Foundations of Group Therapy
advertisement

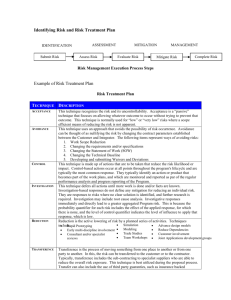
Running head: FOUNDATIONS OF GROUP THERAPY Foundations of Group Therapy Dayle Lauren Stenberg College Good! 1 FOUNDATIONS OF GROUP THERAPY 2 Abstract Nurses must be skilled in various areas of communication as it is an integral part of working with individuals and groups. A closer look at the dynamics of group therapy reveals that there is inherent benefit to many patients with mental illness in partaking in group psychotherapy. Groups can be formed with the intent of offering education, support or sharing, or to offer a means to an end for a common underlying problem. As nurses, there is a need to develop skills both as group leaders and group members in order to intervene therapeutically with patients and families. By examining the characteristics of the group such as the importance of cohesiveness, transparency and transference, and the role of the therapist through the group dynamics, the foundation of group development is better understood and subsequently initiated and therefore more successful. The knowledge gained from group experiences not only crosses the nursepatient barrier but also works for the nurse in the professional giving understanding of any group’s particular function and the roles of attending members: during this process, a nurse ultimately becomes more self-aware and relational throughout therapeutic relationships. FOUNDATIONS OF GROUP THERAPY 3 Foundations of Group Therapy Group therapy has been cited by many researchers as being highly beneficial to individuals with many mental illnesses. The consensus is that group therapy benefits those who at first undergo individual therapy in relation to their mental health issues before entering the group milieu. There are many theories that abound psychotherapy, and yet a few foundational elements exist as a common thread through most. This paper will highlight these as proper group development, the importance of group cohesion, the phenomenon of transference and transparency in the group setting, as well as the interjection of basic tasks expected of the group facilitator along the way. A group is defined as consisting of three or more people with a common goal or interest (Kearney-Nunnery, 2012). In psychotherapy, the interplay of interactions among group members, otherwise known as the group process, (a form of a social system), focus on a specific group goal that is outlined by the group facilitator. Groups can be classified by their structure, composition, roles and their overall focus (Kearney-Nunnery, 2012), (Yalom & Leszcz, 2005). Regardless of the classifications of a group, effective groups have an identified purpose or need and a commitment to the group process (Kearny-Nunnery, 2012). As Yalom & Leszcz posit, the group leader is effectively responsible for creating and maintaining the group (2005), while Kearney-Nunnery states that the facilitator also must tailor the group process to the developmental stages of the group; a feat that takes effective leadership and active participation by its members (2012). According to Tuckman (1965), a model of group development over time consists of originally four distinct stages which he labelled “forming”, “storming”, “norming”, and “performing” (Tuckman & Jensen, 1977, p. 420). Specifically, these four stages each encompass FOUNDATIONS OF GROUP THERAPY 4 a set of group settings and stages of task activities. These are illustrated as being the testing and dependence phase in which group members become oriented to the task at hand, or the forming’ stage (Tuckman & Jensen, 1977). This is followed by the other three stages in which there begins intergroup conflict and a subsequent emotional response to the demands of the task at hand, which he has labeled the ‘storming’ phase; the ‘norming’ stage that involves the development of group cohesion and the relative exchange of interpersonal interpretations; and the fourth ‘performing’ stage in which the solutions to the task become evident and the role relatedness of all the members becomes apparent (Tuckman & Jensen, 1977). As cited by Tuckman & Jensen, (1977), a final stage of development was also integrated into the Tuckman model over the years with further study, identified as ‘adjourning’ and was integrated into the theory of group development after the work of researchers such as Lacoursiere (1974), Mann (1967) and Braaten (1975) who felt he had overlooked this important final phase. Regardless, understanding these stages of group development is an important skill in nursing practice and as a group facilitator must be able to navigate and motivate group members through these stages effectively and accordingly. After all, these stages of group development run parallel to the concept of initial approach, working phase and termination of the therapeutic relationship between nurse and patient. The facilitator of the group must then decide the raison d’être, the selection and preparation of members, and the time and place for meetings (Yalom & Leszcz, 2005). During the forming stage of group development, group members become familiar with each other, the purpose of the group, and the expected outcome. A major group task during this stage is “establishing a group contract, developing trust and identification” (Arnold, 2007, p. 44, as cited by Kearney-Nunnery, 2012). One of the tasks of the facilitator at this time is to establish FOUNDATIONS OF GROUP THERAPY 5 a structure to the group that will allow for an effective working relationship, including setting up the room in a manner that is crucial to group development and feelings of emotional security (Kearney-Nunnery, 2012). During this phase, Kearney-Nunnery states that goal