File - Adam james trafas
advertisement

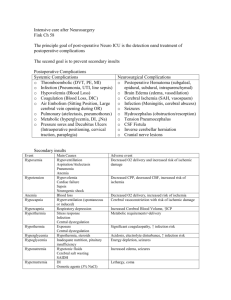
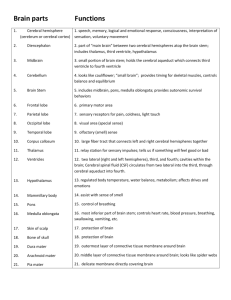
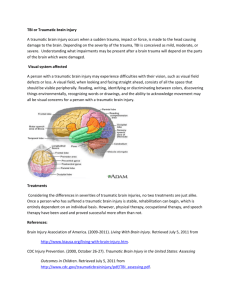
Nursing Intervention Synthesis/Patient Summary Events leading to admission (ER, Direct Admit, Transfer from another facility) This client, K.R., is a 15-year-old, well-developed Caucasian male. On Sunday, March 16th, 2013, this young man was riding to church with his mother and two brothers. There were headed down a two-way 55-mph country road when the mother hit a patch of black ice and slid into a head on collision with another vehicle. K.R. was seated in the back seat, likely was ejected from the vehicle during the collision. The remaining 3 passengers all remained within the vehicle. The driver of the other vehicle rushed over to K.R., who was lying in the road 50 feet from the vehicle unresponsive and bleeding profusely from his head. Per EMS reports that CPR was performed and the patient was intubated and transported to St. Mary’s via helicopter. The remaining three passengers were all admitted to hospitals for varying injuries include one brother to St. Mary’s, the mother to Covenant Health Care, and the other brother to Mid Michigan Regional Medical Center. Presenting Symptoms per ED documentation: The patient arrived at St. Mary’s unresponsive and with full spinal precautions. At1032. On admission he was quite hypothermic and was shivering. He also presented with a large laceration in the right parietal occipital are which was stapled quickly and after being hemodynamically stabilized he was taken back to the CT scan for a full body scan (See Laboratory/ Test Results). The following information was obtained from K.R’s medical record prior to my arrival. Physical Assessment per ED documentation: This is the initial physical assessment completed in the emergency department prior to surgery submitted at 1324 on the day of the accident. Information Presented here is verbatim from a physical assessment document done by emergency department personnel. See “Physical Assessment” for a full in depth assessment completed the following morning. Craniofacial: The client had approximately 8 centimeters laceration to the right parietal occipital area of the scalp in which staples were applied. Neck: The client has a C-collar in place that was applied at the scene. Eyes: Pupils are 3 mm, equal, round, and sluggishly reactive to light. ENT: The client does have an ET tub in place. Mucous membranes are pink, moist, and normal in color. External ears are intact. Tympanic membranes are intact. Respiratory: Equal breath sounds. Cardiovascular: Regular rate and rhythm. No pericardial friction rubs. Abdomen: Soft, non-tender, non-distended with active bowel sounds. No peritoneal signs. No organomegaly. Back: No tenderness to palpation in the thoracic, lumbar or sacral spine. Extremities: No cyanosis, no clubbing, no edema. No obvious deformities. Neurologic: The patient is a Glascow Coma Scale (GCS) of 7T. Some purposeful movement noted. The patient is intubated. Psychiatric: Unobtainable. Glascow Coma Scale: 7 Vital Signs: These are the vital signs for K.R. on the scene and at his arrival in the ED at 1055. Note a pain scale was not provided due to his lack of consciousness. EMS did a good job of stabilizing his vitals as evidenced by the chart below. Tachycardia was not present, however, he was hypothermic. Oxygen saturation was poor and then improved as well as respirations after intubation. Note that the patient minimal respiratory effort, most of the breathing effort was done by assist-control ventilator. No widened pulse pressure. Time 1036 1055 BP 134/95 128/99 P 86 90 RR 29 16 GCS 7 7 Osat 86 99% Temp 95.1 95.7 Lab Results: Lab results obtained in the emergency department submitted at approximately 1300. Hemoglobin Hematocrit WBC Platelet PT INR Lactic Acid Glucose BUN Creatinine Sodium Potassium Chloride 13.0 40.0 24.0 183,000 13.5 1.3 3.1 197 13 0.6 142 3.7 107 Low Low High Normal Normal High High High Normal Normal Normal Normal Normal Predicted Serum Osmolarity 299.6 mOsm/kg 4.6 points above normal but not high enough to be considered a gap. ABG: Results obtain in the emergency department submitted at approximately 1200. Note that the specific initial ventilator setting were unable to be found via EMR, however, see “Respiratory Assessment” for ventilator settings and ABGs for the following day. If the FiO2 was room air (21%) then these values would be fairly close to normal, however if FiO2 was 100% then these would be far from normal. PH pCO2 7.30 46 pO2 Bicarbonate 89 22 Urinalysis: All Normal. Drug Screen: Negative. Image Results 1. Chest X-Ray: Moderate opacity involving the right upper lobe. Differential diagnosis includes pulmonary contusion versus pneumonia. 