Navigating Your Way Through Two MOCs
advertisement

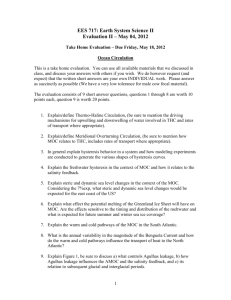
Maintenance of Certification: Navigating Your Way Through Two MOCs H2089 Section on Med-Peds Program J. Thomas Cross, Jr., MD, MPH, FAAP, FACP President, A-Cross Medicine Reviews Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity. I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation. But For FULL Disclosure • From January 7, 2002 to January 6, 2013, I worked for MedStudy Corporation. • I have a non-compete with MedStudy until January 7, 2016. • I currently own and teach for a Primary Care CME company—that does not do ANY Board Review Preparations—just fun CME courses.* • I supplement my income by doing Home Health assessments. *This was true as of 8/19/15…In January 2016, ABIM will allow routine approved CME to count for Part 2! • If you plan on starting your own company from scratch, plan on eating Raman noodles and having to drink box wine or really, really cheap gin/bourbon during the first 3 years. Changes You May Wish to Make in Practice 1. Find an easier way to navigate MOC 2. Understand the whole process of reciprocity and whether it helps you or not 3. Demonstrate to you which “Parts” are quick and easy if you are in a time crunch Preparation • I meticulously went through the ABIM and ABP websites • I followed the total public decimation of the ABIM (Newsweek to blogs) • The ABP Response to ABIM temporarily getting rid of “Part 4” Preparation • I surveyed the Med-Peds listserve • Allen Friedland supplied documents from the APDIM and APPD meetings from the ABIM and ABP • I used my 18+ year knowledge of teaching at various Board reviews and knowing what people have told me personally about how they survived/navigated the ABIM and ABP Comments from Your Peers “I approached the whole process with the view that it was a stupid useless burdensome exercise and looked for the easiest way to complete the requirements with no expectation I would learn anything from the process. I went to the online Part 2 offerings on the board sites and selected ones that were free and which I might have a chance of passing without further study (e.g. General Medicine update). I took the tests without reading anything, kept track of the answers, usually failed on the first try, but with a retake or two I passed the test and got the credit with very little investment of time. Part 4 I did by looking around on the website for a free easy program and found the Joslin Cardiovascular exercise. I quickly reviewed some charts, waited a few months and reviewed some more charts and I was done. It also was relatively painless. Both boards credited me for this.” Part 4 is now easier as my hospital's diabetes performance improvement program now counts and I work in a PCMH* which also counts. *An NCQA (National Committee for Quality Assurance) designated Primary Care Medical Home (PCMH). “I'm totally overwhelmed and confused by the process” “I tried to start one of the AAP practice improvement modules - I thought that hypertension would be easy - but I don't have enough clinical volume to be able to complete this in a reasonable timeframe. It's going to take me two years of one half day clinic per week (in a resident clinic that sees mostly kids <3) to complete 2 initial and followup cycles with 25 charts at a time.” “I have honestly not found any straightforward or useful MOC 4 activities. I think the modules through AAP Equipp are the easiest to get through, especially now that there is no extra cost on top of AAP membership. Having said that, I cannot say these activities have changed my clinical practice. I learned a lot more when mentoring a few QI projects with residents, but at the time it was too cumbersome to have those projects accepted to meet my MOC 4 requirements. I completed one MOC 4 module through the ABP on influenza vaccine. I had to give surveys to participating patients to complete which I found really disrupted the flow of the visits and would not recommend those. I prefer to go back and do a chart review on my own terms.” “My academic appointment is primarily IM, so I was planning on using reciprocity for Peds and doing my points in IM (with some medical knowledge points in Peds, too, just to keep up my skills). However, my first Peds cycle ends in December 2016, and I don't