determination may need to be delayed in order to allow members to participate in goal development naturally (2012). In a presentation done by Yalom, (n.d.) he expresses that the basic three tasks of the group facilitator are the creation and maintenance of the group; culture building; and activation and illumination of the ‘here-and-now’ (Yalom, n.d.). The storming and norming phases of group development have arguably been stated to be all one stage by researchers such as Lacoursiere (1974) who believed members’ expectations became more realistic and their desire to learn what they needed to do became clear (Tuckman & Jensen, 1977). Although members become more comfortable with the group, it will likely start out with a show of ambivalence about the need for the group and its intended goals (KearneyNunnery, 2012). During this phase, the authority and competency of the facilitator will be tested and through this phase, the identification of behavioural standards and expectations will become known more clearly (Kearney-Nunnery, 2012). It is during this stage of development that the group will also begin to show intergroup dynamics that will be characteristic of this particular group: traditional views of cooperation and conflict may be tested due to the racially and ethnically diverse membership base and the overall homogeneity or heterogeneity of the group (Kearney-Nunnery, 2012), (Yalom & Leszcz, 2005). Understanding the relationship between intragroup and intergroup dynamics and relations is not only practical but significant for its theoretical value: understanding social dynamics then requires a commonality between intra/intergroup theories (Dovidio, Saguy, & Shnabel, 2009). This awareness is especially important in maintaining group harmony and relieving potential group tensions. Dovidio et al., FOUNDATIONS OF GROUP THERAPY 6 (2009) posit that the naturally occurring dynamic tensions that exist between group stability is not always an adaptive process, but rather, the tensions associated with change may be instead be more therapeutic as it allows the voice of disadvantaged individuals to be heard; potentially as a benefit to society as a whole. It is during this middle phase of group development, the storming and norming phase, that group cohesion becomes an important consideration in order to keep the group alive and healthy in its progress. In a 2008 study, researchers concluded that group cohesion could simply not be considered as a group-as-a-whole phenomenon, but rather had to include consideration of individual interpersonal relationship styles, motivation for membership, self/other differentiation processes, problems and transference dynamics (Crowe & Grenyer, 2008). Part of understanding the cohesion of the group is the therapist’s ability to measure group climate: the ability to capture the moments of group member perceptions or in other words, the degree to which members are actively engaged in the group therapy process (Crowe & Grenyer, 2008). According to Crowe & Grenyer, this stage consists of three phases: ‘engaged’, which is a reflection of the group’s alliance and cohesion; ‘avoiding’ which is reflective of the resistance apparent in group members to change; and ‘conflict’, a measure of the interpersonal tension and any mistrust that exists among the group (2008). When the group leader provides a positive, supportive and encouraging model to the members of the group, the cohesive esprit de corps can endure through this phase of development (Kearney-Nunnery, 2012). Conflict, however, can be the most challenging aspect of this stage of group development, and entails creative problem solving and direction from the facilitator to continually satisfy the group process through this phase (Kearney-Nunnery, 2012). Yalom cites Brabender, Fallon & Smolar (2004) as positing that there are eight dimensions to the group leader’s role at this time: directive vs. non-directive; FOUNDATIONS OF GROUP THERAPY 7 transparency vs. opaqueness; considerations of group as a whole/subgroup/interpersonal/ and individual; past/present and future; inside/outside group factors; content/process; understanding and the corrective emotional experience; and confrontation/ exploration versus support (Yalom, n.d.). Part of the challenge faced by the facilitator through the storming and norming phase is the issue of transparency and that of transference. The most influential of the dimensions outlined by Yalom (n.d.) is the facilitator’s ability to remain transparent at acceptable levels: too transparent and there are no boundaries and the facilitator then faces loss of the dual role of a leader, and not transparent enough and the group feels like a cold, unsafe place with very little spontaneous interaction. Yalom further posits that a prudent therapist or facilitator should know the intent of the transparency and its dynamic influence in relation to the group (n.d.). It is indisputable that both the therapist and the group members struggle with the unique relationship dynamics that group therapy offers, but disclosure can be used as a limited technique in joining, as long as the facilitator presents themselves more generically, being sure to keep a position of power and greater responsibility than that of clients, while at the same time only offering enough personal disclosure to affirm and support the central concern of the client (Roberts, 2005). It is a fine act of balance; one in which the therapist can ultimately be prone to “showing their erudition in ways that highlight that they have access to education, and thus power” (Roberts, 2005, p. 53). This awareness becomes very important when dealing with clients from various backgrounds, cultures, socio-economic status and