What physical exam will be most helpful for diagnosis?
advertisement

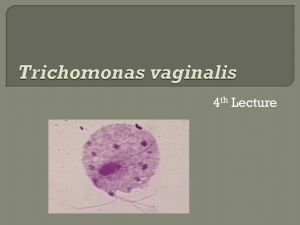
HPI • A 23 year-old female comes to your office complaining of vaginal discharge, itching, and burning with urination for several days. The symptoms had worsened during her menstrual period. She has had a similar infection in the past, but she doesn't remember what it was. She only remembers that she took 4 pills for it in the office and it went away. HPI cont'd Medical Hx: none Social Hx: College student studying biology. Sexually active with one new male partner for the last 2 months. Does not smoke. Drinks 2-3 beers on weekends with friends. Meds: none Family Hx: father with HTN What physical exam will be most helpful for diagnosis? Physical Exam Vital Signs: all normal Speculum exam shows frothy, green, malodorous discharge. Cervix has small, red, punctuate hemorrhages. ROS: normal other than in HPI Cervix on exam What is your differential diagnosis? Image from pediatrics.georgetown.edu, “Week 28, Case 1,” retrieved 12/28/2012 http://pediatrics.georgetown.edu/residents/visualdiagnosis/week28 Differential Diagnosis • Trichomoniasis • Chlamydia • Gonorrhea • Bacterial Vaginosis What is your next step? Any tests you want to order/perform? Lab Results • • Wet mount shows many PMNs and motile organisms. No clue cells are seen. There are other options for diagnosis: culture or rapid antigen tests. However, if trichomonads are seen on wet mount, these are unnecessary. PMNs Trichomonads Image from pediatrics.georgetown.edu, “Week 28, Case 1,” retrieved 12/28/2012 http://pediatrics.georgetown.edu/residents/visualdiagnosis/week28 Trichomoniasis • Caused by flagellated protozoan trichomonas vaginalis. • Sexually transmitted. Can have asymptomatic carrier phase, increasing transmission from partners who do not know they have the disease. • High prevalence of co-infection with other sexually transmitted diseases Image from UpToDate, “Trichomonas vaginalis,” retrieved 12/28/2012 Treatment • Metronidazole or tinidazole, 2 grams orally x1 • Longer courses of treatment are available, but they do not improve cure rates. Instead, they decrease compliance. Is there anything else you want to do? You need to treat her partner! • Because the disease is sexually transmitted, you need to treat your patient's partner as well! He may have an asymptomatic infection and cause re-exposure to the disease even after she is treated. • Patients should avoid sexual contact for approximately one week to avoid re-infection. What if your patient is 22-weeks pregnant? Trichomoniasis in Pregnancy • Trichomoniasis is believed to be associated with preterm delivery and infection in pregnant women. However, it is currently not recommended to treat asymptomatic infection in pregnancy, as this does not reduce these risks. • Also, if she were near term, she could possibly transmit the infection to her newborn at delivery. • Treatment in pregnancy is metronidazole. Summary • Trichomoniasis is a common sexually-transmitted infection caused by the protozoan trichomonas vaginalis. • Characteristic symptoms include green, frothy, malodorous discharge, pruritis, and dysuria. Physical exam may show a “strawberry cervix.” • Wet mount will show many neutrophils, motile trichomonads. It will not usually show clue cells (associated with bacterial vaginosis). • Treatment is with metronidazole. All sexual partners should also be treated, and sexual contact should be avoided for 7 days following treatment to prevent reinfection.