Atrial Fibrillation: Strategies for the Acute Conversion
advertisement

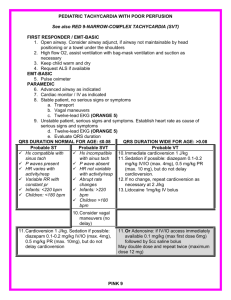
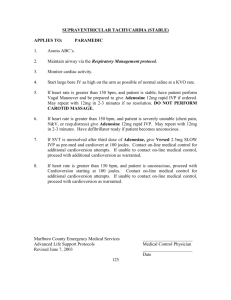
Converting Atrial Fibrillation to NSR Pills or Electrical Thrills Peter Holzberger MD www.mediclicks.net Background • Atrial fibrillation is the most common sustained arrhythmia • Affects 2 million Americans • 6% over the age of 65 experience it • Responsible for 15% strokes – Benjamin E: Epidemiology of Atrial Fibrillation. In Falk RH, Podrid PJ, eds:Atrial Fibrillation: Mechanisms and Management. 2nd Ed, Lippincott-Raven Press, New York 1997, pp.1-22. Symptoms • • • • Inappropriate heart rate response Irregular rate Loss of atrial systolic function Thromboembolism Choices for Immediate Treatment • Anticoagulation and Rate Control • Or • Conversion to NSR NSR-Pills Or Electrical Thrills • Pills – Placebo – Single Dose Antiarrhythmic Treatment – Ibutilide • Electrical Thrills – Traditional External Cardioversion – Double External Cardioversion – Biphasic Cardioversion Choices • 40 yr old healthy female with 6 hrs of palpitations. First time ever. • Found in atrial fib. Rate slowed with IV lopressor, and patient feels much better. • ED evaluation entirely normal • Next step is ? Choices • A) DC Cardioversion • B) P.O. Propafenone • C) Discharge on p.o. lopressor and revaluate next day • D) Admit for further workup and treatment Predictors of Conversion to NSR • Duration of atrial fib – <24 hrs spontaneous conversion in up to 66% • Underlying cardiac function • Underlying cardiac disease • Age Pills - Placebo • Conversion of recent onset paroxysmal atrial fibrillation to normal sinus rhythm: The effect of no treatment and high-dose amiodarone. A randomized, placebo controlled study – 100 patients PAF (<48 hrs) – IV Amiodarone (3 gms) vs. IV Placebo – Cotter et al,.Eur Heart J Dec 1999; 20(24):1833-42 Placebo Conversion (%) 100 90 80 70 60 50 40 30 20 10 0 P=0.0017 92 64 IV amiodarone IV Placebo 24 hrs – Cotter et al,.Eur Heart J Dec 1999; 20(24):1833-42 Choices • 45 yr old on Coumadin for recent DVT presents with several day history of palpitations. • INR has been therapeutic for several months • Rate is controlled but still feels poorly • Evaluation entirely unremarkable • What next? Choices • A) DC Cardioversion • B) P.O. Propafenone • C) Discharge on p.o. lopressor and revaluate next day • D) Admit for further workup and treatment Pills - Single Dose Rx – Boriani et al, Pacing Clin Electrophys Nov 1998; Vol.21 Part II, 2470-74 Single Dose • 417 patients with AF < 8 days • Randomized to – Placebo – IV Amiodarone 5mg/kg bolus followed by 1.8 gms/24hrs – IV Propafenone – PO Propafenone 600 mg – PO Flecainide 300 mg – Boriani et al, Pacing Clin Electrophys Nov 1998; Vol.21 Part II, 2470-74 Single Dose 100 80 Placebo IV Amio IV Prop PO Prop PO Flec 60 40 20 0 SR≤1 hr SR≤3hr SR≤8hr – Boriani et al, Pacing Clin Electrophys Nov 1998; Vol.21 Part II, 2470-2474 Choices • 45 yr old female with several week history of worsening SOB, no palpitations • Exam reveals, mild CHF, A fib rate 140, Echo EF 35%-global hypo • What next? Choices • A) DC cardioversion • B) p.o. Propafenone • C) Discharge on p.o. lopressor and revaluate next day • D) Admit for further workup and treatment Anticoagulation Prior to Conversion to NSR • At least 3 weeks Therapeutic INR >2.0 • Unless arrhythmia is less than 48 hours in duration – Even then heparin has been advocated in high embolic risk patients • Mitral stenosis, CHF, previous emboli – Chest. Sixth ACCP Consensus Conference on Antithrombotic Therapy Vol. 119(1) Suppl. Jan 2001 194S-206S www.mediclicks.net TEE Prior to Conversion to NSR Thrombus Pills (sort of) -Ibutilide Pills (sort of) -Ibutilide Pills (sort of) -Ibutilide Ibutilide – Stambler et al, Circulation October 1996; Vol 94, No 7, 1613-21 Ibutilide • 266 patients (3 hrs to 45 days) – 133 with atrial flutter – 133 with atrial fibrillation • Randomized to – Placebo/Placebo – 1mg/0.5mg – 1mg/1mg – Stambler et al, Circulation October 1996; Vol 94, No 7,1613-21 Ibutilide – Stambler et al, Circulation October 1996; Vol 94, No 7,1613-21 Ibutilide • Proarrhythmia – PMVT developed in 8.3% • Sustained PMVT 1.7% – MMVT developed in 4% • QTc prolonged an average of 63 msec. • No hemodynamic effects – Stambler et al, Circulation October 1996; Vol 94, No 7,1613-21 Ibutilide • Contraindications – – – – – – Hx of Torsades QTc > 440 K< 4.0 mEq/L Concomitant Type 1 or III drug HR <60 Severe LV dysfunction (EF < 30%) Ibutilide • Key Points – Close monitoring during infusion • For NSR, PMVT (3 beats), QTc >600msec, conduction or hemodynamic problems – Monitor post infusion for at least 4 hours or until QTc returns to baseline – (longer with hepatic dysfunction) – Trained personnel, defibrillator, Code Cart and IV magnesium should be present Pills Or Electrical Thrills • Pills – Placebo – Single Dose Antiarrhythmic Treatment – Ibutilide • Electrical Thrills – Traditional External Cardioversion – Double External Cardioversion – Biphasic Cardioversion Electrical Thrills - DC • Used for conversion of atrial fib by Dr Bernard Lown in the 1960’s – 94% of 456 cases of atrial fib • Overall efficacy felt to be about 85% • Use of high energy (360J) associated with skin burns and possible myocardial stunning DC Cardioversion • Efficacy dependent on – – – – Paddle size and position Transthoracic impedance Energy Waveform Underlying disease Paddle Position • Anterior/Posterior #1 Paddle Position • Anterior/Posterior #2 Paddle Position • Anterior/Anterior Transthoracic Impedance • Lowered by putting pressure on the anterior paddle during cardioversion Electrical Thrills - Double DC – Saliba et al, J Am Coll Cardiol 1999; Vol.34, No 7: 2031-34 Double External Cardioversion • Double Shock Double External Cardioversion • 55 patients who had all failed conventional DC cardioversion • 84% success rate – 9 patients received more than one 720J • No complications • Saliba et al, J Am Coll Cardiol 1999; Vol.34, No 7: 2031-34 Pills and Electrical Thrills – Oral et al, NEJM 1999, Vol. 340 No24:1849-54 Ibutilide and DC Cardioversion • 100 consecutive patients – 50 assigned conventional DC – 50 pretreated with 1 mg Ibutilide 100 100 P<0.001 90 72 80 70 DC only 60 50 Ibutilide/DC 40 30 20 –10 Oral et al, NEJM 1999, Vol. 340 No24:1849-54 0 % Success Ibutilide and DC Cardioversion • 20% treated with Ibutilide converted without DC • 14 patients who did not convert with DC alone were then pretreated with Ibutilide – None converted with drug alone – All converted with DC • Oral et al, NEJM 1999, Vol. 340 No24:1849-54 Electrical Thrills Damped Biphasic Biphasic - AF • 165 patients randomized to monophasic vs. biphasic shocks – Stepped approach • Biphasic: 70,120,150,170 • Monophasic:100,200,300,360 – Mittal et al, Circulation March 2000,Vol.101(11): 1282-87 Biphasic - AF – Mittal et al, Circulation March 2000,Vol.101(11): 1282-87 Conclusion • Prior to conversion: – A fib less than 48 hrs or, – Anticoagulation with an INR >2.0 for 3 weeks, or – TEE showing no clot at time of conversion • Pills work about 40% of the time • Electrical Thrills work about 90% of the time Conclusion • Biphasic waveform is superior and desirable • Ibutilide will have a role – unable to perform anesthesia – very effective for atrial flutter – facilitate DC cardioversion www.mediclicks.net