Rebuilding the Foundation of Prosperity October 2, 2008
advertisement

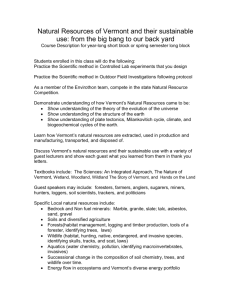
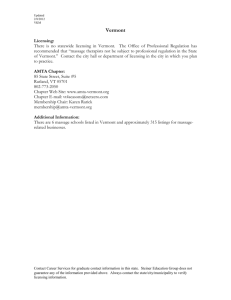
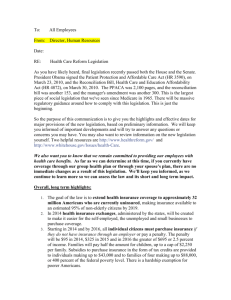
Health Care Insecurity: Roadblock to Prosperity Choices for Vermont: Rebuilding the Foundation of Prosperity October 2, 2008 Health Care Insecurity: Roadblock to Prosperity • Current health care financing in Vermont • Health care financing and the broader economy • Opportunities for reform How Health Care is Financed • Three ways to look at this – Where the money comes from – Intermediaries (where it visits along the way) – Where it ultimately winds up Where the Money Comes From • All money for health care originates in households • It flows into the system through 3 main channels – Taxes – Premiums – Out-of-Pocket (direct payments to providers) • And one smaller one - philanthropy Where the Money Comes From – Out-of-Pocket • Out-of-Pocket (OOP) includes – Cost sharing, like deductibles, coinsurance, and copayments – Payments for services not covered by insurance – ALL payments by the uninsured • In Vermont, about $490 million of the $3.9 billion in health care spending (12.5%) is OOP (2006). Where the Money Comes From – Premiums and Taxes • Straghtforward: – Taxes pay for public programs like Medicare and Medicaid – Premiums pay for private insurance like MVP and Blue Cross • Not so straightforward – What about public employees? – What about Medicare and Medicaid premiums? Premiums and Taxes • So what’s the difference? • Taxes are – Mandatory – Linked (usually) to ability to pay • Premiums are – Voluntary – Sometimes (not always) linked to expected consumption of health care services Premiums and Taxes • In 2006, Medicare, Medicaid, and other state and federal programs (mostly tax-financed) paid about $1.8 billion (46%) of Vermont’s health care bill • Private insurance and self-insured employers paid about $1.6 billion (41%). • Payments on behalf of public employees (included in private above) were about $360 million (9% of total spending). Intermediaries • Private – Employers – Health Insurers • Public – Medicare – Medicaid Where the Money Goes • Providers • Payers – Administration – Reserves – Profits Funds Flows Health Care Financing and Vermont’s Economy • Issue Areas – Health care costs are consuming a larger and larger share of resources – Costs of health insurance for private sector entities are embedded in the costs of their goods and services, not explicitly financed – These costs are extremely difficult for employers to control – Employers and employees must trade off wage increases and benefits – Retiree health costs are an increasing burden Health Care Financing and Vermont’s Economy • Health care costs are consuming a growing share of individuals’, employers’, and governments’ revenues • This leaves less and less for other expenses • For example, adjusted for inflation, the per capita income in Vermont rose by about $5,000 between 1997 and 2006. About $2,000 of that was consumed by increasing health care costs. Health Care Financing and Vermont’s Economy • Between 1997 and 2006, total personal income in Vermont grew about 5.3% per year. • During that period, health care spending grew at an average annual rate of 9.2%. • The share of personal income spent on health care grew from 13% to 18%. • At that rate, in another 10 years, we’ll spend one-quarter of all personal income on health. Health Care Financing and Vermont’s Economy • The problem of averages – Unlike many costs, such as food or heat (!), health care costs vary enormously in a population. – The healthier half of a typical population accounts for less than 5% of all costs – About 70% of all health care spending is accounted for by 10% of the population. Health Care Financing and Vermont’s Economy • Health care costs affect different families quite differently – For those with employer-sponsored insurance, their contributions are rising between 10% and 20% per year, benefits are being reduced, and wage increases are traded off for coverage. – For those who purchase insurance directly, costs are rising and the only products remaining in the market are high-deductible ($3,500 or more) Health Care Financing and Vermont’s Economy • Health care costs affect different families quite differently – For those with no insurance, a single episode of illness can lead to financial ruin. – The uninsured often go without preventive care, increasing their risks. State Government – an Illustration • In the first year, assume a state budget of $1 billion, 10% of which is spent on health care programs. • Assume state revenues grow at 4% per year and health care costs grow at 10% per year (both are historical averages). No new revenue sources. • In 25 years, health care costs will consume ALL new revenue. State Government Spending Illustration Private Sector Costs • Under the current system, health care costs are a cost of doing business for employers. – This is true whether you believe that employers pay for health care or that employees pay the full cost • These costs are included in the price that the employer charges for