Step in Urine Formation Location in Nephron Substances Transported and Mode of Transport From where to where? (i.e. from blood to glomerular filtrate) II. URINARY ORGANS B. Ureters are small tubes that carry urine from each kidney to the urinary bladder through peristaltic movements. 1. 2. 3. 25 - 39 cm in length; See Fig 20.1 and 20.2, page 773. retroperitoneal; Three layers: a. Inner mucosa = transitional epithelium; b. Middle muscularis = inner circular layer of smooth muscle and outer longitudinal layer (peristalsis); c. Outer serosa = fibrous CT. See Fig 20.26, page 795. C. Urinary Bladder See Fig 20.27, page 796 and Fig 20.28, page 797. 1. Location: within pelvic cavity, behind symphysis pubis; 2. Structure: a. b. c. d. 3. D. hollow, distensible, muscular organ; lined by transitional epithelium; detrusor muscle = 3 layers of smooth muscle; covered by fibrous CT. Function: storage of urine. The urethra is a tube that carries urine from the urinary bladder to the outside. See Fig 20.30 and Fig 20.31, page 798. 1. 2. Length depends on sex: a. female = 4 cm; b. male = 20 cm. Histology depends on sex: a. female = 3 layers; b. males = 2 layers. III. ELIMINATION OF URINE A. Micturition = the process by which urine is expelled from urinary bladder to outside. See Table 20.5, page 799. 1. Micturition reflex center is in sacral spinal cord 2. Parasympathetics cause detrusor muscle to contract in response to stretch of the urinary bladder. 3. External urethra sphincter (skeletal muscle) is last “doorway” to pass, and therefore micturition can be (and usually is) inhibited until released by conscious control. B. Starts at glomerulus where glomerular filtrate is collected in Bowman's capsule PCT loop of Henle DCT collecting duct (urine) minor calyx major calyx renal pelvis ureter (peristalsis) urinary bladder (micturition) urethra outside Use this flow chart as a review by adding key points where they belong (i.e. reabsorption, reabsorption of water under influence of ADH, secretion, etc.) IV. LIFE SPAN CHANGES A. B. C. D. E. F. V. Homeostatic Imbalances/Disorder of the Urinary System A. B. C. D. E. F. G. H. I. J. VI. As one ages, the following changes are seen in the urinary system: The kidneys become grainy and scarred. GFR decreases significantly as glomeruli atrophy, fill with connective tissue, or unwind. Fat accumulates on the exterior of the renal tubules, making them asymmetric. 1. Reabsorption and secretion become slow or impaired. 2. The rate of drug clearance decreases. Cardiovascular changes lead to decreased rates through urinary system. 1. The kidney: a. slows in its response to changes. b. Is less efficient at activating Vitamin D. Elasticity of urinary organs declines. 1. Changes in urination patterns result. Hemolytic uremic anemia. See introduction on page 772. Inherited kidney abnormalities. See purple box on page 773. Chronic Renal Failure. See Clinical Application 20.1, page 776. Glomerulonephritis. See Clinical Application 20.2, page 780. Nephrotic Syndrome. See Clinical Application 20.3, page 789. Gout. See purple box on page 793. Cystitis/Ureteritis. See purple box on page 795. Kidney Stones. See purple box on page 796. Bladder Cancer. See purple box on page 796. Incontinence. See purple box on page 800. Other Interesting Topics Concerning the Urinary System A. B. Dialysis. See blue box on page 774. Urinalysis: Clues to Health. See Clinical Application 20.4, page 799. VII. Innerconnections of the Urinary System: See page 801. VIII. Clinical Terms Related to the Urinary System. See page 802 Urine Formation SUMMARY TABLE Major Step in Urine Formation glomerular filtration tubular reabsorption tubular secretion Location in Nephron glomerulus primarily through proximal convoluted tubule (PCT) primarily through distal convoluted tubule (DCT) Substances Transported and Mode of Transport All plasma constituents except proteins (i.e. glucose, amino acids, water, ions, creatine, lactic acid, urea, uric aid, ascorbic acid, etc) glucose, amino acids, water, ions, creatine, lactic acid, urea, uric acid, ascorbic acid, etc. excess ions, trace amino acids, urea, uric acid From where to where? (i.e. from blood to glomerular filtrate) from blood in glomerulus to “filtrate” in Bowman’s capsule from “filtrate” in PCT to blood in peritubular capillaries from blood in peritubular capillaries to “urine” in DCT Chapter 20: Urinary System IX. I. Introduction A. The organs of the urinary system are kidneys, ureters, urinary bladder and urethra. B. The functions of the kidneys are to remove substances from blood, form urine, and to regulate certain metabolic processes. C. The function of the ureter is to carry urine from the kidneys to the bladder. D. The function of the bladder is to store urine. E. The function of the urethra is to convey urine from the bladder to the outside. X. II. Kidneys A. Introduction 1. A kidney is reddish brown in color and bean shaped. 2. A kidney is enclosed by a tough, fibrous capsule. B. Location of Kidneys 1. The kidneys are located on either side of the vertebral column in a depression high on the posterior wall of the abdominal cavity. They are positioned about the level of the 1st three lumbar vertebrae. 