ethnicity. Transference, according to Bion (2005) is a mutual dynamic that exists characteristically within comradeship and is seen as the normal development between client and therapist present in the group milieu (Walters, 2009). Freud first identified transference as an attitude towards the FOUNDATIONS OF GROUP THERAPY 8 therapist that is brought about through ‘transferred’ earlier attitudes towards important figures in the client’s life (Yalom & Leszcz, 2005). Freud also stated that if used properly, this transference could be the therapists’ most effective tool, and therefore the ability to analyze this phenomenon is of utmost importance to the therapist, along with interpreting it in a manner that clarifies some aspect of the transference (Yalom & Leszcz, 2005). Markin posits that Freud also viewed transference as a prototype of sorts that shapes subsequent relationships: group members then see all other members similarly as they assimilate others into the pre-existing template adopted by the perceiver’s perceptions (2009). A therapist can help group members to then explore and work through transference reactions to one another and in turn create a corrective and more relational experience (Markin, 2009). Pointedly, Markin states that psychodynamic theory predicts “that resolving member transference leads to clinical improvement” (2009, p. 320). As a group facilitator, a task related to transference would then be to sense how the transference in the group might differ for each of the members in the group who perhaps have a different diagnosis (Markin, 2009). It is ultimately this ‘working through’ of transference that initiates changes among group members, as touted by Markin, and lead the group to successful completion of its therapeutic goal (2009). Conclusively, there are many complex phases and stages involved in group therapy and it is the conglomeration of these such as self-awareness, transparency, knowledge of the phases of group development, understanding of what constitutes healthy group cohesion and a thorough understanding and broad range of skills in the basic tasks of facilitating a group that lead to a successful group experience. As a facilitator, lifelong learning and understanding of underlying group theories, models and therapist role playing all offer opportunity to hone the skills and sensitivity needed to run a successful group. FOUNDATIONS OF GROUP THERAPY 9 References Crowe, T. P., & Grenyer, B. F. (2008). Is therapist alliance or whole group cohesion more influential in group psychotherapy outcomes? Clinical Psychology and Psychotherapy, 15, 239-246. http://dx.doi.org/10.1002/cpp.583 Dovidio, J. F., Saguy, T., & Shnabel, N. (2009). Cooperation and conflict within groups: Bridging intragroup and intergroup processes. Journal of Social Issues, 65(2), 429-449. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=pbh&AN=37559635&site=ehost -live Kearney-Nunnery, R. (2012). Working with groups. In Advancing your career: Concepts in professional nursing (5th ed., pp. 39-53). New York, NY: F. A. Davis Company. Markin, R. D. (2009, December). Exploring a method for transference assessment in group therapy using the social relations model: suggestions for future research. The Journal for Specialists in Group Work, 34(4), 307-325. http://dx.doi.org/10.1080/01933920903219086 Roberts, J. (2005). Transparency and self-disclosure in family therapy: Dangers and possibilities. Family Process, 44(1), 45-63. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=pbh&AN=16061917&site=ehost -live Tuckman, B. W., & Jensen, M. C. (1977). Stages of small-group development revisited. Group & Organization Studies, 21(4), 419-427. Retrieved from http://www.freewebs.com/group-management/BruceTuckman(1).pdf FOUNDATIONS OF GROUP THERAPY 10 Walters, D. A. (2009, May). Transference and countertransference as existential themes in the psychoanalytic theory of W. R. Bion. Pscyhodynamic Practice, 15(2), 161-172. http://dx.doi.org/10.1080/14753630902811367 Yalom, I. D., & Leszcz, M. (2005). The theory and practice of group psychotherapy (5th ed.). New York, NY: Basic Books. Yalom, I. (n.d.). Chapter 5: Therapist basic tasks [Lecture notes]. Retrieved from http://psychologyforyouandme.com/LECTURES/Group%20therapy/Chapter%205%20ne w%20design%20and%20modified.ppt Grade Graded on Graded by 57.60 / 60.00 Saturday, 24 August 2013, 8:59 AM Debbie McCreedy 1) Write a 2,000 word essay which analyses some of the concepts, theories and practices of group work within mental health care. The essay is worth 60% of your final grade. 2) Format to APA standards including a title page, an abstract and a reference list. Feedback comments 3) A minimum of five references is required. Must be peer reviewed references.(Textbook not included although you may use as an additional reference) 4) Please focus on a minimum of three to a maximum of five concepts, theories and practice of group work within mental health care" that we have focused on during the weeks of this course prior to the essay being due. These include: Session One: Therapeutic Factors FOUNDATIONS OF GROUP THERAPY Session Two: Interpersonal Learning Session Three: Group Cohesiveness Session Four: Client Experiences of Therapeutic Groups Session Five: Basic Tasks for the Therapist (group facilitator) Session Six: Stages of Group Development Session Seven: Working in the ‘Here and Now’. Session Eight: Transference and Transparency Session Nine: The Selection of Group Participants Session Ten: Creation of the Group APA and Use of References 3/5 Grammar, syntax, sentence structure 8 /10 Width of Reading 10 /10 Relevant Material 25/25 Critical Thinking 25 /25 Coverage of Major Issues 25/25 Total Mark 96 /100 57.6 /60 DMcCreedy PSYN 203-3 WIGS 11