2. Pelvic X-Ray: Negative, no mention of kidneys. 3. CT of the head: right frontoparietal subdural hemotoma, large scalp hematoma, parenchymal hemorrhage within the right frontal cortex, left temporal lobe, left thalamus, arachnoid cyst seen within the right middle cranial fossa and posterior fossa. 4. CT of the maxillofacial: negative ECG: Normal Sinus Rhythm Treatment Provided in Emergency Department: The patient was seen and evaluated in the emergency department immediately upon arrival where all imaging and diagnostic tests were completed. Access devices included two 18-guage peripheral IV’s (Left A/C and right A/C), one arterial line in the right radial and a central line. The patient was then admitted to the NICU after surgery with critical care orders. The plan at this time was to keep the patient on the ventilator and wean as appropriate, monitor lab values and treat them according while they wait for further instruction from the neurosurgeon. Impression: Status is post motor vehicle accident with intracranial hemorrhage including right frontoparietal subdural hematoma as well as a parenchymal hemorrhage. A large scalp hematoma is present as well as a large scalp laceration, which was repaired with staples. A right pulmonary contusion versus aspiration pneumonia and traumatic respiratory failure, requiring intubation. Lactic Acidosis is also present. Traumatic brain injury (TBI) is a major cause of morbidity and mortality worldwide. The modern management of severe TBI has fallen into the area of a multidisciplinary team led by neurointensivists, neuroanaesthetists, and neurosurgeons. Patient care is based on the avoidance of secondary injury, maintenance of cerebral perfusion pressure (CPP), and optimization of cerebral oxygenation. After viewing the information above I can gather the severity of this case and prepare myself for what to expect as the day progresses. Guidance by the licensed nurse in addition to my clinical instructor allowed me to be confident as I began the day caring for K.R. Patient Information: Patient Initials: K.R. Age: 15 Height: 5’9” Weight: 65.3 kg Allergies: NKA Social and Family Background: Due to immediacy of the situation, the family dynamic, and the widespread locations of the passengers in the accident there was no information in his St. Mary’s chart relative to a social and family assessment for K.R. However, his aunt came in around 1300 during my shift and I had the opportunity to sit down with her and gather some information regarding his family and social background. She explained to me that the woman driving the vehicle was, in fact, his biological mother but the two other boys in the vehicle were his half-brothers. His mother remarried and had 2 boys with another man, K.R’s stepfather. She also explained to me that K.R’s biological father had not been around for some time and his whereabouts were unknown to her. She also described the 3 brothers as very close, displaying good relationships between them. She stated that the other 2 brothers were extremely worried and upset about K.R. but couldn’t see him due to their conditions following the accident. K.R’s aunt had just left Covenant ICU where K.R’s mother was located for 2 broken legs and several other injuries. The biological father of K.R’s 2 brothers had been upstairs most of the day with one of the other passengers and did not visit K.R once during my shift. His mother had been in contact via phone where we had been updating her on the status of her son for most of the afternoon. A social assessment revealed that K.R. is a freshman at a local high school where he is an accomplished wrestler and a beloved student. His aunt also explained that he has had some behavioral issues throughout childhood and adolescence. She described him as having anxiety, depression, panic disorder, and some violence towards others. Past Medical History: K.R’s mother revealed this client’s past medical history via phone during the morning of March 17th, 2013. This was the only information we had about