2. Retroperitoneally means behind the parietal peritoneum and against the deep muscles of the back. C. Kidney Structure 1. The renal sinus is a hollow chamber on the medial side of each kidney. 2. The renal pelvis is the expansion of the ureters in the kidney. 3. The renal pelvis is divided into major calyces. 4. Major calyces are divided into minor calyces. 5. Renal papillae are small projections that project into each minor calyx. 6. The renal medulla is an inner region composed of conical masses called renal pyramids. 7. Renal pyramids are divisions of the renal medulla. 8. The renal cortex is the outer region of a kidney. 9. Renal columns are cortical tissues between renal pyramids. 10. The renal capsule is a fibrous membrane surrounding a kidney. D. Functions of the Kidneys 1. The main functions of the kidneys are to regulate the volume, composition, and pH of body fluids and to remove metabolic wastes from the blood and excrete them to the outside. 2. Erythropoietin functions to regulate the production of red blood cells. 3. Renin regulates blood pressure. 4. Hemodialysis is an artificial means of removing substances from blood that would normally be excreted in urine. E. Renal Blood Vessels 1. Renal arteries arise from the abdominal aorta. 2. At rest, the renal arteries contain 15% t0 30% of the total cardiac output. 3. Renal arteries branch into interlobar arteries, which pass between renal pyramids. 4. Interlobar arteries branch into arcuate arteries. 5. Arcuate arteries branch into interlobular arteries. 6. Interlobular arteries branch into afferent arterioles. 7. Afferent arterioles lead to the nephrons. 8. Venous blood of the kidneys is returned through a series of vessels that generally correspond to the arterial pathways. 9. Renal veins join the inferior vena cava. F. Nephrons 1. Structure of a Nephron a. Functional units of the kidneys are called nephrons. b. Each nephron consists of a renal corpuscle and renal tubules. c. A renal corpuscle consists of a glomerulus and glomerular capsule. d. A glomerulus is a tuft of capillaries. e. A glomerular capsule is thin walled, saclike structure the surrounds a glomerulus. f. Afferent arterioles give rise to glomeruli, which lead to efferent arterioles. g. The two layers of the glomerular capsule are a visceral layer and a parietal layer. h. Podocytes are located in the visceral layer. i. Slit pores are cleft between podocytes. j. The renal tubule leads away from the glomerular capsule. k. The parts of the renal tubule are proximal convoluted tubule, nephron loop, and distal convoluted tubules. l. Distal convoluted tubules merge together to form a collecting duct, which empties into a minor calyx. 2. Juxtaglomerular Apparatus a. The macula densa is comprised of epithelial cells of the distal convoluted tubule that contact and are between the afferent and efferent arterioles. b. The juxtaglomerular cells are vascular smooth muscle cells in the walls of an afferent arteriole near its attachment to a glomerulus. c. The juxtaglomerular apparatus is composed of juxtaglomerular cells and macula densa cells. d. The juxtaglomerular apparatus is important in regulating the secretion of renin. 3. Cortical and Juxtamedullary Nephrons a. Cortical nephrons have relatively short nephron loops that do not reach the renal medulla. b. Juxtamedullary nephrons have corpuscles that extend deep into the medulla. c. The juxtamedullary nephrons are important in regulating water balance. 4. Blood Supply of a Nephron 1. Blood enters a glomerulus through an afferent arteriole. 2. Blood leaves a glomerulus through an efferent arteriole. 3. An efferent arteriole delivers blood to the peritubular capillary system. 4. A peritubular capillary system is located around the renal tubule. 5. Vasa recta are capillary loops that are closely associated with juxtamedullary nephrons. 6. Blood leaves the peritubular capillary system through the venous system of the kidney. XI. III. Urine Formation A. Introduction 1. The main function of the nephrons is to control the composition of body fluids and remove wastes from the blood. 2. Urine is the product produced by kidneys and contains wastes, excess water, and electrolytes. 3. The three processes involved in urine formation are glomerular filtration, tubular reabsorption, and tubular secretion. 4. In glomerular filtration, blood plasma is filtered. 5. The function of tubular reabsorption is to return most of the products filtered from plasma back to the blood. 6. The function of tubular secretion is to put waste products into the filtrate to be excreted from the kidney. B. Glomerular Filtration 1. Glomerular filtration is the process in which water and other small dissolved molecules and ions are filtered out of the glomerular capillary plasma and into the glomerular capsule. 2. Glomerular filtrate is the fluid in the glomerular capsule. 3. The normal composition of glomerular filtrate is mostly water and the same solutes as in blood plasma, except for the larger protein molecules. C. Filtration Pressure 1. The main force that moves substances through the glomerular capillary wall is the hydrostatic pressure of the blood inside. 