Alternatives to Quetiapinein presentation slides
advertisement

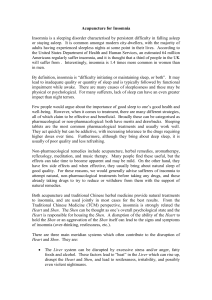
NC Academic Consortium for Cost Effective Pharmacologic Treatment Cost Effective Options in the Treatment of Insomnia: A Presentation from NC-ACCEPT: The NC Academic Consortium for Cost Effective Psychopharmacologic Treatment Supported by Community Care of NC and the NC AHEC Program 1 W. Vaughn McCall, M.D., M.S. Wake Forest Baptist Medical Center Revised 5/10/2011 NC Academic Consortium for Cost Effective Pharmacologic Treatment The four academic departments of psychiatry in North Carolina at the University of NC at Chapel Hill, Eastern Carolina, Wake Forest and Duke University and the North Carolina Psychiatric Association with the support of Community Care of North Carolina and the North Carolina Area Health Education Center Program are committed to conserving resources and improving psychiatric medication prescribing. Toward that effort we formed NC ACCEPT: The North Carolina Academic Consortium for Cost Effective Psychopharmacologic Treatment. The goal of NC ACCEPT is to engage in a dialogue about cost effective use of psychiatric medications with clinicians and trainees in psychiatry and primary care. By promoting discussion about evidence-based approaches to prescribing we will encourage appropriate use of generic medications, reduce unnecessary use of multiple medications, and encourage discontinuing medications when they are no longer needed. NC Academic Consortium for Cost Effective Pharmacologic Treatment Objectives • • • The participant will be able to describe the role of insomnia as a risk factor for incident psychiatric illness The participant will be able to discuss the impact of insomnia on the course of psychiatric illness The participant will be able to propose a variety of strategies for managing insomnia NC Academic Consortium for Cost Effective Pharmacologic Treatment There are no disclosures to be made for this program. This program did not receive any commercial support. NC Academic Consortium for Cost Effective Pharmacologic Treatment NC Academic Consortium for Cost Effective Pharmacologic Treatment $60,000,000 $50,000,000 $50,799,374 $40,000,000 Top 15 NC Medicaid (DMA) Medication Expense Items FY 2010 By Medication (all strengths of medication aggregated) $39,018,801 $30,000,000 $30,292,268 $20,000,000 $20,901,793 $17,850,045 $16,354,412 $14,452,879 $10,000,000 $12,194,509 $10,137,283 $14,669,114 $17,213,592 $0 $13,354,291 $12,081,078 $9,573,614 $9,226,600 NC Academic Consortium $9,000,000 $8,000,000 Comparison of Aggregated Seroquel Use NC-DMA SFY 2009 and 2010 for Cost Effective Pharmacologic Treatment $8,996,827 $8,443,635 $7,000,000 $6,000,000 $6,271,970 $7,508,502 $5,861,869 $5,000,000 $3,669,153 $4,000,000 $3,000,000 $2,000,000 $2,385,850 $2,517,088 $4,222,352 $3,807,541 $4,292,262 $4,277,316 $2,554,187 $1,834,008 $2,372,354 $1,000,000 $0 SEROQUEL 25 SEROQUEL XR SEROQUEL XR MG 400 MG 300 MG SEROQUEL 400 MG SEROQUEL 50 MG SFY 2009 Units SFY 2010 Units SFY 2009 Dollars SFY 2010 Dollars SEROQUEL 100 MG SEROQUEL 200 MG SEROQUEL 300 MG $8,561,724 NC Academic Consortium for Cost Effective Pharmacologic Treatment Question #1 • The most common cause of chronic insomnia is: a) psychiatric illness b) medical illness c) primary insomnia NC Academic Consortium for Cost Effective Pharmacologic Treatment Percent of Patients DSM-IV Diagnoses in Chronic Insomnia 50 45 40 35 30 25 20 15 10 5 0 N=216 Mental Disorder Primary Insomnia DSPS=delayed sleep phase syndrome OSAS=obstructive sleep apnea syndrome Buysse DJ et al. Am J Psychiatry. 