his previous history since he was not in St. Mary’s electronic system. Note: the information regarding his health history was not obtained from his family doctor and the mother had been in severe emotional and physical distress during this time. During a brief phone call from the mother on Sunday night she provided the medical staff with information regarding his medical history. She explained that he has a history of mild seizures and takes medication to prevent them. She also confirmed his behavioral health history that the aunt would later explain to me. Known previous medical history by system: Neurovascular: Seizures, nonspecific HEENMT: Migraines, sinusitis Respiratory: None Cardiovascular: None Peripheral Vascular: None Gastrointestinal: None Genitourinary: None Musculoskeletal: Back pain, possible scoliosis Skin: None Hematology/Oncology: None Endocrine: None Behavioral Health: Anxiety disorder, depression, panic disorder, violence towards others Infectious Diseases: None Home Medication: Because of the aforementioned dynamics of this situation it was unknown the exact medication(s) that he was taking at home during the time of my care. As stated above we were able to obtain information relative to K.R’s history of seizures but the specifics of the diagnosis were unknown at that time including the exact medication(s) he was taking. However, the mother was able to explain to us that he was not taking anything currently for his behavior issues and that the only medication(s) he was taking were for seizure prevention. I was led to believe that someone was in the process of trying to obtain a pharmacy record, however, I was never notified of the results. Past Surgical History: According to the mother, grandmother, and aunt, K.R. has had no previous surgeries. Primary Diagnosis: K.R’s primary diagnosis is a severe traumatic Brain injury (TBI) with a thin right-sided frontoparietal subdural hematoma and bilateral punctate hemorrhages, suggestive of axonal injury. He also presents with small compound skull depression with overlying laceration in occipital parietal area. Pathophysiology: Traumatic Brain Injury: Traumatic brain injury (TBI) is the result of an external mechanical force applied to the cranium and the intracranial contents, leading to temporary or permanent impairments, functional disability, or psychosocial maladjustment. TBI can manifest clinically from concussion to coma and death. Injuries are divided into 2 subcategories: (1) primary injury, which occurs at the moment of trauma, and (2) secondary injury, which occurs immediately after trauma and produces effects that may continue for a long time. The physical mechanisms of brain injury are classified using the following categories: Impact loading (Collision of the head with a solid object at a tangible speed), Impulsive loading (Sudden motion without significant physical contact), Static or quasistatic loading (Loading in which the effect of speed of occurrence may not be significant). Impact loading, which is what caused K.R. TBI, causes trauma through a combination of contact forces and inertial forces. Inertial force ensues when the head is set in motion with or without any contact force, leading to acceleration of the head. Contact force occurs when impact injury is delivered to the head at rest. In this instance it was likely a combination of impact loading, impulsive loading and contact force that led to K.R’s TBI. Subdural Hematoma: The usual mechanism that produces an acute subdural hematoma is a high-speed impact to the skull as seen in this case. This causes brain tissue to accelerate or decelerate relative to the fixed dural structures, tearing blood vessels. Often, the torn blood vessel is a vein that connects the cortical surface of the brain to a dural sinus. The head trauma may also cause associated brain hematomas or contusions, subarachnoid hemorrhage, and diffuse axonal injury. Secondary brain injuries may include edema, infarction, secondary hemorrhage, and brain herniation. Diffuse Axonal Injury (DAI): Unlike brain trauma that occurs due to direct impact and deformation of the brain, DAI is the result of traumatic shearing forces that occur when the head is rapidly accelerated or decelerated, as may occur in auto accidents, falls, and assaults. It usually results from rotational forces or severe deceleration. Vehicle accidents are the most frequent cause of DAI. The