2. Glomerular filtration is also influenced by the osmotic pressure of the blood plasma in the glomerulus and the hydrostatic pressure inside the glomerular capsule. 3. Net filtration pressure is the net effect of all forces that influence glomerular filtration and normally favors filtration at the glomerulus. 4. Net filtration can be calculated by subtracting forces opposing filtration from forces favoring filtration. D. Filtration Rate 1. The glomerular filtration rate is directly proportional to the net filtration pressure. 2. The factors that affect glomerular filtration are glomerular hydrostatic pressure, glomerular plasma osmotic pressure, or hydrostatic pressure in the glomerular capsule. 3. Normally the most important factor affecting net filtration pressure and GFR is glomerular hydrostatic pressure. 4. If the afferent arteriole constricts, net filtration pressure decreases and the filtration rate drops. 5. If the efferent arteriole constricts, net filtration pressure increases and the filtration rate rises. 6. Factors that can change the hydrostatic pressure in the glomerular capsule are obstructions in the glomerular capsule. 7. If hydrostatic pressure in the glomerular capsule becomes too high, net filtration pressure will decrease. E. Control of Filtration Rate 1. GFR may increase when body fluids are in excess and decrease when the body must conserve fluid. 2. If blood pressure and volume drop, vasoconstriction of the afferent arterioles results, which leads to a decrease in filtration pressure and GFR. 3. If excess body fluids are detected, vasodilation of the afferent arterioles results, which leads to an increase in filtration pressure and GFR. 4. Renin is secreted by the juxtaglomerular cells in response to stimulation from sympathetic nerves and pressure-sensitive cells. 5. Renal baroreceptors detect pressure. 6. In the bloodstream, renin reacts with angiotensinogen to form angiotensin I. 7. Angiotensin I is used to make angiotensin II. 8. The effects of angiotensin II are vasocontriction, increased aldosterone secretion, increased ADH secretion, and increased thirst. 9. The functions of ANP are to stimulate sodium excretion through a number of mechanisms, including increasing GFR. F. Tubular Reabsorption 1. Introduction a. Tubular reabsorption is the process by which substances are transported out of the tubular fluid, through the epithelium of the renal tubule, and into the interstitial fluid and then into the peritubular capillaries. b. Tubular reabsorption returns substances to the internal environment. c. In tubular reabsorption, substances must first cross the cell membrane facing the inside of the tubule and then the cell membrane facing the interstitial fluid. d. Active tubular reabsorption requires ATP. e. The factors that enhance the rate of fluid reabsorption from the renal tubule are the low pressure in the peritubular capillary, the increased permeability of the peritubular capillary wall, and the colloid osmotic pressure of the peritubular capillary plasma. f. Tubular reabsorption occurs throughout the renal tubules but most occurs in the proximal convoluted portion. g. Microvilli in the proximal convoluted tubule function to greatly increase the surface area exposed to the glomerular filtrate and enhance reabsorption. h. Segments of the renal tubule are adapted to reabsorb specific substances, using particular modes of transport. i. Usually all of the glucose in glomerular filtrate is reabsorbed because there are enough carrier molecules to transport it. j. The renal plasma threshold is when the plasma concentration of a substance increases to a critical level in which more substances are in the filtrate than the active transport mechanisms can handle. k. Glucose is excreted in urine when its concentration exceeds the renal plasma threshold. l. Diuresis is an increase in urine volume. m. Osmotic diuresis is when nonreabsorbed glucose in the tubular fluid draws water into the renal tubules by osmosis, thus increasing urine volume. n. Examples of substances that are reabsorbed through renal tubules are glucose, amino acids, small proteins, creatine, lactic acid, citric acid, uric acid, ascorbic acid, and many ions. 2. Sodium and Water Reabsorption a. Water reabsorption occurs by osmosis and is closely associated with the active reabsorption of sodium ions. b. If sodium reabsorption increases, water reabsorption increases. c. Much of the sodium reabsorption occurs in proximal segment of the renal tubule by active transport. d. When sodium ions move through the tubular wall, negatively charged ions move with them. e. About 70% of water and sodium may be reabsorbed before urine is excreted. f. Two hormones that affect sodium and water reabsorption are ADH and aldosterone. G. Tubular Secretion 1. In tubular secretion, substances move from the plasma of the peritubular capillary into the fluid of the renal tubule. 