Hyperthyroidism (Clinical manifestations)
advertisement
")
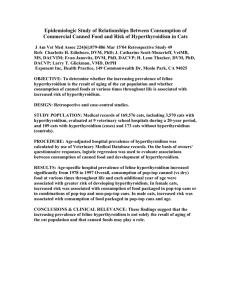
Hyperthyroidism (Clinical manifestations) INTRODUCTION 1. 2. The clinical manifestations of hyperthyroidism are largely independent of its cause. However, disorder that causes hyperthyroidism may have other effects. In particular, Graves' disease, the most common cause of hyperthyroidism, causes unique problems that are not related to high serum TH concentrations. These include Graves' ophthalmopathy and infiltrative dermopathy (localized or pretibial myxedema). Most patients with Graves' hyperthyroidism have diffuse goiter, but so do patients with other, less common causes of hyperthyroidism such as painless thyroiditis and TSH-secreting pituitary tumors. The major clinical manifestations of hyperthyroidism (thyrotoxicosis) will be briefly reviewed here. More detailed discussions of its effects on specific organ systems as well as diagnostic approach to patients with hyperthyroidism are discussed separately. SKIN 1. The skin is warm (and may rarely be erythematous) in hyperthyroidism due to increased blood flow; it is also smooth because of decrease in keratin layer. A. Sweating, which increases due to increased calorigenesis; this is often associated with heat intolerance B. Onycholysis (loosening of nails from nail bed, Plummer's nails) and softening of nails C. Hyperpigmentation, which can occur in severe cases; it appears to be mediated by accelerated cortisol metabolism, leading to increased ACTH secretion D. Pruritus and hives, which are occasional findings, primarily in patients with Graves' 2. hyperthyroidism E. Vitiligo and alopecia areata, which can occur in association with autoimmune disorders F. Thinning of hair Infiltrative dermopathy occurs only in patients with Graves' hyperthyroidism. The most common site is skin overlying shins, where it presents as raised, hyperpigmented, violaceous, orange-peel-textured papules. EYES 1. Stare and lid lag occur in all patients with hyperthyroidism. They are due to sympathetic overactivity, possibly mediated by increased α-adrenergic receptors in some tissues. Lid lag is evaluated by having patient follow examiner's finger as it is moved up and down. The patient 2. 3. has lid lag if sclera can be seen above iris as patient looks downward. As noted above, only patients with Graves' disease have ophthalmopathy. It is characterized by inflammation of extraocular muscles and orbital fat and CNT, which results in proptosis (exophthalmos), impairment of eye-muscle function, and periorbital and conjunctival edema. Ophthalmopathy is more common in patients who smoke cigarettes. Patients with ophthalmopathy may have gritty feeling or pain in their eyes, and may have diplopia due to extraocular muscle dysfunction. Corneal ulceration can occur as result of proptosis and lid retraction, and severe proptosis can cause optic neuropathy and even blindness. CARDIOVASCULAR 1. Patients with hyperthyroidism have increase in CO, due both to increased peripheral oxygen 2. 3. 4. needs and increased cardiac contractility. HR is increased, pulse pressure is widened, and SVR is decreased. Systolic HTN is common. The LVEF does not increase appropriately during exercise, suggesting presence of true CMP. High- or normal-output CHF can occur in patients with severe hyperthyroidism and CHF worsens in patients who already have it. Af occurs in 10 to 20% of patients with hyperthyroidism, and is more common in elderly patients. In study, 8% of all patients and 15% of patients between ages 70 to 79 developed Af within 30 days of diagnosis of hyperthyroidism. Even subclinical hyperthyroidism is associated with increased rate of atrial ectopy and 3-fold increased risk of Af. In 60% of hyperthyroid patients with Af, rhythm converts spontaneously to SR when hyperthyroidism is treated; in one study, all who spontaneously converted did so within 4 months after becoming euthyroid. Among those who do not convert spontaneously to SR and who undergo successful electrical cardioversion, 2-year risk of recurrent Af was 59% compared with 83% of patients whose Af was not associated with hyperthyroidism. The role of anticoagulation is controversial in hyperthyroid patients with Af. In several studies, 10 to 40% of patients with hyperthyroidism and Af had arterial embolus. LAE, which is risk factor for thrombus formation, is present in about 90% of hyperthyroid patients with Af and 2% of hyperthyroid patients with SR. Based on these results, we usually anticoagulate hyperthyroid patients with Af. This recommendation is in agreement with guidelines published in 2006 by ACC/AHA/ESC. 5. Other abnormalities, including MVP, MR, and increase in left ventricular mass index have also been reported. METABOLIC 1. Serum lipids A. Patients with hyperthyroidism tend to have low serum total and HDL-c and low total cholesterol/HDL-c ratio. These values increase after treatment. 2. Hyperglycemia A. Although thyroxine is not counterregulatory hormone, hyperthyroidism can interfere with glucose metabolism. It is associated with both increased sensitivity of pancreatic β cells to glucose, resulting in increased insulin secretion, and antagonism to peripheral 3. action of insulin. The latter effect usually predominates, leading to impaired glucose tolerance in untreated patients. Adrenal function A. Interpretation of cortisol response to ACTH stimulation testing may be misleading in patients with hyperthyroidism because cortisol binding globulin (CBG) levels decrease, resulting in lower total serum cortisol. In one report of 49 hyperthyroid patients undergoing ACTH testing, 35% had subnormal total serum cortisol values (< 18 mcg/dL), while only 11% had subnormal free cortisol index (ratio of serum total cortisol to CBG). RESPIRATORY 1. Dyspnea and DOE may occur for many reasons in hyperthyroidism. 2. Oxygen consumption and CO2 production increase. These changes result in hypoxemia and hypercapnia, respectively, both of which stimulate ventilation. 3. Respiratory muscle weakness is important cause of dyspnea, and reduced exercise capacity may be largely due to respiratory muscle weakness and decreased lung volume. 