major cause of damage in DAI is the disruption of axons, the neural processes that allow one neuron to communicate with another. Tracts of axons, which appear white due to myelination, are referred to as white matter. Acceleration causes shearing injury, which refers to damage inflicted as tissue slides over other tissue. When the brain is accelerated, parts of differing densities and distances from the axis of rotation slide over one another, stretching axons that traverse junctions between areas of different density, especially at junctions between white and grey matter. (ADD CITATION) Surgical Intervention: Name of procedures: Right parietooccipital craniotomy and elevation of depressed skull fracture, debridement and closure of right occipital parietal laceration, insertion of left frontal ventriculostomy. Patient tolerated the procedure well and was taken to ICU recovery room in a stable condition. Time of procedure: 1600 3-16-2014 My Day of Care: The following information, assessments and lab values all occurred during the 12 hours in which I was assigned to K.R. ***Diagnostic Testing/Lab Results: Lab results for 3-17-2014 at 1010, my day of care. Lab Results Normal Range Patient Correlation Test/other diagnostic testing WBC 14 mm3 5-10 mm3 High. Within minutes of a traumatic impact, a robust inflammatory response is elicited in the injured brain. The complexity of this post-traumatic squeal involves a cellular component, comprising the activation of resident glial cells, microglia, and astrocytes, and the infiltration of blood leukocytes RBC 4.7 4.5-5.5 WNL. Tells how many red blood cells you have. Helps diagnose anemia and other conditions affecting red blood cells Hgb 13 g/dl 12-15 g/dL WNL. Protein found on the RBC that gives blood its red color. Hgb is composed of iron and carries oxygen. Hct 41% 36-46 % WNL. Hct is the volume of packed red blood cells found in 100 ml of blood. Tells the concentration of RBC in the blood. Platelet 152 150-400 WNL. Basic elements in the blood Count that promote coagulation. Neutrophils 73% 50-70 % High. Most numerous circulating WBC. Body’s first line of defense. They respond to inflammatory and tissue injury. High. Immune response with T cells and B cells. Lymphocyte 37% 25-35 % Monocyte 5.4% 4-6% Ingest large particles of debris. Second line of defense. Eosinophil 2.8% 1-3% WNL. Basophil 1% 0.4-1.0% Increase during the healing process. PT 13.5 seconds 10-12 seconds High: A limited trauma-induced coagulopathy as evidence by prolonged PT levels has been found in patients hospitalized for head injury, but PT levels return to normal after 12 hours and the clinical importance of this prolongation is currently unclear INR 1.4 2-3 PTT Not provided BUN 7 mg/dl 20-30 seconds 1.5-2 x normal value (40-75 seconds with a PE) 5-25 mg/dL Creatinine 0.5 mg/dl 0.5-1.5 mg/dL WNL. Used to diagnose renal dysfunction. GFR Ca++ Not calculated for ages <18 7.8 mEq/L 8.5-10.5 mEq/L Low: K+ 3.8 mEq/L 3.5-5.0 mEq/L WNL. Na+ 144 mEq/L 135-145 mEq/L WNL. Sodium (Na+) is the major cation in the extracellular fluid and plays a major role in maintaining osmotic pressure of extracellular fluid, regulating potassium and chloride levels, stimulating neuromuscular reactions, and maintaining systemic blood pressure. Alterations in serum sodium levels are critical in patients with head injuries Hyponatremia may be due to the syndrome of inappropriate antidiuretic hormone (SIADH) or cerebral salt wasting. Both Cl- 114 mmol/L 98-106 mmol/L Mg 1.5 mg/dl Glucose 104 60-110 mg/dl Predicted Serum Osmolarity 296.3 285-295 mOsm/kg. The measured osmolality should not exceed the predicted by more than 10 mOsm/kg. A difference of more than 10 mOsm/kg is considered an osmolal gap . syndromes involve decreased serum sodium level in the face of increased urinary sodium losses. Elevated sodium levels in head injury indicate simple dehydration or diabetes insipidus. High: Chloride is the most plentiful extracellular anion in the body. It carries a negative charge and serves to maintain electrically neutrality with cations. Magnesium is depleted in the acute phases of both minor and severe head injuries. Because this cation blocks the excitotoxic response and functions as an antioxidant, careful monitoring of magnesium may improve outcomes. There is substantial evidence highlighting the adverse effects of hyperglycemia in critically ill patients and tight