1994;151: 1351-1360 DSPS OSAS Medical Disorder NC Academic Consortium for Cost Effective Pharmacologic Treatment Psychiatric Correlates of Insomnia Insomnia as a Precursor to Psychiatric Disorder • • • 1. 2. Unresolved insomnia ↑ the odds of new Ψ disorder over one year (especially major depression episode (MDE) and panic disorder)1 Unclear whether preceding insomnia is an early symptom of MDE or a modifiable risk factor Sleep deprivation (insomnia?) is probably a modifiable risk factor for mania2 Ford and Kamerow JAMA 1989 Wehr et al NC Academic Consortium for Cost Effective Pharmacologic Treatment Persistent Insomnia and Subsequent Psychiatric Disorders Any Psychiatric Disorder Major Depression Anxiety Disorders Alcohol Abuse % Patients 40 35 33.6 30 25 25.6 20 15 10 5 0 12.7 0.6 2.5 7.4 Resolved Insomnia 14 * Unresolved Insomnia At 1-Year Follow-Up Adapted from Ford DE and Kamerow DB, 1989. 3.4 NC Academic Consortium for Cost Effective Pharmacologic Treatment Psychiatric Correlates of Insomnia Insomnia During MDE • • Insomnia is an independent contributor towards poor quality of life in depressed patients1 Insomnia intensity is related to suicidal ideation intensity in depressed patients, and is predictive of suicide in some studies2 1. McCall WV, Reboussin BA, Cohen W. Subjective measurement of insomnia and quality of life in depressed inpatients. J Sleep Res 2000; 9:43-48. 2. McCall WV, Blocker JN, D’Agostino, Jr R, Kimball J, Boggs N, Lasater B, Rosenquist, PB. Insomnia Severity is an Indicator of Suicidal Ideation During a Depression Clinical Trial. Sleep Medicine 2010;11:822-827 NC Academic Consortium for Cost Effective Pharmacologic Treatment Question #2 • The most common residual symptom in an otherwise successfully SSRI-treated case of depression is: a) b) c) sad mood insomnia poor appetite NC Academic Consortium for Cost Effective Pharmacologic Treatment 50 45 40 35 30 25 20 15 10 5 0 lI de at io n io n ra t Su ce nt ic id a ui lt G C on Fa tig ue ee Ps p yc ho m ot or Sl ei gh t W In te M re st Subthreshold Threshold oo d % of Remitting Subjects (n=108) Frequency of Major Depressive Disorder Residual Symptoms Among Remitters (HAMD-17 7) After 8 Weeks of Treatment Nierenberg AA, et al. J Clin Psychiatry. 1999;60(4):221-225. Patients with MDD (N=215) received a fixed dose of fluoxetine 20 mg for 8 weeks. Presence of residual symptoms not predicted by baseline demographic characteristics or Axis I and Axis II comorbid conditions. NC Academic Consortium for Cost Effective Pharmacologic Treatment Co-administration of a sleep aid with an antidepressant is the rule, not the exception • What are the implications of hypnotics co-administered with antidepressants? – 60% of sertraline and fluoxetine patients were prescribed something for sleep • Cook and Conner (1995): Clin Drug Invest NC Academic Consortium for Cost Effective Pharmacologic Treatment Question #3 • Complications of residual insomnia after treatment of depression include: a) b) c) metabolic syndrome low serum cortisol increased rate of depressive relapse NC Academic Consortium for Cost Effective Pharmacologic Treatment Psychiatric Correlates of Insomnia Insomnia after MDE Residual insomnia in otherwise successfully treated cases of depression – Is predictive of relapse1 1. Reynolds, Am J Psychiatry, 1997 NC Academic Consortium for Cost Effective Pharmacologic Treatment Evaluation of Persistent Insomnia in Psychiatric Disorder • • • • • Incomplete response Iatrogenesis Medical disorder Primary sleep disorder Poor sleep habits – conditioned insomnia NC Academic Consortium for Cost Effective Pharmacologic Treatment