2. Examples of substances that are secreted into renal tubules are drugs, histamine, ammonia and various ions. 3. To summarize, urine forms as a result of glomerular filtration of materials from blood plasma, reabsorption of substances, and secretion of substances. H. Regulation of Urine Concentration and Volume 1. Aldosterone and ANP affect the solute concentration of urine. 2. The cells lining the later portion of the distal convoluted tubule and the collecting ducts are impermeable to water unless ADH is present. 3. A countercurrent mechanism ensures that the medullary interstitial fluid becomes hypertonic. 4. Chloride ions are reabsorbed in the in the ascending limb and sodium ions follow the chloride ions. 5. Tubular fluid in the ascending limb becomes hypotonic as it loses solutes. 6. Water leaves the descending limb by osmosis and NaCl enters the descending limb by diffusion. 7. Tubular fluid in the descending limb becomes hypertonic as it loses water and gains NaCl. 8. As NaCl repeats the circuit, its concentration in the medulla increases. 9. The vasa recta countercurrent mechanism helps maintain the NaCl concentration in the medulla. I. Urea and Uric Acid Excretion 1. Urea is a by-product of amino acid catabolism in the liver. 2. Urea enters the renal tubule through filtration. 3. About 50% of urea is reabsorbed but the remainder is excreted in urine. 4. Uric acid is a product of the metabolism of certain nucleic acid bases. 5. Uric acid is completely reabsorbed. 6. About 10% of the reabsorbed uric acid ends up in urine because it is secreted into the renal tubule. J. Urine Composition 1. Urine is normally composed of water, urea, uric acid, creatinine, trace amounts of amino acids and various electrolytes. 2. Factors that change urine composition are fluid intake, environmental temperature, relative humidity of surrounding air, a person’s emotional condition, respiratory rate, and body temperature. K. Renal Clearance 1. Renal clearance is the rate at which a particular substance is removed from the plasma. 2. The inulin clearance test is used to calculate the rate of glomerular filtration. 3. The creatinine clearance test is used to calculate GRF and to determine amount of renal failure. 4. The para-aminohippuric acid test is used to calculate the rate of plasma flow through the kidneys. XII. IV. Elimination of Urine A. Introduction 1. After forming in the nephrons, urine passes from the collecting ducts through openings in renal papillae and enters the calyces of the kidney. 2. From the renal calyces, urine passes through the renal pelvis into a ureters, and into the urinary bladder. B. Ureters 1. Ureters are located posterior to the parietal peritoneum and parallel to the vertebral column. In the pelvic cavity, they course forward and medially to join the bladder. 2. The three layers of the wall of a ureter are an inner mucous coat, a middle muscular coat, and an outer fibrous coat. 3. Urine is moved through ureters by peristaltic waves. 4. A renal calculus is a kidney stone. 5. The effects of ureter obstruction are to stimulate constriction of the renal arterioles and to reduce urine output. C. Urinary Bladder 1. The urinary bladder is located within the pelvic cavity, posterior to the symphysis pubis and inferior to the parietal peritoneum. 2. The trigone of the bladder consists of the opening of the urethra and the two openings of the ureters. 3. The neck of the bladder is a funnel shaped extension of the bladder that contains the opening into the urethra. 4. The four layers of the wall of the bladder are an inner mucous coat, a submucous coat, a muscular coat, and an outer serous coat. 5. The mucous coat is composed of transitional epithelial cells. 6. The submucosa consists of connective tissue and elastic fibers. 7. The muscular coat is composed of smooth muscle fibers. 8. The detrusor muscle is the collection of smooth muscle fibers in the wall of the urinary bladder. 9. The internal urethral sphincter is located in the neck of the bladder and functions to prevent the bladder from emptying until the pressure within the bladder increases to a certain level. 10. The serous coat is composed of the parietal peritoneum. D. Urethra 1. The urethra conveys urine from the bladder to the outside. 2. Urethral glands are located in the urethral wall and function to secrete mucus into the urethral canal. 3. The external urethral sphincter is located as part of the urogenital diaphragm and functions to voluntarily control urination. 4. The three parts of the male urethra are prostatic, membranous, and spongy. E. Micturition 1. Micturition is urination. 2. The muscles that contract during micturition are the destrusor muscle, abdominal wall muscles, pelvic floor muscles and the diaphragm. 3. The micturition reflex center is located in the sacral portion of the spinal cord. 4. The urgency to urinate occurs when the bladder wall distends as it fills with urine. 