4. There may be tracheal obstruction from large goiter. 5. Hyperthyroidism may exacerbate underlying asthma. 6. Pulmonary arterial systolic pressure is increased. GASTROINTESTINAL 1. Weight loss is due primarily to increased metabolic rate (hypermetabolism), and secondarily to increased gut motility and associated hyperdefecation and malabsorption; rare patients have steatorrhea. Celiac disease is also more prevalent in patients with Graves' disease. Most patients have hyperphagia, but occasional patient with mild hyperthyroidism may have sufficient appetite stimulation that weight is gained (more commonly in younger patients). Anorexia may be prominent in elderly hyperthyroid patients. 2. Other changes that may occur. A. Vomiting and abdominal pain, rarely B. Dysphagia due to goiter C. Abnormalities in LFT, particularly high serum ALP and, rarely, cholestasis HEMATOLOGIC 1. RBC mass is increased in hyperthyroidism, but plasma volume is increased more, resulting in normochromic, normocytic anemia. Serum ferritin concentrations may be high. 2. Graves' hyperthyroidism may be associated with autoimmune hematologic disorders such as ITP and pernicious anemia, and some patients have anti-neutrophil antibodies. 3. Hyperthyroidism may also be prothrombotic. As example, in meta-analysis of 51 studies evaluating effect of thyroid hormone excess (exogenous or endogenous) on coagulation system, excess thyroid hormone was associated with rise in prothrombotic factors, including factors VIII, IX, fibrinogen, vWF, and PAI-1. Similar findings were noted in patients with either overt or subclinical hyperthyroidism. GENITOURINARY 1. 2. Urinary frequency and nocturia are common in hyperthyroidism, although mechanism is uncertain. Possible causes include primary polydipsia and hypercalciuria. Enuresis is common in children. In women, serum SHBG are high, which results in high serum estradiol and low-normal serum free estradiol, high serum LH, reduced mid-cycle surge in LH secretion, oligomenorrhea, and anovulatory infertility. Amenorrhea can occur in women with severe hyperthyroidism. 3. In men, increase in serum SHBG results in high serum total testosterone, but serum free testosterone are normal or low. Serum LH may be slightly high. Extra-gonadal conversion of testosterone to estradiol is increased, so that serum estradiol is high. These changes can cause gynecomastia, reduced libido, and erectile dysfunction. Spermatogenesis is often decreased or abnormal, eg, more spermatozoa are abnormal or non-motile. BONE 1. Thyroid hormone stimulates bone resorption, resulting in increased porosity of cortical bone and reduced volume of trabecular bone. The loss in cortical bone density is greater than that of trabecular bone. Serum ALP and osteocalcin are high, indicative of increase bone turnover. The increase in bone resorption may lead to increase in serum calcium, thereby inhibiting PTH secretion and conversion of calcidiol to calcitriol. In addition, metabolic clearance rate of calcitriol is increased. These changes result in impaired calcium absorption and increase in urinary calcium excretion. The net effect is osteoporosis and increased fracture risk in patients with chronic hyperthyroidism. 2. Graves' disease may also be associated with thyroid acropathy, with clubbing and periosteal new bone formation in metacarpal bones or phalanges. Patients with thyroid acropathy commonly present with asymptomatic clubbing, severe ophthalmopathy, and dermopathy; a high percentage is cigarette smokers. NEUROPSYCHIATRIC 1. Patients with thyrotoxicosis may experience behavioral and personality changes, such as psychosis, agitation, and depression. Less overt manifestations that are more common in less severe thyrotoxicosis include anxiety, restlessness, irritability, and emotional lability. Insomnia is also common. Symptoms often worsen in patients with preexisting psychiatric disorders. 2. These behavioral manifestations are accompanied by cognitive impairments, particularly impaired concentration, confusion, poor orientation and immediate recall, amnesia, and constructional difficulties. Other neurologic manifestations are discussed separately. GERIATRIC HYPERTHYROIDISM 1. Hyperthyroidism in elderly patients may be apathetic, rather than having hyperactivity, tremor, and other symptoms of sympathetic overactivity. However, two-thirds of such patients have symptoms similar to those in younger patients. In cross-sectional studies of 2. patients with hyperthyroidism, older patients had a reduced risk for the presence of several classical symptoms (heat intolerance, tremor, nervousness) but a higher prevalence of weight loss and shortness of breath compared with younger patients. Older patients also had a higher rate of atrial fibrillation and moderate to severe ophthalmopathy. Elderly patients with Graves' hyperthyroidism are less likely to have a goiter. Toxic multi-nodular goiter is more common in the elderly, although the majority of hyperthyroid patients at any age have Graves' hyperthyroidism. In addition, elderly patients often have persistent constipation. Tachycardia of 100 beats per minute is absent in 40% of elderly hyperthyroid patients, due primarily to coexistent conduction system disease. SUMMARY 1. The classic symptoms of hyperthyroidism include weight loss, heat intolerance, tremor, 2. 3. palpitations, anxiety, increased frequency of bowel movements, and shortness of breath. Goiter is commonly found on physical examination. Elderly patients may have fewer classical manifestations of hyperthyroidism. However, weight loss, shortness of breath, and atrial fibrillation occur more commonly in older than younger patients. The clinical manifestations of hyperthyroidism are largely independent of its cause. However, the disorder that causes hyperthyroidism may have other effects. In particular, Graves' disease causes unique problems that are not related to the high serum thyroid hormone concentrations. These include Graves' ophthalmopathy and infiltrative dermopathy (localized or pretibial myxedema).