Ancillary Assessment of Insomnia • • • • Sleep Logs Psychometric Tests Blood Work Polysomnography NC Academic Consortium for Cost Effective Pharmacologic Treatment Sleep Logs • Sleep logs record bedtime, sleep latency, number and duration of wakenings, and up time. They also include substance use and naps. NC Academic Consortium for Cost Effective Pharmacologic Treatment Blood Work in the Assessment of Insomnia • Thyroid panels are commonly obtained in chronic insomnia evaluations, but thyroid abnormalities have not been shown to be more common in insomniacs than in good sleepers • A ferritin, B12, and thyroid panel are warranted in insomnia secondary to Restless Leg Syndrome. NC Academic Consortium for Cost Effective Pharmacologic Treatment The Role of Polysomnography in the Assessment of Insomnia • Polysomnography (PSG) is generally not indicated in the assessment of insomnia1 • PSG may be justified if excessive daytime sleepiness is also present, or if there is high clinical suspicion for sleep apnea, periodic limb movement disorder, nocturnal hypoxemia, or refractory insomnia2 1. Sleep 1995;18:35-37 2. McCall WV, Blocker JN, D’Agostino, Jr R, Kimball J, Boggs N, Lasater B, Rosenquist, PB. Insomnia Severity is an Indicator of Suicidal Ideation During a Depression Clinical Trial. Sleep Medicine 2010;11:822-827 NC Academic Consortium for Cost Effective Pharmacologic Treatment Non-pharmacologic Treatment of Insomnia • Includes changes in diet and activity such as elimination of caffeine and alcohol • Includes specific behavioral therapies such as sleep restriction and stimulus control therapy, which when combined is called CBT-Insomnia (CBT-I) • CBT-I is efficacious in controlled clinical trials of primary insomnia, and some early evidence for efficacy in psychiatric insomniacs 1,2 1. Sleep 1999;22:1134 2. J Clin Psychiatry 1998;59:693-699 NC Academic Consortium for Cost Effective Pharmacologic Treatment CBT for insomnia versus temazepam 30mg in primary insomnia of the aged Figure 2. Changes in Wake After Sleep Onset From Pretreatment to Posttreatment as Measured by Sleep Diaries and Nocturnal Polysomnography Sleep diary data are based on 2 weeks of self-monitoring at baseline (before treatment) and the last 2 weeks of treatment. Morin, C. M. et al. JAMA 1999;281:991-999 Copyright restrictions may apply. NC Academic Consortium for Cost Effective Pharmacologic Treatment Prescribed Pharmacologic Treatment of Insomnia • On-label – Benzodiazepines – Benzodiazepine receptor agonists – Melatonin receptor agonists – Low dose TCA • Off-label (partial list) – Quetiapine – Trazodone – Mirtazapine – Gabapentin NC Academic Consortium for Cost Effective Pharmacologic Treatment Clonazepam (CLZ) for insomnia secondary to depression • In 80 depressed patients receiving fluoxetine, the coadministration of CLZ 0.5-1.0 QHS for 21 days was superior to placebo in improving HRSD sleep items over 3 weeks1 • In 50 depressed patients receiving fluoxetine, the coadministration of CLZ 0.5-1.0 QHS for 18 weeks was superior to placebo in HRSD sleep items only for the first 3 weeks2 1. Londborg PD et al, 2000 2. Smith WT et al, 2002 NC Academic Consortium for Cost Effective Pharmacologic Treatment Is Extended Clonazepam Cotherapy of Fluoxetine Effective for Outpatients with Major Depression? HAM-D Score Smith WT, et al. J Affect Disord. 