5. Micturition is usually under voluntary control because the external urethral sphincter is under voluntary control. XIII. V. Life-Span Changes A. With age, changes of the kidneys include shrinkage, scarring, loss of glomeruli, and a decreases ability to remove nitrogenous wastes and toxins. B. Changes of the nephron include thickening of renal tubules, shortening of renal tubules, and a decreased ability to clear drugs and other substances from the blood. C. Changes of the bladder, ureters, and urethra include loss of elasticity. D. Common reasons for incontinence are loss of muscle tone in the bladder, urethra, and ureters, and the atrophy of bladder sphincters. In males, an enlarged prostate may lead to incontinence. Chapter 20 Urinary System 1. Name the organs of the urinary system, and list their general functions. a. Kidneys—remove substances from the blood, form urine, and help regulate various metabolic processes. b. Ureters—tubes that transport urine away from kidneys to the urinary bladder. c. Urinary bladder—saclike organ that serves as a urine reservoir. d. Urethra—tube that transports urine to the outside the body. 2. Describe the external and internal structure of a kidney. Externally, a kidney is a reddish brown, bean-shaped organ about 12 centimeters long, 6 centimeters wide, and is enclosed in a smooth, tough, fibrous capsule (tunic fibrosa). The lateral surface of the kidney is convex, while its medial side is concave. The hollow depression (renal sinus) of the concave side allows blood and lymphatic vessels, and the ureter to pass through at the hilum. The ureter opens up inside the sinus to become the renal pelvis. The pelvis then divides into two or three tubes (major calyces [sing. calyx]) that further divide into eight to fourteen minor calyces. The kidney has two distinct regions, the inner renal medulla and the outer renal cortex. The renal medulla contains conical masses of tissue (renal pyramids) between the renal columns, arranged so that the bases face the convex side of the kidney and the apexes (renal papillae) project into the renal sinus. The papillae have many openings that lead into the minor calyces. The cortex is granular, and surrounds the medulla. Its tissue dips into the medulla between the renal pyramids, forming renal columns. The random arrangement of tiny tubules associated with the nephrons gives the cortex its granular appearance. 3. List the functions of the kidneys. The functions of the kidneys are: a. regulate the volume, composition, and the pH of body fluids, b. remove metabolic wastes from the blood and excrete them, c. aid control of the rate of red blood cell production by secreting erythropoietin, d. regulate blood pressure by secreting renin, and e. regulate calcium ion absorption by activating vitamin D. 4. Name the vessels the blood passes through as it travels from the renal artery to the renal vein. The route the blood follows is: renal artery to several interlobar arteries, to arciform (arcuate) arteries, to afferent arterioles, to efferent arterioles, to peritubular capillaries, to interlobular veins, to arciform (arcuate) veins, to interlobar veins, to a renal vein. 5. Distinguish between a renal corpuscle and a renal tubule. A renal corpuscle is a tangled cluster of blood capillaries called a glomerulus. The glomerulus surrounds a glomerular capsule that marks the enlarged, closed end of a renal tubule. The renal tubule contains the fluids secreted by the blood in the renal corpuscle. 6. Name the structures fluid passes through as it travels from the glomerulus to the collecting duct. Once the fluid is secreted into the renal tubule, it travels into a highly coiled proximal convoluted tubule. This tubule turns toward the renal pelvis and straightens to become the descending nephron loop. The tubule then curves back toward the renal corpuscle as the ascending nephron loop. This branch again becomes highly coiled, and is called the distal convoluted tubule. Several of these tubules converge in the renal cortex to form a collecting duct that joins with others to eventually empty into a minor calyx. 7. Describe the location and structure of the juxtaglomerular apparatus. A juxtaglomerular apparatus is located at the point were a distal convoluted tubule passes between, and contacts, the afferent and efferent arterioles. At this point, the tubule’s epithelial cells narrow and pack tightly together to form the macula densa. Nearby, the wall of the afferent arteriole contains large, vascular smooth muscle cells called juxtaglomerular cells. The macula densa and the juxtaglomerular cells, together, make a juxtaglomerular apparatus. 8. Distinguish between cortical and juxtamedullary nephrons. Nephrons located in the renal cortex are called cortical nephrons. The nephrons located close to the renal medulla have nephron loops extending into the medulla, and are thus called juxtamedullary nephrons. 9. Distinguish among filtration, reabsorption, and secretion as they relate to urine formation. Filtration moves chemicals from the glomerulus into the renal tubules by pressure. Reabsorption moves some of these chemicals back into the blood. Secretion moves other chemicals from the peritubular capillaries into renal tubules by various mechanisms. 10. Define filtration pressure. Filtration pressure is the net pressure that causes substances to move from the capillaries into the renal tubules. The calculation takes into account glomerular hydrostatic pressure (blood pressure inside the glomerulus), capsular hydrostatic pressure (fluid pressure inside the glomerular capsule), and the glomerular osmotic pressure (the amount of force the substances have in the blood to keep water inside). 