PowerPoint
advertisement

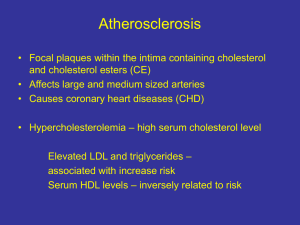
Lipid-Lowering Drugs Kirk Mykytyn, Ph.D. Department of Pharmacology mykytyn.1@osu.edu Learning Objectives Learning Resources 1. Lilly’s Pathophysiology of Heart Disease, 5th ed. Chapter 5 p. 127130 and Chapter 17 p. 431-435 2. Dr. Mehta’s lecture on Lipid Metabolism Introduction: Hyperlipidemia Definition: Elevated levels of circulating lipids, specifically cholesterol and triglycerides (TG) Hyperlipidemia and disease: Hyperlipidemia (and especially high levels of low-density lipoprotein (LDL)) is correlated with an increased incidence of atherosclerosis and coronary artery disease (CAD) Total serum cholesterol level of 240 mg/dl = 2X ↑risk of CAD vs. 200 mg/dl Combination with other risk factors Age/Sex/Family history Smoking Hypertension Diabetes Obesity Low HDL levels Introduction: Hyperlipidemia Treatment of Hyperlipidemia Overview of Lipoprotein Metabolism HMG-CoA Reductase Inhibitors (Statins) Most effective and best-tolerated agents for reducing LDL fluvastatin, lovastatin, pravastatin, simvastatin, atorvastatin, rosuvastatin, and pitavastatin LDL 20-55%, TG 7-30%, HDL 5-15% Other cardioprotective effects Improve endothelial function, promote plaque stability, inhibit platelet aggregation, and suppress inflammation HMG CoA Reductase Inhibitors (statins) Harvey RA. Lippincott’s Illustrated Reviews: Pharmacology. 5th ed. Baltimore, MD: Lippincott, Williams & Wilkins; 2012. HMG-CoA Reductase Inhibitors (Statins) Mechanism of action Analog of HMG CoA Competitive inhibitor of HMG CoA reductase, the rate limiting step in cholesterol synthesis Reduced hepatic cholesterol results in LDL receptor expression, which the removal of LDL from the blood Reduced hepatic cholesterol results in VLDL synthesis and secretion Adverse Effects Hepatotoxicity (less than 1% of patients) Myopathy (2 to 10% of patients) – rarely leads to rhabdomyolysis Contraindicated in pregnancy Niacin Niacin (nicotinic acid, vitamin B3) is one of the oldest lipid-regulating drugs and favorably affects virtually all lipid parameters Most effective agent for raising HDL cholesterol LDL 5-25%, TG 20-50%, HDL 15-35% Overview of Lipoprotein Metabolism Niacin Niacin Niacin Mechanism of action Decreases hormone-sensitive lipase (HSL) activity in adipose tissue flux of free fatty acid to the liver, hepatic TG production, VLDL secretion Enhances lipoprotein lipase (LPL) in adipose and muscle cells TG clearance from circulating VLDL Increases the half-life of apoAI, the major apolipoprotein in HDL HDL levels, without disturbing hepatic retrieval of cholesterol Adverse Effects Transient cutaneous flushing and itching Prevented by aspirin, regular use, or timed-release formulations Hyperuricemia, impaired insulin sensitivity, hepatotoxicity, and myopathy Fibrates Fibric acid derivatives (gemfibrozil and fenofibrate) Primarily used for reducing TG and increasing HDL serum levels LDL 0-20%, TG 20-50%, HDL 10-20% Overview of Lipoprotein Metabolism Fibrates Fibrates Mechanism of action Activators of the nuclear transcription factor peroxisome proliferatoractivated receptor α (PPARα) LPL expression, TG clearance from circulating VLDL expression apoAI, HDL levels Adverse Effects Mild GI disturbances Gallstones ( biliary cholesterol excretion) Myalgia Bile Acid-Binding Resins Large, highly positively charged molecules that bind negatively charged bile acids and bile salts in the small intestines LDL 15-30%, TG, HDL 3-5% Mechanism of action Bile acids are prevented from returning to the liver and are excreted in feces hepatic cholesterol conversion to bile acids, hepatic cholesterol concentrations, LDL receptor expression Hepatic cholesterol synthesis also stimulated VLDL production, serum TG levels Adverse Effects Interference with absorption of fat-soluble vitamins and certain drugs GI effects: constipation, nausea, and bloating Cholesterol Absorption Inhibitors Treatment Guidelines for Hyperlipidemia Harvey RA. Lippincott’s Illustrated Reviews: Pharmacology. 5th ed. Baltimore, MD: Lippincott, Williams & Wilkins; 2012. Emerging Therapeutics Proprotein convertase subtilisin/kexin type 9 (PCSK9) routes LDL and LDL receptor complexes for degradation in lysosomes Monoclonal antibodies against PCSK9 block the interaction of PCSK9 with the LDL receptor, allowing LDL receptor recycling to the cell surface, which leads to a decrease in circulating LDL Thank you for completing this module Questions? mykytyn.1@osu.edu