glycemic control has become a part of the routine management of general intensive care patients. Hyperglycemia has been associated with increased cerebral lactate resulting in local brain tissue acidosis. Slightly high but not high enough to be considered an osmolal gap. Serum osmolarity is a good indicator of dehydration and over hydration. Importance of Diagnostic Tests: Medications: Medication Indication Dose Route Frequency Drip 5mcg/kg/min 10 mg/ml Continuous 24 hr Diprivan (propofol) Chemical class: 2,6diisopropylphenol derivative Therapeutic class: Sedative-hypnotic Pregnancy category: B To provide sedation for critically ill patients in intensive care Sublimaze (fentanyl) Indicated for the Drip management of 1mcg/kg/hr persistent, .3ml/hr Side Effect Contraindications Patient Correlation Diprivan is not recommended in hypothermic patients as it has a tendency to accumulate and precipitate hyperlipidaemia. Other reported problems with propofol include precipitous cardiovascular collapse and the propofol infusion syndrome of metabolic acidosis, rhabdomyolysis, and bradycardia, first described in children but also identified in adults. Adequate sedation minimizes pain, anxiety, and agitation, reduces the cerebral metabolic rate of oxygen consumption, and facilitates mechanical ventilation. This is achieved with sedative drugs. Propofol is preferred because of its superior metabolic suppressive effects, and favorable short half-life. 46 CNS: Agitation, amnesia, anxiety, asthenia, As an adjunct to sedation therapy, Chemical class: Opioid, phenylpiperidine derivative Therapeutic class: Analgesic, anesthesia adjunct Pregnancy category: C Controlled substance schedule: II norepinephrine (Levophed) Chemical class: Catecholamine Therapeutic class: Cardiac stimulant, vasopressor Pregnancy category: C moderate to severe chronic pain in opioid tolerant patients Continuous 24 hour To treat acute hypotension, cardiogenic shock, and septic shock 1mg/ml at 4ml/hr titrate for MAP>80 ataxia, confusion, delusions CV: Asystole, bradycardia GI: Anorexia, constipation RESP: Apnea, depressed cough reflex Contraindicated: Under age 2, asthma, myasthenia gravis, opioid hypersensitivity or intolerance, significant respiratory depression, upper airway obstruction; transmucosal form: acute or chronic pain Contraindicated: Concurrent use of hydrocarbon inhalation anesthetics, hypersensitivity to norepinephrine or its components, hypovolemia, mesenteric or peripheral vascular thrombosis Side effects: CV: Angina, bradycardia, ECG changes GI: Nausea, vomiting GU: Decreased renal perfusion RESP: Apnea, dyspnea SKIN: Pallor Sliding Scale Insulin To treat acute Maintaining Side effects: fentanyl is provided in regular doses, which has minimal effects on cerebral hemodynamics in adequately resuscitated patients. Important component in maintaining blood pressure to a level adequate enough to profuse the body but more importantly the brain. Also note that fentanyl is a hypotensive agent so caution must be taken with order changes. The stress mannitol (Osmitrol) Chemical class: Hexahydroxy alcohol Therapeutic class: Antiglaucoma, diagnostic agent, osmotic diuretic, urinary irrigant Pregnancy category: B hyperglycemia related to body response to accident glucose rates between 80120 -Hypoglycemia To reduce intracranial or intraocular pressure 30g IVPB every 6 hours 150ml/hr Contraindications: Active intracranial bleeding (except during craniotomy), anuria, hepatic failure, hypersensitivity to mannitol or its components, pulmonary edema, severe dehydration, severe heart failure, severe pulmonary congestion, severe renal insufficiency Side effects: CNS: Chills, dizziness, fever, headache, seizures CV: Chest pain, heart failure, hypertension, tachycardia, thrombophlebitis EENT: Blurred vision, dry mouth, rhinitis GI: Diarrhea, nausea, thirst, vomiting GU: Polyuria, urine retention RESP: response in trauma patients, including those with severe TBI, generates a hypercatabolic state leading to rapid muscle protein breakdown and hyperglycaemia Hyperosmolar therapy is a key intervention for the management of cerebral edema and raised ICP after TBI. It is particularly indicated for acute rises in ICP as it has a rapid effect. Mannitol, an osmotic diuretic, is commonly employed and the immediate efficacy is likely to result from a plasmaexpanding effect and improved blood rheology due to a reduction