Body-Weight- Supported Gait Training
advertisement

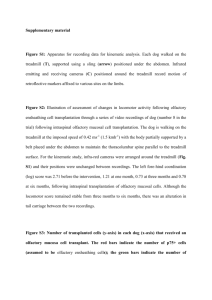
Body-WeightSupported Gait Training Mary Bernardo, Katie Blow, Lauren Bussian, Kaylea Kirven, Sarah Nockengost Alternative Intervention Presentation Lifespan 1 2015 Virginia Commonwealth University Body-Weight-Supported Treadmill Training (BWSTT) ● Used in a variety of practice settings ● Targets strength, endurance, and task-specific gait training ● Body weight is unloaded by a harness or adult assistance ● Active movements with therapist guidance/assistance when necessary ● Generally followed by a period of overground gait training with body-weight support as needed Body-Weight Supported Treadmill Training, Colorado Physical Therapy Specialists Video https://www.youtube.com/watch?v=XLdc tmNvACo Background ● 1960’s - Animal research proved that cats with transected spinal cords could actively step after a period of BWSTT ● 1992 – Wernig and Muller reported improved walking patterns following BWSTT in patients with SCI ● Systematic Review of pediatric studies in 2006 Only 7 articles from peer-reviewed sources ● Still preliminary in pediatric population Rationale • Motor Learning principles support the use of repetitive, task-specific practice over time • Current evidence demonstrates the neuroplasticity of the central nervous system, indicating its ability to learn • Body-Weight-Supported Gait Training provides the appropriate intensity and specificity needed to promote neuroplastic changes. • Facilitates step training • Reduces postural requirements • Encourages more appropriate motor patterns APTA Guidelines for Use of Body-WeightSupported Treadmill Training (APTA’s Section on Pediatrics, 2010) Frequency 2-5 days/week Session Length 5-30 minutes/session Treadmill Speed .05-3 mph Percent Body-Weight Support Load stance limb Use the least amount of body-weight support to maintain erect postural alignment Manual Assistance Least amount required for stepping Assist intra- and inter-limb coordination if necessary Support Using arms/hands Fading use of handrails Episode of Treatment 2-16 weeks Equipment • Various equipment used for BWSTT Examples: • LiteGait System: • May require manual assistance requiring 2-4 trained providers • Lokomat: • Provides robotic assistance during body-weightsupported gait training • Therapist Support LiteGait® Lokomat® Continuing Education/Training • Certification and continuing education are not required to utilize BWSTT in physical therapy intervention • Many companies offer training for use of their products •LiteGait ($850-$140) •Lokomat Patient Population • Down Syndrome • Cerebral Palsy (CP) • Spinal Cord Injury (SCI) • Myelomeningocele • Stroke • Guillain-Barre Syndrome • Traumatic Brain Injury (TBI) Contraindications • • • • • • • • • Cardiovascular issues Osteoporosis Fractured ribs Groin infection or skin graft in groin area Weight-bearing restrictions Ventilator dependency Intravenous drip Self-harming behavior **Any contraindication to exercise (Ex: orthostatic hypotension, thrombocytopenia) A Systematic Review of the Effectiveness of Treadmill Training and Body Weight Support in Pediatric Rehabilitation Damaino, D. et. al. (2009) Journal of Neurological Physical Therapy Purpose: To explore the strength, quality, and conclusiveness of the scientific evidence supporting BWSTT in children with motor disabilities. Design: 29 articles met inclusion criteria. Results for CP: - Highest level study: significant increase in self-selected gait speed and walking distance - High variability across subjects in the amount of change - Positive effects are small and mostly non-significant - No harmful outcomes Conclusion: Limited evidence that has non-significant outcomes; has not been compared sufficiently to other interventions A Systematic Review of the Effectiveness of Treadmill Training and Body Weight Support in Pediatric Rehabilitation Damaino, D. et. al. (2009) Journal of Neurological Physical Therapy Results for Down Syndrome: • Highest level study: practicing step training on a motor treadmill can accelerate development of ambulation • More intense protocol is preferred over lower intensity levels - Long term effect on physical activity levels - Greater stride length - Earlier age of walking onset Conclusion: Body-weight-supported treadmill training is effective for promoting the development of independent ambulation and enhancing gait qualities. A Systematic Review of the Effectiveness of Treadmill Training and Body Weight Support in Pediatric Rehabilitation Damaino, D. et. al. (2009) Journal of Neurological Physical Therapy Results for SCI: - Mostly positive outcomes with clinically significant changes. - Many children became functional ambulators. - Lack of change in lower extremity motor strength indicates task-specificity of practice. - Data is limited in children compared to adults. - No negative or harmful effects were found. Conclusion: Limited evidence warrants more rigorous studies in this patient