11. Compare the composition of glomerular filtrate with that of the blood plasma. The glomerular filtrate has about the same composition as what becomes tissue fluid elsewhere in the body. In other words, glomerular filtrate is mostly water and contains essentially the same substances as blood plasma, except for the larger protein molecules. 12. Explain how the diameters of the afferent and efferent arterioles affect the rate of glomerular filtration. The rate of glomerular filtration is directly proportional to the filtration pressure. So, if the afferent arteriole constricts, blood flow decreases, and the filtration pressure drops. On the other hand, if the efferent arteriole constricts, the resulting back pressure will cause an increase in filtration pressure. 13. Explain how changes in the osmotic pressure of the blood plasma may affect glomerular filtration. Osmotic pressure is the amount of attraction of substances to water. When hydrostatic pressure forces water out, the remaining blood proteins exert more force to pull water back in. When the osmotic pressure is high enough, filtration stops. If blood protein concentration is low, filtration increases. If the blood flow is rapid, osmotic pressure stays low and filtration rates remain high. If the blood flow is slow, the osmotic pressure changes because the blood has more time to be filtered. 14. Explain how the hydrostatic pressure of a glomerular capsule affects the rate of glomerular filtration. The hydrostatic pressure in the glomerular capsule opposes the hydrostatic pressure in the glomerulus. If the glomerular capsule pressure is too great, as with an obstruction, filtration will decrease. 15. Describe two mechanisms by which the body regulates the filtration rate. Glomerular filtration rate (GFR) can be controlled by the renin-angiotensin system, which controls sodium excretion. Renal baroreceptors sense changes in blood pressure and act with the sympathetic nervous system to cause the juxtaglomerular cells to secrete renin when the pressure drops. The macula densa sense concentrations of sodium, potassium, and chlorid ions and causes renin secretion if any of these drop too low. The atrial natriuretic hormone (ANH) can also control GFR. When the atria stretch because of excessive pressure. This process is called autoregulation. 16. Define autoregulation. Filtration usually, and continuously, occurs simply by the physical properties of osmosis and hydrostatic pressure. This process is called autoregulation. 17. Discuss how tubular reabsorption is a selective process. Tubular reabsorption causes the composition of the filtrate to change before it is excreted as urine. For instance, glucose is present in the filtrate, but is absent in the urine. Urea and uric acid are considerably more concentrated in the urine than they are in the glomerular filtrate. This is accomplished through the epithelium of the renal tubule. 18. Explain how the peritubular capillary is adapted for reabsorption. Because the efferent arteriole is narrower than the peritubular capillary, the pressure of the blood in the capillary is relatively low. Also, the walls of the capillary are more permeable than those of other capillaries. These factors enhance the rate of fluid reabsorption. 19. Explain how epithelial cells of the proximal convoluted tubule are adapted for reabsorption. The epithelial of the proximal convoluted tubule contain microvilli that greatly increase their surface area. For this reason, most tubular reabsorption occurs here. 20. Explain why active transport mechanisms have limited transport capacities. Active transport is a highly selective mechanism. The carrier molecules can only transport certain amounts of very specific passenger molecules. For this reason, the active transport mechanism has a limited transport capacity. 21. Define renal plasma threshold, and explain its significance in tubular reabsorption. Under normal conditions there are sufficient carrier molecules to transport glucose out of the filtrate. If the glucose concentration reaches a point where active transport can no longer handle it, it is said to have reached its renal plasma threshold. Because no more glucose can be carried out, the excess will remain in the urine. This is significant because glucose draws water into the renal tubule by osmosis and results in increased urine volume. 22. Explain how amino acids and proteins are reabsorbed. Amino acids are thought to be reabsorbed by using three different active transport systems in the proximal convoluted tubules. Each active transport system reabsorbs a different group of amino acids with a similar molecular structure. The filtrate is usually free of proteins except albumin. Albumin has a relatively small structure and is reabsorbed by pinocytosis in the microvilli of the proximal convoluted tubules. From there, it is converted by enzymatic actions into amino acids and moved back into the blood of the peritubular capillaries. 