2002; Aug; 70(3): 251-259 0 14 42 Day Number 84 126 NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Benzodiazepines • Pros – Some are FDA approved for sleep (not clonazepam) – inexpensive • Cons – Tolerance, dependence – Daytime sleepiness, delayed reaction time – Falls, amnesia, behavioral disinhibition NC Academic Consortium for Cost Effective Pharmacologic Treatment Zolpidem as add-on Tx for SSRI in Depression • 190 patients already on SSRIs for a number of weeks who had persistent insomnia were randomized to have either zolpidem 10 mg or placebo as add on therapy • Improvement in “Global Well Being” • Improvement in sleep • Non-significant improvement in depression NC Academic Consortium for Cost Effective Pharmacologic Treatment HAM-D Total Score- Change from Baseline Zolpidem for Persistent Insomnia in SSRI-Tx Depressed Patients 0 N=190 week 1 week 2 week 3 week 4 -0.5 -1 zolpidem placebo -1.5 -2 -2.5 -3 Asnis GM, et al. J Clin Psych. 1999; Oct; 60(10): 668-676 P=NS NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of zolpidem-immediate release • Pros – FDA indicated for sleep – Useful in depressed patients – Inexpensive • Cons – Approved for short-term use only – A controlled substance possibly with tolerance and dependence – Hallucinations, falls, cognitive problems NC Academic Consortium for Cost Effective Pharmacologic Treatment Change from Baseline in HAM-D17 (LOCF) (N=545) All Items LS Mean Change Week 4 Excluding Insomnia Items Week 4 Week 8 0 0 -2 -2 -4 -4 -6 -6 -6 -6.7 -8 -8 -10 -12 -10.9 p=0.01 -12.9 -14 -16 -8.4 -8 -9.6 p=0.02 -10 -12 Week 8 p=0.16 -9.5 p=0.04 -14 Placebo+Fluoxetine -16 Eszopiclone+Fluoxetine NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Eszopiclone • Pros – FDA approved for sleep – Indicated for open-ended use – Several positive studies in depressed and anxious insomniacs • Cons – A controlled substance – Possible tolerance and dependence – Expensive NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Ramelteon • A Melatonin-1 receptor agonist • Pros – Mild efficacy for sleep onset – No liability for tolerance or dependence – No effects on cognition or balance • Cons – No efficacy for sleep maintenance – Expensive NC Academic Consortium Low dose doxepin (a TCA) for Cost Effective Pharmacologic Treatment Roth et al. Sleep 2007, 30:1555-1561 NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Low Dose Doxepin • Pros – FDA approved for sleep – Effective for sleep maintenance problems – Not a controlled substance – Approved for open-ended duration of use – Inexpensive as the generic, down to 10 mg capsules • Cons – Not particularly effective for sleep onset problems – Despite it being a TCA, not yet studied as an add-on to SSRIs – Expensive as the branded Silenor™ at 3 and 6 mg NC Academic Consortium for Cost Effective Pharmacologic Treatment MADRS Insomnia item in depressed insomniacs Rx FLX with and without Quetiapine Garakani et al. Int Clin Psychopharm 2008;23:269-275 © 2008 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2 NC Academic Consortium for Cost Effective Pharmacologic Treatment Weight gain and EPS effects of Low dose Quetiapine • 43 patients of mixed diagnoses received quetiapine 100 mg at bedtime for insomnia, as an add-on to other stabledosed psychotropics. At the end of 11 months, average weight gain was 5 pounds1 • Two patients are described who received quetiapine 2550 mg as add-on therapy for insomnia, and both developed akathisia2 1. Cates et al. Community Mental Health J. 2009;45:251-254 2. Catalano et al. Psychosomatics 2005;46:291-301 NC Academic Consortium for Cost Effective Pharmacologic Treatment $60,000,000 $50,000,000 $50,799,374 $40,000,000 Top 15 NC Medicaid (DMA) Medication Expense Items FY 2010 By Medication (all strengths of medication aggregated) $39,018,801 $30,000,000 $30,292,268 $20,000,000 $20,901,793 $17,850,045 $16,354,412 $14,452,879 $10,000,000 $12,194,509 $10,137,283 $14,669,114 $17,213,592 $0 $13,354,291 $12,081,078 $9,226,600 $9,573,614 NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Quetiapine • Pros – Several studies showing sleep benefit in depressed patients – Not a controlled substance • Cons – Not FDA indicated for sleep – Metabolic effects possible at low doses – Akathisia possible at low doses – Effects of low doses on cognition and balance are unknown – Very expensive NC Academic Consortium for Cost Effective Pharmacologic Treatment Low-dose Trazodone (50-100 mg) in depressed and nondepressed insomniacs with self report and PSG • • • 1. 2. 3. In non-depressed insomniacs, it is comparable to zolpidem for the first week by patient-report, but somewhat weaker the second week.1 In non-depressed insomniacs, it is associated with improved alertness the morning after dosing, compared with placebo.2 In depressed insomniacs on SSRIs, TRZ is associated with improved self-reported sleep, as compared with placebo.3 Walsh et al. Human Psychopharmacology 1998;13191-198 Roth A, McCall WV, Ligouri A. (in press) Nierenberg AA et al. Am J Psychiatry 1994; 151:1069-1072 NC Academic Consortium for Cost Effective Pharmacologic Treatment New Data on Trazodone: Alertness, Memory, and Motor stamina NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Trazodone • Pros – Effective for insomnia in some patients – Not a controlled substance – May improve alertness – Inexpensive • Cons – Not FDA approved for sleep – Adverse memory effects? – Priapism (unlikely at low doses) NC Academic Consortium for Cost Effective Pharmacologic Treatment Mirtazapine 30 mg • • 1. 2. Mirtazapine mono-therapy improves self-reported sleep in depressed insomniacs in an open trial.1 Mirtazapine mono-therapy improves PSG- sleep in depressed insomniacs in an open trial.2 Winokur et al. Biol Psych 2000; 48:75-78 Shen et al. Can J Psychiatry 2006;51:27-34 NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Mirtazapine • Pros – Effective for sleep – Not a controlled substance – Inexpensive • Cons – Not FDA approved for sleep – Weight gain is possible NC Academic Consortium for Cost Effective Pharmacologic Treatment Gabapentin 300 bid and 600 qhs in 33 abstinent alcoholics Mason et al. Addict Biol.2009;14:73-83 NC Academic Consortium for Cost Effective Pharmacologic Treatment Gabapentin 300 bid and 600 qhs in 33 abstinent alcoholics Mason et al. Addict Biol.2009;14:73-83 NC Academic Consortium for Cost Effective Pharmacologic Treatment Gabapentin 1500 mg versus placebo qhs in 21 abstinent alcoholics over 6 weeks: Better sleep was associated with better drinking outcomes Brower et al. Alcohol Clin Exp Res 2008;32:1429-1438 NC Academic Consortium for Cost Effective Pharmacologic Treatment Pros and Cons of Gabapentin • Pros – May be helpful in sleep of alcoholics – May curb alcoholic cravings – Is not a controlled substance – Excreted unchanged by the kidneys – Inexpensive • Cons –? NC Academic Consortium for Cost Effective Pharmacologic Treatment Alternatives to Quetiapine for insomnia Summary • Taking a careful sleep history, and identifying opportunities to limit time in bed, limit naps, and fix wake up time are key • Manage unreasonable sleep expectations • Consider generic zolpidem, trazodone, doxepin, mirtazapine, and gabapentin • Gabapentin is emerging as a favored treatment for insomnia associated with alcoholism NC Academic Consortium for Cost Effective Pharmacologic Treatment Supplemental Slides Cost Effective Options in the Treatment of Insomnia NC Academic Consortium for Cost Effective Pharmacologic Treatment Quetiapine Philip NS et al. Ann Clin Psychiatry. 