population Treadmill Training of Infants With Down Syndrome: Evidence-Based Developmental Outcomes Dale A. Ulrich, PhD, Beverly D. Ulrich, PhD, Rosa M. Angulo-Kinzler, PhD, Joonkoo Yun, PhD Purpose: To determine if practice stepping on a motorized treadmill could help reduce the delay in walking onset normally experienced in infants with Down Syndrome. Design: n = 30; began study once able to sit independently for 30 sec. Control Group Experimental Group Biweekly PT HEP Adult assist treadmill stepping practice 8 minutes/day, 5 days/week Speed .46mph Biweekly home PT and research staff visits HEP Treadmill Training of Infants With Down Syndrome: Evidence-Based Developmental Outcomes Dale A. Ulrich, PhD, Beverly D. Ulrich, PhD, Rosa M. Angulo-Kinzler, PhD, Joonkoo Yun, PhD Results: Length of time (days) from entry of study to onset of: Control Group Experimental Group Mean Difference Raise to Stand 194 134 60 Walking with Help 240 166 73 Walking Independently 401 300 101 Conclusion: Body-Weight-Supported Treadmill Training is an effective approach in early intervention to facilitate earlier onset of independent walking. Efficacy of Partial Body-Weight-Supported Treadmill Training [PBWSTT] Compared With Overground Walking Practice for Children With Cerebral Palsy Willoughby, et al. (2010) Disabil. Rehabil. Purpose: • Determine safety and feasibility of PBWSTT in a school environment • Investigate if PBWSTT can increase walking endurance, walking speed, and walking function at school for children – adolescents with CP (GMFCS III & IV) Design: • Inclusion Criteria: • Exclusion Criteria: • Ages 5 – 18 years old • Physical assistance to walk • Diagnosis of CP • Concurrent medical condition • GMFCS Level III or IV • • Able to understand simple instructions Lower limb orthopedic surgery or botulinum toxin injection within 6 months of study Willoughby, et al. (2010) n = 26 Outcome Measures: Baseline, Week 10, 14 weeks after training - 10-meter Walk Test - School Function Assessment - 10-minute Walk Test Willoughby, et al. (2010) Results: Conclusion: –PBWSTT is safe & feasible to conduct in a school setting for children with CP –But, BWSTT is no more effective than practicing overground walking Limitations: –Q of L, psychological outcomes, physiological outcomes not measured –Severity of CP Locomotor Training Within an Inpatient Rehabilitation Program After Pediatric Incomplete Spinal Cord Injury: A Case Study Prosser, L. (2007) Phys. Ther. Purpose: Describe a comprehensive inpatient rehabilitation program with a locomotor training component in a child with a severe incomplete SCI. Patient: 5 y/o female with C4 level lesion Intervention: Inpatient rehabilitation program including a component of BWSTT and overground gait training; 3-4x/week for 6 months Outcome Measures: ASIA Impairment scale, WeeFIM II, Walking Index for Spinal Cord Injury II, Parent-report Results: • Walking independently with rolling walker and L AFO (30-100m) • Clinically significant improvements in UE and LE motor scores • Clinically significant improvements in WeeFIM II and WISCI II scores • Participation - walking in school 100% of the time ICF ICF ICF Recommendations ● Safe! ● Positive results in certain pediatric populations ● Financial burden ● Time-intensive ○ When do we stop working on gait and focus on other skills? ● Need more RCTs and studies comparing BWSTT to other gait training methods References: • • • • • • • • • • Body-Weight-Supported Treadmill Training: Using Evidence to Guide Physical Therapy Intervention. Section on Pediatrics, American Physical Therapy Association. 2010. Body-Weight Supported Treadmill Training. University of Washington Rehabilitation Medicine, 2003. Web. <http://sci.washington.edu/info/newsletters/articles/03sp_body_weight_support.asp>. Behrman AL, Harkema SJ. Locomotor Training after Human Spinal Cord Injury: A Series of Case Studies. Physical Therapy. 2000;80(7):688-700. Litegait Training. https://www.litegait.com/education/litegait-training Rehabilitation Institute of Chicago. Pediatric Lokomat Walking Therapy. http://www.ric.org/conditions/pediatric/services/pediatric-lokomat-walking-therapy/ Duncan, PW, et. al. Body-Weight-Supported Treadmill Training Rehabilitation after Stroke. N Engl J Med. 2011. 364 (21). Damiano DL, DeJong, SL. A Systematic Review of the Effectiveness of Treadmill Training and Body Weird Support in Pediatric Rehabilitation. J Neurological Phys. Ther. 2009; 33: 27-44. Ulrich DA, Ulrich BD, Angulo-Kinzler RM, Yun J. Treadmill training of infants with Down syndrome: evidence-based developmental outcomes. Pediatrics 2001;108 Willoughby, KL, et. al. Efficacy of partial body-weight supported treadmill training compared with overground walking practice for children with cerebral palsy: a randomized controlled trial. Archives Phys. Med. Rehabil. 2010. (3) 333-9. Prosser L. Locomotor Training Within an Inpatient Rehabilitation Program After Pediatric Incomplete Spinal Cord Injury. Phys. Ther. 2007; 87: 1124-1232. Questions?