23. Describe the effect of sodium reabsorption on the reabsorption of negatively charged ions. Because sodium is a positively charged ion, its reabsorption causes negatively charged ions to follow it out of the filtrate. The sodium is reabsorbed by active transport in the proximal area of the renal tubule. The negatively charged ions of chloride, phosphate, and bicarbonate follow through in passive transport systems. 24. Explain how sodium ion reabsorption affects water reabsorption. As sodium and its negative ions are reabsorbed, the solute concentration of the peritubular capillaries increases. This causes water to move into the peritubular capillary by osmosis in order to equalize the solute concentrations on both sides, and this reduces the fluid volume within the renal tubule. 25. Explain how hypotonic tubular fluid is produced in the ascending limb of the nephron loop. The ascending limb of the nephron loop is impermeable to water but diffuses electrolytes by transport mechanisms. This causes its fluid to be hypotonic with respect to the interstitial fluid surrounding it. 26. Explain why fluid in the descending limb of the nephron is hypertonic. Because the descending limb of the nephron loop is very permeable to water yet almost impermeable to solutes, its fluid is hypertonic with respect to the interstitial fluid surrounding it. 27. Describe the function of ADH. ADH (antidiuretic hormone), produced by the hypothalamus and secreted by the posterior lobe of the pituitary gland, causes water reabsorption to increase by increasing the permeability of the linings of the distal convoluted tubules and collecting ducts. This occurs in response to decreasing blood volume and pressure or decreasing concentrations of water in the blood. 28. Explain how the renal tubule is adapted to secrete hydrogen ions. Secretory mechanisms are active transport mechanisms that work in the opposite direction. The epithelium of the proximal convoluted segment actively secretes hydrogen ions along with other organic compounds. 29. Explain how potassium ions may be secreted passively. The active reabsorption of sodium ions out of the tubular fluid produces a negative charge within the tube. Because of this, in the distal portions of the proximal convoluted tubule and the collecting duct, potassium ions (which are positively charged) move from the tubular epithelium and into the tubular fluid by electrical attraction. 30. Explain how urine may become concentrated as it moves through the collecting duct. In response to certain metabolic conditions such as decreasing blood or fluid volume, the posterior lobe of the pituitary gland releases ADH (antidiuretic hormone). In the kidney, ADH causes increased permeability of the epithelial linings of the distal convoluted tubule and collecting duct. This moves water rapidly out of these segments. Thus, the urine becomes more concentrated because water is conserved by the body. 31. Compare the processes by which urea and uric acid are reabsorbed. About fifty percent of urea is reabsorbed by passive diffusion in the renal tubule. The rest is secreted in the urine. Uric acid is reabsorbed by active transport. Although all of the uric acid is reabsorbed, about ten percent is secreted in the urine. This seems to be a result of the acid being secreted back into the renal tubule. 32. List the more common substances found in urine and their sources. a. Water—excess intake and cellular metabolism. b. Urea—a by-product of amino acid catabolism. c. Uric acid—a by-product of organic base and nucleic acid metabolism. d. Amino acids--protein synthesis or breakdown. e. Electrolytes--various body processes. 33. List some of the factors that affect the volume of urine produced each day. These factors include: amount of fluid intake, environmental temperature, relative humidity of surrounding air, the person's emotional condition, respiratory rate, and body temperature. 34. Describe the structure and function of a ureter. A ureter is a tubular organ, approximately 25 centimeters long. It begins as the funnelshaped renal pelvis, extends downward behind the parietal peritoneum and parallel to the vertebral column. In the pelvic cavity, it moves medially and anteriorly, to join the urinary bladder from underneath. The wall of the ureter has three layers: a. Mucous coat—the inner layer, it is continuous with the linings of the renal tubules and the urinary bladder. b. Muscular coat—the middle layer consisting largely of smooth muscle. c. Fibrous coat—the outer layer, it consists of connective tissue. The ureter functions to pass urine from the kidneys into the urinary bladder. 35. Explain how the muscular wall of the ureter aids in moving urine. The smooth muscle layer produces peristaltic waves originating from the renal pelvis and forcing urine along the ureter into the urinary bladder. 36. Discuss what happens if a ureter becomes obstructed. If the ureter becomes obstructed, peristaltic waves strengthen at the proximal end of the tube helping to push the obstruction into the bladder. Concurrently, the ureterorenal reflex constricts the renal arterioles and decrease urine production in that kidney. 