in hematocrit. Pulmonary edema pantoprazole (Protonix) peptic ulcer disease prophylaxis 40mg iv push once daily Side effects: CNS: Anxiety, asthenia, confusion, dizziness, headache, hypertonia, hypokinesia, insomnia, malaise, migraine, speech disorder vertigo CV: Chest pain, hypercholesterolemia, hyperlipidemia EENT: Anterior ischemic optic neuropathy, blurred vision, increased salivation, pharyngitis, rhinitis, sinusitis, tinnitus ENDO: Hyperglycemia GI: Abdominal pain, atrophic gastritis, constipation, diarrhea, elevated liver function tests results, flatulence, gastroenteritis, hepatotoxicity, indigestion, nausea, pancreatitis, vomiting GU: Elevated serum creatinine level, interstitial nephritis Chemical class: Substituted benzimidazole Therapeutic class: Antiulcer, gastric acid proton pump inhibitor Pregnancy category: B Potassium Chloride Contraindications: Hypersensitivity to pantoprazole, Electrolyte balance/ 20mEg IV in NS at Contraindications: Urinary retention, Peptic ulcer disease prevention due to increased medication load on stomach. In the TBI patient with hydration 100ml/hr via central line hyperkalemia. Side effects: · confusion, anxiety, feeling like you might pass out; · uneven heartbeat; · extreme thirst, increased urination; · leg discomfort; · muscle weakness or limp feeling; cefazolin (Ancef) To treat pneumococcal pneumonia 1000 mg IV push every 12 hours Chemical class: Firstgeneration cephalosporin, 7aminocephalosporanic acid Therapeutic class: Antibiotic Pregnancy category: B levetiracetam (Keppra) Contraindications: Hypersensitivity to cephalosporins or their components Side effects: CNS: Chills, fever, headache, seizures CV: Edema EENT: Hearing loss GI: Abdominal cramps, diarrhea, elevated liver function test results, hepatic failure, hepatitis, hepatomegaly, nausea, oral candidiasis, pseudomembranous colitis, vomiting GU: Elevated BUN and serum creatinine levels, nephrotoxicity, renal failure, vaginal candidiasis As adjunct to treat partial seizures 500 mg IV every 12 hours Contraindications: Hypersensitivity to levetiracetam or its raised ICP, sudden changes in serum sodium concentration and osmolarity must be avoided since these factors impact on the nature and degree of cerebral edema With the possibility that K.R. aspirated he is at an increased risk to develop pneumonia. Anti-epileptics should not be prescribed components Chemical: Pyrrolidine derivative Therapeutic: Anticonvulsant Pregnancy category: C Normal Saline Drip Side Effects: CNS: Abnormal gait, aggression, agitation EENT: Amblyopia, conjunctivitis GI: Anorexia, constipation, diarrhea MS: Neck pain RESP: Asthma, cough SKIN: Alopecia, ecchymosis Hydration 1000 ml at 100ml/hr Side effects: Febrile response, infection at the site of injection, venous thrombosis or phlebitis extending from the site of injection, extravasation, and hypervolemia. unless there is documented clinical or EEG evidence of seizures, which in this case there is a previous medical history of seizures. TBI patients are susceptible to disorders of salt and water balance. Causes include central diabetes insipidus (CDI), cerebral salt wasting (CSW) syndrome, and syndrome of inappropriate anti-diuretic hormone (SIADH) secretion Physical Assessment: 1200 on 3-17-2014 my day of care Time 0700 0800 0900 1000 1100 BP 129/58 130/61 144/63 124/60 143/57 HR 62 67 72 66 63 RR 16 16 16 16 16 Temp 96.8 96.8 96.7 97.5 97.3 O2 Sat 100 100 100 100 100 MAP 81 84 90 81 85 CPP 66 66 71 65 70 ICP 15 18 19 16 15 1200 154/64 68 16 97.5 100 94 73 21 Neurological Assessment: K.R was unresponsive; sedated and ventilated during my entire shift. He remained in a calm state throughout the day. His pupils were round, 3mm in size and sluggish when presented with light. During my Glascow Coma Scale he presented with no verbal response, no eye opening and a bilateral flexion withdraw to pain for a score of 6. His motor ability was minimal but he did present with both upper and lower flexion withdrawal on both sides. When prompted to squeeze my fingers there was no response bilaterally, however, damage to his temporal lobe cannot be ruled out as he may be able to hear me but his auditory center for sound interpretation could be damaged. Muscles of the extremities were flaccid. Throughout the morning K.R. showed no signs of voluntary movement, however, towards the later afternoon his left arm moved spontaneously several times. As