have to earn any substantial IM points until December 2018. My IM points don't even count until January 2016! My initial certification for both was in the same year. I'm also leery of counting on ABIM part 4 points when they're "suspended." I have just 4 hours/week of Peds clinical activity (precepting residents) so getting part 4 points on Peds is going to be really hard, but I'm afraid of putting off part 4 until I only have a few months to go... it's a dilemma.” Editorial note from Tommy: (I would disagree and say this….) Cost of Recertification • Internists will incur an average of $23,607 (95% CI, $5,380 to $66,383) in MOC costs over 10 years, ranging from $16,725 for general internists to $40,495 for hematologists-oncologists. Time costs account for 90% of MOC costs. • Cumulatively, 2015 MOC will cost $5.7 billion over 10 years, $1.2 billion more than 2013 MOC. This includes $5.1 billion in time costs (resulting from 32.7 million physician-hours spent on MOC) and $561 million in testing costs. Ann Intern Med. Published online 28 July 2015 doi:10.7326/M15-1011 ABIM unlinks MOC enrollment from board certification (Dr. Baron BLOG post—August 4, 2015) • Diplomates who lost certification solely on the basis of failure to enroll in MOC or to pay MOC fees have now had their certification status updated to “certified.” ABIM Requirements (8/2015) ABIM Changes January 2016 • Maintaining Cardiovascular Disease certification will no longer be required to maintain certification in Advanced Heart Failure & Transplant Cardiology, Clinical Cardiac Electrophysiology, Interventional Cardiology and Adult Congenital Heart Disease • Maintaining Gastroenterology certification will no longer be required to maintain certification in Transplant Hepatology • Maintaining another certification will no longer be required to maintain certification in Adolescent Medicine, Hospice & Palliative Medicine, Sleep Medicine and Sports Medicine ABIM Requirements 8/2015 • The MOC program requires that you complete some MOC activity every 2 years and earn 100 points every five years (at least 20 in Medical Knowledge). • Points earned every 2 years will also count toward your fiveyear requirement, and also count toward the milestones for the certifications you are maintaining. Points earned count toward all certifications being maintained. • If you are in fellowship, you can earn 20 MOC points for each eligible year of fellowship training (10 in medical knowledge, 10 in practice assessment) • If you are dual-boarded by one or more of the other American Board of Medical Specialties (ABMS) member Boards, your selfevaluation requirements will be waived—if you fill out reciprocity. ABIM Requirements Continued • Pass the MOC exam in your specialty(ies) every 10 years (first exam attempt in each certification area you maintain earns 20 MOC points). • Part 4 is currently not required: • Practice Assessment • Patient Voice • Patient Safety ABIM Requirements for Reciprocity • To receive credit, ABIM diplomates will need to attest that they are current and participating in the other Board's MOC program. Diplomates will still need to meet the other ABIM MOC requirements: • • • maintain a valid, unrestricted and unchallenged medical license pass a secure ABIM MOC examination meet any ABIM-specific, subspecialty-specific procedural requirements • About attesting: • If you are eligible to participate, you will see a link on your home page. The link takes you to the attestation form. • Upon attesting, self-evaluation credit is applied to your ABIM MOC Status Report. ABIM Requirements for Reciprocity • ABIM will randomly audit attestations. Providing false or misleading information could result in disciplinary action by ABIM, including certificate revocation and reporting of misrepresentation to state medical licensing boards. • You will be required to complete a new attestation form every 2 years in order to continue to receive ABIM MOC credit. When due, a link will appear on your personal ABIM home page and a reminder email will be sent to your e-mail address. ABIM “Free” General IM Part 2 Note. That there are only 74 Part 2 points available for “Free” from the ABIM. Remember, you have to have 100 points total over 5 years. Hmm….. So either do “non free” part 2’s or free part 4’s or specialty free part 2’s to reach 100 