37. Describe the structure and location of the urinary bladder. The urinary bladder is a hollow, distensible, muscular organ located within the pelvic cavity, just posterior to the symphysis pubis, and inferior to the parietal peritoneum. It is somewhat spherical in shape and when empty, contains many folds. Internally, the floor of the bladder contains a triangular area called the trigone that has openings at each of the three points. At the base of the trigone, are the openings for the ureters, and anteriorly, the bladder has a short, funnel shaped extension called the neck of the bladder that contains the opening to the urethra. The bladder wall consists of four layers: a. Mucous coat—the innermost layer, it contains several layers of transitional epithelial cells. b. Submucous coat—the second layer, it consists of connective tissue and elastic fibers. c. Muscular coat—this layer contains coarse bundles of smooth muscle fiber. Together these muscles comprise the detrusor muscle. d. Serous coat—the outermost layer, it is synonymous with the parietal peritoneum. This layer occurs only on the upper surface of the bladder. Elsewhere, the outer coat is comprised of fibrous connective tissue. 38. Define detrusor muscle. The detrusor muscle is the muscle layer of the bladder. Part of this muscle surrounds the neck of the bladder and forms the internal urethral sphincter. The sustained contraction of this muscle prevents urine from passing into the urethra until the pressure within the bladder reaches a certain level. 39. Distinguish between the internal and external urethral sphincters. The internal urethra sphincter is composed of smooth muscle that surrounds the neck of the bladder. It is controlled involuntarily. The external urethral sphincter is part of the urogenital diaphragm and is located about three centimeters below the bladder and surrounding the urethra. It is composed of skeletal muscle tissue and is therefore controlled voluntarily. 40. Compare the urethra of a female with that of a male. Structurally, urethras in both males and females are internally lined with a mucous membrane containing numerous mucous glands (urethral glands) and are surrounded by a thick layer of longitudinal smooth muscle fibers. The female urethra is about 4 cm long and travels forward from the bladder, below the symphysis pubis, and empties from the external urethra orifice (urinary meatus)—anterior to the vaginal opening and 2.5 cm posterior to the clitoris. In the male, the urethra functions as a urinary canal and a passageway for secretions and cells of the reproductive organs. It contains three sections: a. Prostatic urethra—about 2.5 cm long, it passes from the bladder through the prostate gland. Ducts from the reproductive structures empty here. b. Membranous urethra—about 2 cm long, it begins just distal to the prostate gland passing through the urogenital diaphragm. It is surrounded by fibers of the external urethral sphincter muscle. c. Penile urethra—about 15 cm long, it passes through the corpus spongiosum of the penis ends at the tip of the penis with the external urethral orifice. 41. Describe the micturition reflex. The micturition reflex (urination) involves the contraction of the detrusor muscle and relaxation of the external urethral sphincter. When the bladder is sufficiently distended with urine, stretch receptors in the wall of the bladder signal the micturition reflex center in the spinal cord to send a motor impulse along the parasympathetic nerves to the detrusor muscle. 42. Explain how the micturition reflex can be voluntarily controlled. Because the external urethral sphincter is composed of skeletal muscle, its contraction and relaxation can be consciously controlled until the decision to urinate is made. This control is aided by nerve centers in the brain stem and cerebral cortex that can partially inhibit the micturition reflex. Nerve centers within the pons and hypothalamus function to make the micturition reflex more effective. 43. What changes occur in the urinary system with age? The kidneys are slower to remove nitrogenous wastes and toxins and to compensate for changes to maintain homoestasis. From the outside, the kidneys change with age, appearing scarred and grainy as arterioles serving the cortex constrict, and fibrous connective tissue accumulates around the capsules. On the inside, kidney cells begin to die as early as age 20 years, but the gradual shrinkage is not generally noticeable until after age 40. By 80 years, the kidneys have lost about a third of their mass. Further along the nephron, the renal tubules thicken, accumulating coats of fat. The bladder, ureters, and urethra change with the years too. These muscular organs lose elasticity and recoil with age, so that in the later years, the bladder holds less than half of what it did in young adulthood, and may retain more urine after urination. In the elderly, the urge to urinate may become delayed, so that when it does happen, it is sudden. Older individuals have to urinate at night more than younger people.