goods or services • As health care costs rise rapidly in the US, this makes international competition more difficult Can Employers Control Health Care Costs? • Perhaps in some ways, but their influence is small compared to cost trends • If costs can not be controlled, either the employer’s product becomes more expensive or part of the increase is passed on to employees – Increased contribution to premium – Increased cost sharing / reduced benefits The Wage / Benefit Tradeoff • Most economists look at health benefits as one part of total compensation. – The cost to the employer is the same whether the employer pays the employee $5,000 in cash or $5,000 in benefits, but the benefit is tax-free to the employee (and thus worth more) – But cash is much easier to control • Increases in health care costs will often create a trade-off, under which wage increases are smaller, or wages remain flat Retiree Benefits – Direct Spending • Demographics are changing – the number of retirees relative to the number of active employees is increasing sharply • Combined with increasing health care costs, retiree health spending is growing dramatically • Recent automaker / UAW deals Retiree Benefits – Other Effects • Until recently, both private and public employers included only the “current” costs of retiree health benefits on their balance sheets – The amount they pay in the current year • Now, they have to show the liability for future costs on their balance sheets – FAS 106 and GASB 45 • This has a major impact on their financial status Reform Options • What is it that we want to reform? – Financial • Control rate of growth • Equity of contribution – Access • “Universal” • Coverage • Care – Quality of Care Reform Options • The cost of insurance and the cost of care – Historically, insurance costs have gone up faster than underlying health care costs – Several factors contribute to this, including: • Cost shifting • Adverse selection • Benefit structures – In addition to the basic affordability issue, this leads more people (usually healthier) to drop their coverage, increasing insurance costs even faster. How Far Can a State Go? • Limits to a state’s ability to reform its health care system – Federal law • ERISA • Medicare • Medicaid – Border crossing – Status quo Political Complexities • Are you willing to change how your care is financed and delivered in order to support health care reform? • Polarization and over-simplification – “Markets” vs. “Socialized medicine” Reform in Vermont • Long history of reform – Several efforts to achieve or move toward universal access and cost containment • • • • • Governor Aiken inaugural address, January, 1939 Daniels Commission, 1975 VHIP Governor’s Blue Ribbon Commission, 1991 Act 160 The Current Reform Environment • Several Major Parts – Catamount Health • State-subsidized private health insurance for certain eligibles – Blueprint • Reform of the delivery system • Reduction in the incidence of chronic illness Is Catamount Health Working? • Over 5,000 people have signed up for Catamount Health. This is about one-third of the people eligible for it. • Enrollment has also increased in other Medicaid programs, especially VHAP Catamount Health - Issues • Currently, subsidized premiums for Catamount Health range from $60 per month (below 175% of poverty, about $18,000 per year for an individual) to $185 per month (up to 300% of poverty, $31,200 per year) • The unsubsidized product costs $393 per month • Is this affordable? Other States • So far, Maine, Massachusetts, and Vermont are the leaders. • Many other states are attempting various reforms • For details, check out: http://www.kff.org/uninsured/kcmu_statehealthreform.cfm Massachusetts • The most far-reaching state-based reform to date • Key element: an individual mandate, combined with income-based subsidies. – With an out if insurance is not “affordable” • Based on surveys, it seems to be working. Almost 95% of people in Massachusetts are covered, the highest percentage in the country But… • Massachusetts has had minimal impact so far on costs • Unless costs are brought under control, the program will quickly become unaffordable National Health Care Reform? • While the legal barriers are far less daunting at the national level, the political barriers are much higher • Consider what it took in 1965 to enact Medicare and Medicaid • Consider what happened to Clinton health care reform Current Presidential Proposals • Obama – much like Massachusetts, but the mandate applies only to children • McCain – while a more conservative proposal (no mandates, reliance on existing market), it is much more radical in one way – sharp reduction in the importance of employersponsored health insurance; most people will shift to subsidized coverage in individual market Conclusions • Health care reform is essential, and seems to be impossible • Concerns about health care have a 100 year history. How long can we muddle through? • There is a lack of agreement on what reform means, but we seem to be more able to come to agreement on areas other than financing Questions? Steve Kappel Policy Integrity www.policyintegrity.com