points. ABIM “Free” General IM Part 2 Note. That there are only 74 Part 2 points available for “Free” from the ABIM. Remember, you have to have 100 points total over 5 years. Hmm….. So either do “non free” part 2’s or free part 4’s or specialty free part 2’s to reach 100 points. ABIM Part 2 “Free” • Easy to do quickly if you don’t care about “failing” initially • For example, run through 2013 ABIM Update in Internal Medicine • Answer questions off the top of your head • If you pass, great; if you fail, they tell you which ones you missed. Go back and answer those— repeat process till you pass • If you are an ACP member—the link takes you directly to the answer—Yes, it is just that easy. ABIM “Non-Free” • MKSAP • MOC Modules online from ACP Meeting last/this year—gives you 30 points—but you have had to pay registration for the meeting for it to be “Free” • NEJM • SGIM • Many other organizations IM Certification Examination: First Taker Pass Rates Categorical IM vs Medicine-Pediatrics 100% 88 83 80% 84 85 77 84 86 83 87 86 60% IM IM/Peds 40% 20% 0% 2010 2011 2012 2013 2014 Most Commonly Used MOC Modules Med-Peds 2010-2014 ABIM Part 4 (PIMs) • Tons of choices • Easy chart reviews to patient surveys • Osteoporosis noted by many • Many do their own QI projects (PIMs) and turn them in • Only requires 25 patients at baseline and 1 repeat measurement after “intervention” • Those in teaching do Clinical Supervision PIM ABP Requirements • Every 5 years must have 100 points • Part 2: 40 points • Part 4: 40 points • Part 2 or 4: 20 points • Part 3 test every 10 years • May change in 2017 with MOCA – Maintenance of Certification Assessment!! Exciting News for Peds and Med-Peds Residents! • All residents will be enrolled in November of your PL1 year!! • You have to complete 100 points within your first 5 years after graduation. Congrats! Welcome to our nightmare. • Do Part 4 now in residency and “bank it” (have your preceptor do the Motivation Interviewing PIM—it gives you and THEM credit). • Those going into Fellowship get 10 points of part 2 and part 4 each year just for being in Fellowship More Resident ABP MOC info • Residents can now earn Part 4 MOC credit during residency for meaningful participation in QI activities (just like a diplomate) • • • PIMs (like the motivational interviewing PIM) Approved QI projects in institutions and organizations Authorship of qualifying QI articles or posters/platform presentations • Resident MOC credit will be “in the bank” for when they become certified. It will then be applied to their first MOC cycle. • Residents can access other ABP Part 2 activities (e.g. self assessments), but will not receive bankable credit for any Part 2 activities. ABP Part 2 (“FREE”) • General Knowledge • 200 questions, BUT you only get 10 points • Save this till before your exam because it is VERY similar to the testing center test—a good way to tell if you are ready • One example: Asthma—30 questions for 20 points • Simple if you manage asthma • Just use the provided reference (300+ pages!) to answer all the questions • (took me less than an hour—hint…the reference is a PDF— just do a keyword search based on the question; for example question on increased risk of asthma from “infant exposures”) ABP Part 2 “Free” • Unlike ABIM, you only get 1 chance to get it right • For example, on the asthma part 2, I had to get 80% correct for it to “count”. • Makes you nervous early on, and you generally find yourself being overcautious and looking up stupid things you know. It tells you as you answer if you are right/wrong. Question of the Week • “Approximately 20 minutes will be required to read the case study, abstract and commentary and answer the question presented in this assessment. You must attest that you have read the materials by committing your response. If your final response is incorrect, you will not have another opportunity to answer the question. You are not required to complete the assessment in one sitting, and may save and complete it later.” • 25 questions correct = 10 MOC points • (No limit in 5 years—so you could do 250 questions in 5 years for 100 points if you answered everything correctly) Part 2 “Not Free” • PREP • Generally recommended because it has “similar questions” to ABP testing center exam • Multiple Sources—generally all cost money (Q&A