Pediatric Transport Medicine
advertisement

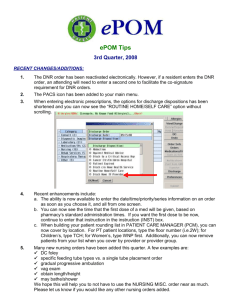
Pediatric Transport Anjali Subbaswamy, MD Critical Care Medicine Children’s National Medical Center Pediatric Transport Medicine (MD’s perspective) • • • • Overview People Process Medical Care Who and why • Why – diagnostic or therapeutic - MD discomfort - parental request • Who – any age, any illness - must be stable enough Utility vs Futility • The benefits of transport must outweigh the risks for the patient limited space, equipment, staff separation from family • The risks/costs of transport must be justified History • • • • • First AAP guidelines 1986 Goal – to provide a safe envt btw H’s Most peds is interfacility (US) <10% of ambulance calls are pediatric <3% of paramedics see >15 kids/mth Lack of pediatric expertise Average EMS provider sees: • 1 peds BVM case q 1.7 years • 1 peds intubation q 3.3 years • 1 peds IO line q 6.7 years Federal EMS-C program (1984) funds educational efforts by states Turn around time • Emergent – trauma - where to? • Urgent – DKA - ASAP – depends on logistics • Routine – for subspecialty care • - 24-72 hours Reimbursement • Patient’s insurance • Taxes • Out of pocket Pediatric vs Adult • • • • Different pathologies More equipment (sizes) +/- parent Early goal-directed rx vs Scoop ‘n run The players Sending Receiving • • • • • • • • • Person who calls 911 Referring hospital MD Referring hospital RN Pt’s legal guardian State police Local EMS Pediatric transport svc Referral hospital ER Accepting physician Med Control Physician • • • • • PEDS ER OR PICU Accepts pt, consults subs Sends appropriate team Directs stabilization Provides ongoing direction to transport team Accepting MD responsibilities • Legally – when transport team arrives on scene can be tricky (ex) Insulin not started for DKA pt • Ethically – when you accept the pt on the phone TEAM Composition ALS team (10%) • MCP • Paramedic • EMT Critical CareTeam (90%) • • • • MCP RN +/- RT +/- MD Paramedic EMT Case 1 – 7 yo MVA ~1 hr The process • • • • OSH/EMS calls referral center Accepting physician (aMD) identified MCP directs transport team Pt arrives to ED or on unit • aMD provides feedback to OSH + PMD Vehicle selection • Ground – space and option to stop • Fixed Wing – stability in bad weather • Helicopter – land at scene, speed Referring hospital responsibilities • • • • • • • • Call appropriate referral center +/- transport svc Copy patients chart Obtain written consent from parents Document acceptance by referral MD Stabilize lines, tubes, splints MD gives report to transport team RN gives report to receiving RN Provide parent w/written destination Case 2 Pneumonia • • • • 2 yo at OSH inpt for 3 days Nec Pna, Abx – resp distress Called for PICU admission 3 hr turnaround time Correct dx? Correct representation of resp distress? WRAMC contracts with CNMC • CNMC 5000 per year • 20% neonatal 80% pediatric • WRAMC and affiliates - 261 last year Case 3 • • • • 4 yo w/CNS tumor Obstructive HC, VPS, Sz d/o Make-a-wish trip to Disneyworld … Status epilepticus transferred for social reasons (home) MEDICAL CARE • Equipment • Medications • Monitoring Specialized meds • Come with patient (factor in travel time/delays) • Pre-ordered at recv’g site if poss. • chemotx, off-label meds, timed abx, metabolic cocktails, all gtts Monitoring Medtronic Lifepak 12 • • • • • • • Monitor/defibrillator 12 lead ECG NIBP Capnography 2 invasive lines Vital sign trends Bluetooth wireless • POC testing Case 4 • • • • • 2 yo s/p Fontan admitted to WRAMC for pna Required Bronch, VATS, intubation ASA 4 intubation risk L MS bronchus compression Predicted LOS 5-7 days Elective transfer to CNMC Conclusion • People • Process • Medical Care