shown in the vitals chart above his Cerebral Perfusion Pressure (CPP) remained above near 70. After brain injury, cerebral blood flow may be lowered to the ischaemic threshold. To prevent further neuronal death (the secondary brain injury), this flow of well-oxygenated blood must be restored. Cerebral Perfusion Pressure may be maintained by raising the Mean Arterial Pressure (MAP, which remained above 80 via norepinephrine) or by lowering the Intracranial Pressure (ICP, which remained below 20mmHg). In addition to controlling CPP, adequate sedation minimizes pain, anxiety, and agitation, reduces the cerebral metabolic rate of oxygen consumption, and facilitates mechanical ventilation. This is achieved with sedative drugs and opioids. Propofol is preferred because of its superior metabolic suppressive effects, and favorable short half-life. Analgesia was provided with fentanyl, which has minimal effects on cerebral hemodynamics in adequately resuscitated patients. Cardiovascular Assessment: Normal sinus rhythm on patient’s telemetry monitor (Lead II). Regular rate and rhythm of S1 and S2 heart sounds. Left and right radial, brachial, femoral and dorsalis pedis 2+ bilaterally. No clubbing, pink nail beds, capillary refill <2 seconds in toes and hands. Jugular venous distention absent. Upper and lower extremities were warm to the touch bilaterally. Murmur or rub not present. Blood pressure was high in response to norepipenephrine. Hypertensive readings in this case are okay because higher blood pressure may be maintaining cerebral blood flow. No cardio-related changes occurred throughout the day. Pulmonary Assessment: K.R. was mechanically ventilated via endotrachial tube by EMS. He remained mechanically ventilated on assist-control mode throughout the day with orders to wean, however, his settings remained the same throughout the day. The ventilation settings were as follows: Vent Humidifier Temp: 35 degrees Celsius, FiO2: 50%, Tital Volume: 450ml, Set Rate (Breath/min): 16/min, Peak Inspiratory Pressure: 15cm H2O, Flow Rate: 40L/min, PEEP: 5. His breath sounds were clear bilaterally with a productive cough presenting with small amounts of thin, white sputum, which was suctioned intermittently throughout the day. He did not breath over the ventilator at all which may indicate a minimal to no respiratory effort. His pulse oximetry never dropped below 99%. Patients with severe head injury require mechanical ventilation to maintain an arterial Po2 and Pco2 between 4.5. No changes in respiratory status occurred during my shift. GI: No symptoms. Abdomen rounded, soft, symmetric and non-tender. Bowel sounds active x 4. His last bowel movement was unknown. No bowel movements during shift. Note that the patient is taking protonix once daily for peptic ulcer disease prophylaxis. At the time of assessment K.R. was NPO, however, it had been suggested that he start enternal feedings via O/G tube with osmolite at 30ml/hr and increase with tolerance by 10 ml increments every 8 hours until 55ml/hr to reach goal of 1980 kcals/day and 83 grams of protein/day. Total caloric intake including propofol would be 2112 kcals/day. It’s important to remember that as he is weaned off the propofol in the future his enteral feeding rate with need to increase to make up for the kcals. Enternal feeding started at approximately 1300 during my day of care. No changes in GI throughout the day. GU: Foley catheter: patent with urine yellow and clear. Secured via tape on his thigh. Bladder distention was absent. Due to his traumatic brain injury and heavy sedation a Foley catheter is needed to prevent urinary retention. The prior 12 hours before my assessment his intake was 3485 ml and his output was 2,965 ml for a net of 520 ml. He continued to display adequate voiding patterns throughout the day. No urinary changes occurred throughout my shift. Integumentary: Skin was warm, dry, pink, elastic and intact. Mucus membranes were pink and moist. Elastic skin turgor and hydration as evidence by minimal tenting on the back of his hands. Braden scale: limited response to painful stimuli, occasionally moist skin, confined to bed, very limited mobility, inadequate nutrition. Braden scale score of 12. Patient has several minor scrapes on legs that do not require attention. Overall his skin was in remarkable shape given the circumstances of the accident. Patient position was changed every 2 hours