series, etc. or specialty society membership) ABP Part 4 “Free” • All require baseline + 2 post intervention processes and various intervals • Minimum time to complete: 2 weeks (Handwashing and Reducing errors in prescriptions!); most minimum 6-8 weeks; a few 4 weeks ABP Part 4 “Free” All Ages including adults! • • • • Handwashing Health Literacy Influenza Motivational interviewing • Patient Centered Medication Management • Reducing errors in prescriptions ABP Part 4 “Age Specific” • Adolescent Depression screening • Chlamydia (adolescent females) • Critical congenital heart disease (newborns) • Developmental survey (9 months and 24 months) • Enhancing breast milk use in nursery • Obesity (2-18 years) • Preschool vision screening (3-5 years) Part 4 “Free” Patients/cycle • 10: ADHD, Breast feeding in nursery, adolescent depression screening, improving asthma care • 15: Reducing errors in prescriptions • 20: Chlamydia, Developmental, Influenza, obesity, patient centered medication, preschool vision • 30: Handwashing • 40: Critical CHD Part 4: Forms • Only 1 form (no patient or staff): • Critical CHD (newborns only) • Patient centered medication management • Only 1 form (just to patient) • Handwashing • All the rest are usually 2 forms (commonly patient/parent and physician) Part 4 “Not Free” • AAP has lots of resources including EQUIPP! Part 3—MOCA? • MOCA is based on the American Board of Anesthesiology (ABA), which coined the term “MOC Anesthesiology (MOCA) Minute” to describe their assessment tool. MOCA • Last year, 1,400 ABA diplomates participated in the initial MOCA Minute pilot. • 1 multiple choice question via email every week. • They could choose when to open the question, but once it was opened, they had 1 minute or other time period depending on complexity to answer. • Immediately after submitting the answer, a feedback page appeared indicating whether the answer was correct, as well as a brief explanation of the correct answer, the learning objective, key references, a comment box, and links to learning resources provided by the various anesthesiology specialty societies. • If the diplomate answered the question incorrectly, some follow-up questions on the same general topic continued to appear in subsequent weeks or months. More on MOCA • The Anesthesia Board announced that it will replace its current every 10-year Part 3 MOC exam in general anesthesiology with an expanded MOCA Minute pilot as part of their redesigned MOCA program (i.e., MOCA 2.0). • Their diplomates will be required to answer 30 questions per quarter (120 questions per year). MOCA 2.0 will be “summative,” meaning that a pass/fail decision is made based on the diplomate’s answer pattern over time. Those approaching the minimum standard will receive an alert and have the opportunity to improve their performance. ABP “MOCA” • The ABP is planning to conduct its own pilot study and will be developing a version of MOCA to be launched no later than January 2017. • Diplomates will establish a practice profile when registering for MOCA, so that the content can be weighted to suit the type of practice. • Diplomates may receive 1-3 multiple choice questions per week. ABP “MOCA” • Online resources or books may be used, but because each question is timed, you’ll need to judge carefully whether to invest time in searching through a resource. • A feedback page will pop up after submitting the answer. • If MOCA is ultimately adopted, the ABP will make pass/fail decisions based on the response patterns. Those who successfully participate will meet standards for Part 3 of Maintenance of Certification. ABP Reciprocity Credit with ABIM • If you are ABP certified seeking reciprocal credit for participation in MOC ABIM, you must satisfy the following eligibility criteria: • You are a diplomate of the ABIM. • You are currently meeting MOC requirements with ABIM. • You have earned at least 20 Part 4 MOC points with ABIM within the last 5 years. • You have/will continue to complete the required Parts 2 & 4 activities with ABIM. • You are certified and according to your ABP Portfolio your MOC cycle ends this year OR you are trying to regain your certification/the designation of meeting MOC requirements. MOC Enrollment exempts you from CME requirements for these State Licenses • • • • • Idaho Minnesota North Carolina Oregon West Virginia • California!