2008 Jan-Mar;20:15-20 • Background: Inpatient orders at Butler Hospital (Brown University) for quetiapine were obtained from October 2004 to March 2006 and divided into standing or prn . • RESULTS: The most common diagnoses in patients receiving standing dose quetiapine were depressive disorders, followed by substance-related, bipolar, and psychotic disorders with a median dose of 200 mg/day. Only 28.5% of patients had one of the diagnoses for which quetiapine is approved. • Patients receiving prn dosing had a similar distribution of diagnoses. The most common prn dose was 50 mg, given for agitation or insomnia. NC Academic Consortium for Cost Effective Pharmacologic Treatment Insomnia in Older Patients • Sleep subjectively lightens with age, with more wake time after sleep • • • • onset, and more light sleep seen in the polysomnogram . However, these age-related changes by themselves do not constitute insomnia Insomnia diagnoses should be reserved for those who are significantly distressed, and/or have corresponding daytime symptoms The rates of unanticipated primary sleep disorders (such as sleep apnea) increase with age. Therefore, insomnia ‘treatment-failure’ may justify a laboratory exam CBT for insomnia has been proven to be effective in older persons If medications are prescribed for sleep, then lower doses are recommended NC Academic Consortium for Cost Effective Pharmacologic Treatment Non-prescription drugs for insomnia • Diphenhydramine and doxylamine (Tylenol PM; Unisom) – Efficacy may not be sustained – May have daytime hangover, but no efficacy – Significant anticholinergic effects • Melatonin – Helpful for circadian rhythm problems, but low efficacy for standard insomnia problems • Valerian root – Several studies supporting efficacy, few side effects – Variable quality of the product NC Academic Consortium for Cost Effective Pharmacologic Treatment Chloral hydrate • Sustained efficacy beyond a few nights has not been proven • Hepatotoxic • More respiratory depression in overdose, as compared with benzodiazepines NC Academic Consortium for Cost Effective Pharmacologic Treatment Study Schematic for Hypnotic Treatment of GAD Screening Double-blind Treatment Run-out Open-label Escitalopram 10mg Eszopiclone 3 mg Single-blind PBO Single-blind PBO Placebo V1 Window Week -2 V2 7-10 V3 7 0 V4 7 1 V5 14 2 V6 14 4 Daily Sleep Diary Randomize N = 700 randomized / 420 complete V7 14 6 V8 14 8 10 NC Academic Consortium Disposition for Cost Effective Pharmacologic Treatment Screened Patients N=945 Randomized N=595 LEX + Placebo N=301 Discontinued Adverse Event Lost to follow up Protocol Viol Insomnia Rx Fail Other N=68 N=17 N=18 N=12 N=3 N=18 Completed N=233 77.4% LEX + Eszopiclone N=294 22.6% 5.6% 6.0% 4.0% 1.0% 6.0% Discontinued Adverse Event Lost to follow up Protocol Viol Insomnia Rx Fail Other N=65 N=16 N=17 N=11 N=2 N=19 Completed N=229 77.9% 22.1% 5.4% 5.8% 3.7% 0.7% 6.4% NC Academic Consortium for Cost Effective Pharmacologic Treatment Change from Baseline in HAM-A Key Secondary #2 (Wk 8) Week of Study 1 2 4 6 8 10 LS Mean Chg 0 -2 -4 -6 * -8 -10 -12 * * -14 Week 10 = SBRO *p<0.05 vs placebo * * * Placebo+LEX Eszopiclone+LEX p values reflect results from change from baseline analyses using ANCOVA NC Academic Consortium for Cost Effective Pharmacologic Treatment Change from Baseline in HAM-A Excluding Insomnia Item Week of Study 1 2 4 6 8 10 LS Mean Chg 0 -2 -4 -6 -8 -10 * -12 Week 10 = SBRO * * * Placebo+LEX Eszopiclone+LEX *p<0.05 vs placebo p values reflect results from change from baseline analyses using ANCOVA