to provide adequate profusion. No integumentary changes occurred during my shift. IV Assessment: Access devices included two 18-guage peripheral IV’s (Left A/C and right A/C), one arterial line in the right radial and a central line. All devices were inserted the day before in the emergency department. All insertion points were dry, intact, non edematous and warm. No changes in IV assessments throughout the day. Activity: Patient is unresponsive and heavily sedated; activity type is bed rest. Orthotics included a hard cervical collar as precaution for re-injury and intermittent pneumatic compression devices for blood circulation and DVT prevention. Patient spontaneously moved a handful of times but otherwise he was completely motionless. No changes in activity during my shift. Psychosocial/Spiritual: Unable to asses due to unresponsiveness and heavy sedation. Family support was minimal but the aunt showed genuine concern and was very supportive of the nursing staff. Educational Needs: Once again this area was impossible to assess due to the patient’s status. It is apparent that the family as a whole needs education regarding seatbelt safety. I was not in contact with the mother therefore I could not assess her educational needs specifically. The aunt understood the plan of care and was supportive of our efforts. Prevention/Plan: As previously stated the general plan for TBI is based on the avoidance of secondary injury, maintenance of cerebral perfusion pressure, and optimization of cerebral oxygenation. In this case there are several steps to the plan for K.R. The patient had displayed a pattern of optimal cerebral perfusion via MAP and ICP measures throughout the day. Therefore, part one of the plan is to continue this trend to prevent secondary injury and other complications. Part two of the plan is to wean him off of the ventilator slowly by decreasing the FiO2 by 5 every 2-4 hours while closely monitoring arterial blood gases to insure appropriate reading relation to specific FiO2 measures. Part three of the plan includes continuing protonix therapy for PUD prevention and antibiotic therapy while the patient has drains. Infection avoidance is important in any ICU case but it is extremely important with brain injuries due to the detrimental effects of the inflammatory response on a recovering brain. Part four of the plan includes the nutritional outline previously mentioned in the “GI Assessment”. Lastly, there is a need for family support. Within the coming weeks they expect the number of visitors to increase dramatically. It is important to allow K.R. a quiet, cool, non-stimulating environment while his brain begins to heal. Increasing numbers of visitors could stimulate K.R. to the point of raising his ICP to dangerous levels. Balancing patient advocacy and family visitation will be a topic that must be discussed amongst the nursing staff. Priority NANDAs, NICs, and NOCs: NANDA 1: Fall risk related to altered level of consciousness and limited mobility as evidenced by impaired judgment. NIC: Assess safety needs, bed in low position/side rails up, call bell within reach, initiate precautions, floor uncluttered, restraints as needed. NOC: No falls or injuries to self or staff NANDA 2: Acute pain related to diagnostic/surgical procedure, medical treatment, and trauma as evidenced by changes in vital signs and restlessness. NIC: Assess for causes of pain, evaluate response to pain, monitor signs and symptoms associated with pain. NOC: Stable vital signs, no restlessness, no symptoms associated with pain, exhibits increased comfort. NANDA 3: Disturbed sensory perception related to neurological trauma as evidenced by altered communication patterns, altered thought process, disorientation. NIC: Assess sense of touch, eliminate extra stimuli, promote safe environment, reorient frequently. NOC: Improved sensory perception, no anxiety related to orientation, successful alternatives to communication. NANDA 4: Impaired gas exchange related to altered delivery of oxygen, altered oxygen carrying capacity of blood as evidenced by cyanosis, dyspnea, hypoxia, tachycardia. NIC: Administer medications as ordered, auscultate breath sounds at least every 2-4 hours or as needed, change position every 2 hours, monitor ABGs. NOC: Demonstrates improved ventilation and oxygenation of tissues, baseline respiratory rate for patient, ABGs and pulse oximetry in normal range.