—Once you take the exam at testing center and pass you get 100 hours credit for 4 consecutive years! September 2015 ABIM Bombshell • Assessment 2020 Task Force Findings to Focus Discussion of Changes to ABIM Certification and Maintenance of Certification • 150 page pdf • (http://transforming.abim.org/assessment-2020-task-force-findings-to-focus-discussion-of-changes-to-abim-certificationand-maintenance-of-certification/ • Bottom Line: Part 3 (the testing center test) to go away for ABIM as well! Members of the Task Force • • • • • • • • • • Harlan Krumholz (Chair) Yale University Richard Baron American Board of Internal Medicine Lee Berkowitz University of North Carolina (Chapel Hill) Jack Boulet Educational Commission for Foreign Medical Graduates David Coleman Boston University Ezekiel Emanuel University of Pennsylvania Kevin Eva University of British Columbia Ted Eytan Kaiser Permanente David Johnson University of Texas Southwestern (Dallas) Rebecca Lipner American Board of Internal Medicine • • • • • • • • • Marilyn Mann Patient Advocate William McGaghie Loyola University Chicago André A. Rupp Educational Testing Service Martín J Sepulveda IBM Corporation Candace Thille Stanford University Graduate School of Education Abraham Verghese Stanford University School of Medicine Robert Wachter University of California San Francisco Patrick Alguire (Ex-officio) American College of Physicians Steven Durning (Ex-officio) Uniformed Services University Subtle Difference Between IM and Peds “I just finished a set of PREP questions that were still relevant to what I do (resident education), even though some of them seemed to be less relevant (like the one about teaching testicular self-exam. Really?).” IM versus Peds • IM Testing Center Test • HARD (similar to initial cert)! (as of 10/2015) • Evidence-based • Peds Testing Center Test • Easy compared to initial exam • Not-evidence based—AAP based • Example: Testicular cancer screening recommended by AAP but not by USPSTF Options • Do IM and Peds separately • Still make sure you get the IM 30% discount! • Do IM and get reciprocity with Peds • Do Peds and get reciprocity with IM Do all IM and get Peds Reciprocity • Pros: • Most people need to study for the IM test • If you use MKSAP you get CME and Part 2 credit all at the same time to prepare you for Part 3 • For Peds reciprocity, you only need 20 points in IM Part 4 (which most people find the most painful) but, this has to be within 5 years (so, you have to do a part 4 every 5 years no matter which reciprocity you pick, but doing Peds requires 40 points every 5 years) • Part 2 IM can be done in a weekend • Cons: • Every 2 years you need 20 new points Do all Peds and get IM reciprocity • Pros: • Peds Part 4 are generally easy to do or do EQUIPP if AAP member • Only have to complete it every 5 years (no every 2 year requirement of doing “something”) • Cons: • Less easy to get Peds Part 2 points for free • IM test requires more study so end up spending time and money on part 2 products for IM anyway Bottom Line • Most of us do various Part 2 preparations in each IM and Peds • Part 4 is the sticky point to figure out • Unless you have lots of Part 4 opportunities: QI projects, Medical Home designation, etc….then for you, it is easier to get Part 4! Bottom Line for Me • Is Part 4 “Easy” or “Hard” for you • Easy? Take your pick of whether you’d like to do 40-60 points of Part 2 (to reach total of 100 points) every 5 years (Peds) or 40-80 points of Part 2 every 5 years at 20 points a pop q 2 years (IM) • Hard? Pick IM, otherwise you have to do a Part 4 for 40 points every 5 years instead of 20 points If you are a resident… • Bank as many part 4 points as you can (up to 60 points) for Peds. • Then when enrolled in MOC, I’d do Peds and get IM reciprocity. You only need 40 points in Part 2 Peds by the end of 5 years and the reciprocity in Peds lasts you 10 years in IM. • Then, reevaluate in 9 years (when IM is due) based on your ability to get Part 4 (remember you can do nothing in Peds from years 6-9 and “still meet requirements”, while IM requires something done every 2 years). References • http://www.abim.org • https://www.abp.org • Ann Intern Med. Published online 28 July 2015 doi:10.7326/M151011 • http://www.newsweek.com/certifiedmedical-controversy-320495